Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Microsoft word - mjaart.doc
The emergence of a clinical process: ‘Lifestyle medicine’ as a structured approach to the management of chronic disease.
Garry Egger,1 Andrew Binns,2 Stephen Rossner 3 1 Garry Egger, MPH, PhD, Director; and Adjunct Professor Health
Sciences, Southern Cross University, Lismore, NSW Centre for Health Promotion and Research, Sydney, NSW. 2. Andrew Binns AM BSc MBBS DROCG DA FACRRM; General Practitioner Lismore NSW and Adjunct Professor Health Sciences, Southern Cross University, Lismore, NSW. 3. Stephan Rossner MD PhD, Professor of Health Behaviour Research, Karolinska Institute, Stockholm, Sweden and Director, Obesity Unit at the Karolinska.
Correspondence: [email protected] Conflicts of Interest: Garry Egger co-ordinates and Andrew Binns has contributed to a
Post Graduate Masters in Clinical sciences program (Lifestyle-Medicine) through
Word Count: Abstract (74); Main Copy (1250) Tables (1); Figures (1) Cartoon (optional . Abstract
Chronic diseases with a lifestyle-based aetiology currently make up a significant
proportion of primary care consultations, but management often falls between the
demands of public and clinical health. A modified clinical approach, based around the
concept of ‘lifestyle medicine’ helps fill the gap by adding behavioural, motivational and
environmental skills to conventional medical practice. When used in a multi-disciplinary
setting, lifestyle medicine offers potential cost and effectiveness benefits, which are
Introduction
Around 60-70% of all visits to primary care in developed countries now have a lifestyle-
based (and hence preventive) aetiology.,1 and while lip service is often given to
prevention, 2 governments of all persuasions have largely chosen to ignore the funding of
real preventive action. Hence, while not giving up on Rose’s3 epidemiological dictum
that “small changes in large populations are likely to be more effective than large changes
in small numbers”, it is evident that a different way of managing modern chronic diseases
is called for. This needs to bridge the gap between public health, with its preventive and
population orientation, and clinical practice, with its treatment and patient-centred scope.
The advent of a modified clinical discipline, based around the concept of ‘lifestyle
medicine’, offers promise for doing this.
What is Lifestyle Medicine?
We have defined lifestyle medicine as: ‘the application of environmental, behavioural, medical and motivation principles to the management of lifestyle-related health problems in a clinical setting.’ 4 It involves the therapeutic use of lifestyle interventions in the
management of (predominantly chronic) disease at all levels. This is not meant as an
alternative to conventional clinical practice, but as a means of adding potency to evolving
practice needs. Initially developed in the US, 5 lifestyle medicine currently has specialist
post-graduate medical training in at least three US Universities (Harvard, University of
Florida and Loma Linda), a specialist association, and a journal.6 The advent of the
Enhanced Primary Care (EPC) system within the Australian health care system7 allows a
wider canvas than the US situation, embracing as it does the 13 allied health disciplines,
as well as GPs, eligible for Medicare benefits in managing chronic disease. While not
without its difficulties, 8 the EPC system is evolving into an effective means of dealing
with chronic diseases which do not easily remit under conventional pharmaco-medical
management, and which have largely arisen as collateral damage in the battle for
economic well-being. 9 Examining the reasons for this, makes the need for an altered
Defining Real Causality
A lifestyle medicine approach is largely a consequence of a more deductive style of
epidemiological analysis than is often used in clinical practice. In Figure 1 for example, it
can be seen that chronic diseases have risk factors and markers, which are often the focus
of clinical intervention. However, these markers have causes, which, as shown in Figure
1 can be proximal, medial and distal to the disease. To deal with a risk factor, or marker
alone as a ‘cause’ of chronic disease in this light, is akin to managing influenza by
prescribing tissues. Hence pharmaco-medical treatments for chronic, lifestyle-based
disease, while necessary and important, should not be expected to fully address the
problem. A more comprehensive approach would consider risk factors, as well as all
levels of causality, resulting ultimately in the use of a combination of clinical and public
health approaches, which may not always seem intuitive. For example, a recent
suggestion that an environmental approach to obesity addressing fossil fuel use in
transport as a substitute for personal energy use, while not ignoring the benefits of
personal weight loss programs at the clinical level, might reduce population levels of
obesity, as well as addressing environmental issues like climate change. 10 Several large-
scale prospective studies have now shown the benefits of lifestyle change in preventing
progression from pre-diabetes to Type 2 diabetes, 11,12,13. with effects lasting for up to 20
years.12 Cost effectiveness has also been demonstrated. 13
Processes in Lifestyle medicine
In concentrating on levels of causality in lifestyle medicine, differences in orientation to a
conventional clinical approach become clear, as shown in table 1. In particular there is a
greater requirement for the patient to be more active in his or her own care and, because
of the (often behavioural and emotional) ‘cost’ and commitment required to do this, a
greater need for an understanding and application of motivational principles, and
utilisation of the expertise of other disciplines by the co-ordinating clinician. Ironically,
there is little in the medical literature, or at medical conferences, to assist in
understanding practical approaches to motivating patients. Funded research programs are
still heavily weighted in favour of pharmacological solutions. Motivational interviewing15
Medication, under the lifestyle medicine paradigm is also seen more as an adjunct, rather
than an ‘end treatment’ in care, with side-effects recognised as part of the outcome.
