SECTION TWO Current Treatments LINKS TO: Section One: Parkinson's Disease | Section Three: Starting Treatment | Section Four: Glossary LINKS TO: Current Treatments: The Therapeutic Choices Available Medications Principles of Management Dr. Lynch's Research LINKS BACK TO: Front Page About PALS Aims and Objectives Information on PD Relationships Yoga and PD Newsletters Ask the Doctor Medications PDNS Page The Tips Page Thought for the Day
There are many options available now as regards medications, with four or five arriving on the scene in the
Brainteasers PALS Personal Pages Contact PALS
the dopamine precursors Madopar and Sinemet
COMT inhibitors such as Comtess and Tasmar (the latter has been withdrawn from the European market
dopamine agonists such as Celance, Parlodel, and newer ones such as ropinirole (Requip), pramipexole (Mirapexin).
Symmetrel (amantadine) is thought to be a dopamine releaser, and can help dyskinesias. If you are taking Sinemet or Madopar and you start to get dyskinesias, adding Symmetrel can sometimes help to settle things down.
the available MAOI is Eldepryl (Selegilene)
Artane is the anticholinergic available here
muscle relaxants can help with muscle rigidity
glutamate (NMDA) antagonists such as dextromethorphan, are anti-dyskinetic drugs
antidepressants are very important. Some people with PD get very depressed and miserable, and should be treated for it. When dopamine levels are low in the brain, this can lead to depression, as dopamine is very important for the mood and personality areas of the brain. It is not uncommon for us
to see depression in people with Parkinson's, and depression is often seen even two or three years prior to diagnosis with PD.
There are more drugs coming on board, and we would expect another five or six in the next few years. The choice for patients is increasing, so if one drug doesn't work or doesn't suit, another one may.
Surgery - An Overview
Before any surgery for PD had been done, James Parkinson, after whom PD has been named, noticed that a stroke patient had tremor relieved on the side opposite to a stroke. In 1939, a Dr. Russell Meyers in New York, performed open brain surgery for PD (not the current stereotactic surgery), with benefit in about 6% of patients, but there was a high rate of mortality, in the region of 10% to 15%.
In the 1950s, Dr. Leskell in Sweden, performed Postero-Ventral Pallidotomies, and reported quite good benefit in about 80% of patients. With the arrival of Sinemet in the 1960s, surgery was in general stopped, although Dr. Leskell continued with the operations. By the late 1970s, it had become apparent that, while Sinemet worked well, its eventual side-effects were hard to control. Dr. Leskell's student, Dr. Laitenen continued with operations starting in the mid-eighties. There was a growing realisation that these operations worked, particularly for dyskinesias, and by the 1990s, pallidotomies were performed worldwide.
We are not yet doing these operations in Ireland. The equipment has arrived, except for one machine, a microelectrode recording system, which is still being held up in Europe, and without which the stereotactic system cannot be fully used. Mr. Pidgeon and I have a Movement Disorder Clinic in Beaumont, and we now have a list of patients whom we have
Before going any further, I should mention that, if anyone comes to see me about having surgery for PD, I usually throw barriers in their way. I have to be certain that they have fully explored all the medical aspects. It's not something to be rushed at recklessly.
There have been quite a lot of holes put in brains over the years to try and get the tremor under control. At the turn of the century, they tried operating right at the top of the motor cortex and doing incisions up there to see if it would help. Some patients reported benefit, but many patients had a stroke.
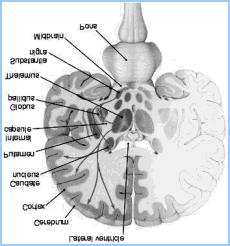
Clumps of nuclei deep in the brain are responsible for controlling automatic movement. There is a very complicated system in the brain, of different pathways, of communications back and forth, that control movement. It is known that, in Parkinson's Disease, the Pallidum gets overactive, and it is thought that knocking out that system might restore a balance. This is a very simplified explanation as the whole system is
1. Pallidotomy
In this operation, a hole (or lesion) is burned in the Globus Pallidus, and seems to work. The Globus Pallidus gets overactive in PD, but it is not known why exactly the operation works.
patients should have late-stage PD, should be disabled by "off" symptoms, and have asymmetrical dyskinesia.
The position of the lesion is critical, size less so except for risks of complications.
The recommended lesion site should be as close to the optic tract as possible.
Effects of a Pallidotomy
does not return the Parkinson's patient to mild PD
it attenuates levodopa-induced dyskinesias
results in mild improvement in "off" states, but with no improvement in "ons"
Possible Complications of a Pallidotomy
Between 1% and 2% suffer a stroke, if a small blood vessel is hit during the operation, which can happen
Neuropsychological Complications It is interesting to do a neuropsychological analysis before and after one of these operations, as there are changes. It has been noted that some people develop emotional debility and decision -making problems. The other thing to emphasize is that you should not operate if people have cognitive problems such as forgetfulness, because by operating you can make a slight problem worse. People with cognitive problems have been operated on, and have taken weeks to return to their normal cognitive state. There are exceptions to that, of course. Medications can cause forgetfulness and confusion, so you have to determine if the confusion is medication-based. Outstanding Issues for Pallidotomies
How long does the positive benefit last? Follow-ups have only been done now for about five years. Will the patient need a top-up in about ten
Will having the operation complicate any newer treatments that may come along?