Erectile dysfunction from anti-depressant medication in a middle age male for example,
can potentially exacerbate the problem. Hence this should be weighed against the
possibility of a lifestyle-change option such as exercise, for which a strong evidence base
It is also apparent that many lifestyle behaviours causing chronic disease are closely
linked in vicious cycles, and that an underlying cause may be the low-grade systemic
inflammation (‘metaflamation’) now identified as being associated with lifestyle-related
diseases. 17 Inadequate sleep for example can lead to fatigue; fatigue to inactivity;
inactivity to poor, or over-nutrition , and all these can exacerbate obesity and depression,
leading to the metabolic syndrome, Type 2 diabetes, sex and mood problems, and
potential heart disease. Medication can help manage this but, as discussed above, may
also cause counter-productive side-effects such as weight gain, exercise induced
myopathy, 18 and sexual dysfunction. All of this – the predisposing factors, cause, disease
and treatment – make up the practice of lifestyle medicine, which, in a rationally
balanced political health world, would be supported in hand-to-hand combat by the
artillery of an effective public health barrage.
Exercise and nutrition are the ‘penicillin’ of lifestyle medicine; psychology the ‘syringe’
through which these are delivered, currently in conjunction with specialists in each area.
In contrast to population and environmental interventions, lifestyle medicine focuses on
individuals (and in some cases small groups), where interventions are typically
administered in a primary care setting. Just as in any specialised area, there is a body of
knowledge and skills that need to be mastered, all of which are unlikely to exist in one
individual. The involvement of different disciplines ensures a greater availability of these
The ambit of lifestyle medicine includes the management of obesity, sleep, mood states
(anxiety, depression), addictions, skin care, sexual behaviour, oral and auditory health,
pain, iatrogenesis, and many types of injury. Typically, each of these requires the input of
a specialist discipline (dietitian, exercise physiologist, psychologist etc). However, a new
generation of multi-disciplinary exponents emanating from vocational programs now
being offered at several Universities is likely to offer a combination of expertise in
different areas including exercise, nutrition and psychology. Such non-medical specialties
are expected to reduce the time and motivational involvement required by the general
practitioner co-ordinator of such a team, who is usually hard pushed for time to do this.
Future Developments
A non-profit Australian Lifestyle Medicine Association (ALMA), with a charter to
service all disciplines accredited under the EPC system was inaugurated in 2008.
Concurrently a set of on-line LM ‘tools’, free to practitioners and patients has been
developed (www.lifestylemedicine.net.au), and is evolving to incorporate the rapidly
developing changes in the field. Several medical schools, and public health programs, are
also looking to incorporate aspects of the discipline at the under-graduate or post-
graduate levels. Evidence to date suggests significant cost-benefits of this new approach,
however more long term prospective work is obviously required. Meanwhile, lifestyle-
related chronic diseases appear unlikely to be decreased in the near future. Hence the
prospects for a discipline of lifestyle medicine indeed appear healthy.
References
1. AIHW (Australian Institute of Health and Welfare) 2006. Chronic disease and associated risk factors, AIH&W: Canberra, Cat No. Aus PHE 81.
2. Note for example the health outcomes of the recent 2020 summit, Canberra,
3. Rose G. The Strategy of Preventive Medicine. Oxford University Press, Oxford,
4. Egger G, Binns A, Rossner S. Lifestyle Medicine. Sydney, McGraw-Hill, 2008.
5. Rippe J (ed). Lifestyle Medicine. NY Blackwell Publishing, 1999
6. American Lifestyle Medicine Association; www.ajl.sagepub.com
7. Royal Australia College of General Practitioners (RCGP). www.racgp.org.au.
8. Beilby JJ. Primary care reform using a layered approach to the Medicare Benefits
Scheme: unpredictable and unmeasured. MJA, 2007; 187 (2): 69-71.
9. Egger G. Dousing our inflammatory environments: is personal carbon trading an
option for reducing obesity – and climate change? Obes Rev,2008; doi:
10. Egger G. personal carbon trading: A potential ‘stealth’ intervention for obesity
reduction? MJA, 2007; 187: 185-187.
11. Herder C, Peltonen M, Koenig W, , et al., for the Finnish Diabetes Prevention
Study Group. Systemic Immune Mediators and Lifestyle Changes in the
Prevention of Type 2 Diabetes: Results From the Finnish Diabetes Prevention
Study. Diabetes 2006; 55:2340–6.
12. Li G, Zhang P, Wang J, et al. The long-term effect of lifestyle interventions to
prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year
follow-up study. Lancet. 2008;371(9626):1783-9.
13. Diabetes Prevention Program Research Group. Intensive Lifestyle Intervention or
Metformin on Inflammation and Coagulation in Participants With Impaired Glucose Tolerance. Diabetes. 2005; 54(5): 1566–72.
14. Galani C, Schneider H, Rutten FF. Modelling the lifetime costs and health effects
of lifestyle intervention in the prevention and treatment of obesity in Switzerland. Int J Pub Health. 2007;52(6):372-82.
15. Miller WR, Rollnick S. Motivational Interviewing: Preparing people for change.
16. Barbour KA, Edenfield TM, Blumenthal JA. Exercise as a treatment for
depression and other psychiatric disorders: a review. J Cardiopulm Rehabil Prev, 2007; 27(6): 359-67.
17. Hotamisligil GS. Inflammation and metabolic disease. Nature, 2006; 444: 860–
18.Sinzinger H, O’Grady J. Professional athletes suffering from familial
hypercholesterolaemia rarely tolerate statin treatment because of muscular problems. Brit J Clin Pharmacol, 2005; 57(4): 525-528.
Hippocrates claimed that to keep well one should simply ‘avoid too much food and too little toil’. To this we might now add “…and don’t smoke, don’t eat too much fat (or eat or drink too much in general), don’t drink too much (or too little) alcohol (while having a couple of alcohol free days a week), try not to get anxious or depressed, get just the right amount of stress, don’t do too many drugs (or all kinds), don’t have unsafe sex, eat breakfast, keep regularly active, sleep well and for long enough, do some stretching and strength work every other day, wear sunscreen, use a moisturiser, avoid air conditioning and over-heating in bed where possible, keep the skin well hydrated, chew gum, floss regularly, and, remember, moderation in all things – including moderation!’
Traditional/Conventional Medicine Lifestyle Medicine
Patient is often a passive recipient of care
Patient is not required to make big changes
Medication is often the ‘end’ treatment
Medication may be needed but is adjunct to lifestyle change
Emphasis is on diagnosis and prescription
Emphasis is on motivation and compliance
Goal is primary/secondary/tertiary prevention
Side effects are balanced by the benefits
Side effects require consideration as part of the outcome
Referral (also) to allied health professionals
Doctor generally operates independently on Doctor is co-ordinatorof a team of health a one-to-one basis
Table 1. Differences between conventional and ‘lifestyle’ medicine approaches. (see ref Figure 1: A hierarchy of chronic disease causes (see ref 4).
T h e n e w e ng l a n d j o u r na l o f m e dic i n eH e a l t h L aw, E t h i c s , a n d H u m a n R i g h t s Ethical Considerations in Studying Drug Safety — The Institute of Medicine Report Michelle M. Mello, J.D., Ph.D., Steven N. Goodman, M.D., M.H.S., Ph.D., The tumult arising from revelations of serious ment began, some argued that the evidence of the safety risks assoc
Kongressbericht vom San Antonio Breast Cancer Symposium 2009 Dr. Ingo Bauerfeind, Landshut Chefarzt der Frauenklinik im Klinikum Landshut und Leiter und Zentrumskoordinator des interdisziplinären Brustzentrums Landshut Email: [email protected] Traditionell fand vom 09. 12. bis zum 13.12. 2009 in San Antonio das Brustkrebs-Symposium statt. Trotz Finanzkrise fanden
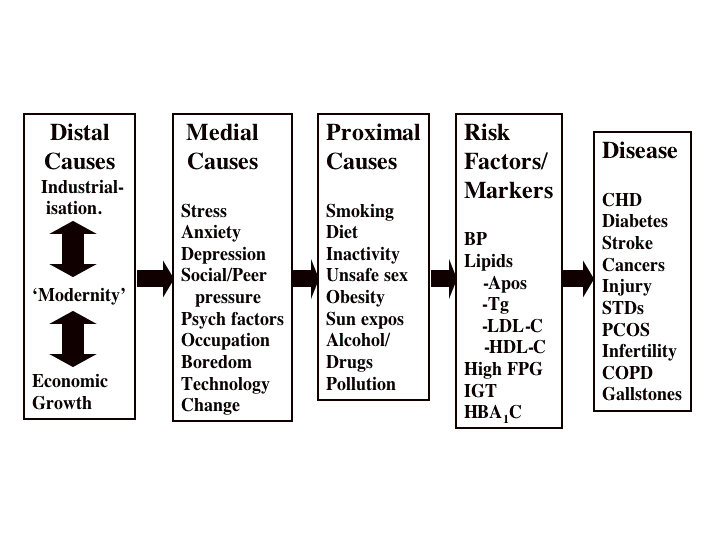
 Figure 1: A hierarchy of chronic disease causes (see ref 4).
Figure 1: A hierarchy of chronic disease causes (see ref 4).