Why do axial symptoms (e.g., balance) not respond?
Progressive Supernuclear Palsy (PSP) does not respond. Why not?
2. Thalamotomy
This is a similar operation, but with the lesion placed instead in the Thalamus. This operation is good for controlling tremor, with an 80% to 90% improvement in the tremor of PD, or in Benign Essential Tremor. The same risks of complications exist, as with the other operations, in 1 to 2% of people.
We should be doing some of these this year, providing the remaining equipment arrives.3. Deep Brain Stimulation of the Sub-Thalamic Nucleus
Rather than burning a lesion, in this operation, a stimulator is inserted which is then connected to a pacemaker. There have been dramatic videos made of the results of this operation. When you switch the pacemaker on, the tremor and stiffness go away - it does work. It is a nice procedure, but the risks are the same as in the other operations, and the Sub-Thalamic Nucleus is a tricky area to get into. So you don't operate on someone with cognitive deficits or on someone who has more complicated syndromes than Parkinson's Disease.
This operation is more expensive, about £10,000. The Health Board will pay for these operations in another EU country, upon referral by a neurologist. The battery needs to be replaced every three to five years. On the positive side, there is no permanent damage to the brain.
I haven't yet sent anyone away for a stimulator. The group that I think are the best at it today are the surgical group led by Professor Benabid in Grenoble. It's a long procedure. You are sitting on the table for about twelve hours, which is a long time to wait, and you can feel quite uncomfortable. Also, the neurologist can spend up to sixty hours trying to ensure that the stimulator goes in the right place.
That's a real problem for us neurologists in Ireland - there are only eleven of us. As you all know, it can be a problem getting to see a neurologist here, as there are too few of us. Ireland actually has the lowest numbers of neurologists per head of the population in the whole of Europe! We have written to the Department of Health to advise that there should be at least forty neurologists in the country within the next few years.
So this procedure, from the biological point of view, is a nice one because you are not doing any damage.
Possible Complications Positive Results
"Off" periods are reduced from occurring for 25% to 50% of the day, to between 1% and 25% of the day.
The daily amount of Sinemet or Madopar taken may be reduced by up to 50%, resulting in a similar level of reduction in the incidence of dyskinesias.
The Sub-Thalamic Stimulation, while only about a year old, gives impressive results. Stimulation can also be done in the Globus Pallidus, but it is not clear whether it will be quite as good.The following are some other procedures that may come on board in the future: 4. Gamma Knife Surgery
A cobalt radioactive probe is used to burn a hole, with no surgery. Some improvement has been reported using this technique, but it is not as accurate as in the more established operations. So, while there is no risk of stroke with Gamma Knife Surgery, your results may not be as good.
5. Other Surgical Techniques
Transplantation of foetal cells - better results obtained in younger patients.
In one trial done, with a group of forty patients, half had foetal cells implanted, and half had sham operations. After a year, those patients who had had sham operations were offered the real thing. The problem of course is the ethics of performing sham operations.
Genetically modified specific cultured cell lines (fibroblasts, glial or neuronal cells)
Trophic agents, e.g., GMI-ganglioside or GDNF (Glial -Derived Neurotrophic Factor).
The latter (GDNF) hasn't worked in trials on motor neurone patients, so I am somewhat skeptical about their potential for PD patients.Alternative Therapies
Electroconvulsive shock therapy for depression and parkinsonian motor symptoms provides short-term improvement.
Transmagnetic stimulation yields short-term improvement also.
This is a more humane way of providing treatment. We don't have one in Ireland yet, but are hoping to get one in the Mater. Rather than using electrical shocks, you can use magnetism to stimulate parts of the brain. In some studies on PD, it has been shown to help some of the stiffness and soreness in the short term.
Section One: Parkinson's Disease | Section Three: Starting Treatment | Section Four: Glossary
About PALS | Parkinson's Disease | Ask the Doctor | Relationships
Yoga and PD | News | Newsletters | Brainteasers | PALS Personal Pages | Email PALS
VYDAC® Columns for USP and Pharmaceutical Analyses The VYDAC SELECTAPORE™ is recommended for USP analyses. The Penicillin V contributes stability and long column life. analysis. Variations in selectivity based onThe specially treated base silica minimizestailing for alkaline analytes, and the 300 Åpore size provides uniform surface accessfor large multi-ring molecules. Performance
Otras parasitosis Hidatidosis o Echinococosis ( Echinococcus granulosus ) • Etiopatogenia : gusano parásito intestinal de los perros que se transmite a los humanos a través de las heces caninas. No se transmite de persona a persona. • Clínica : afectación primordial hepática con 3% de quistes renales de crecimiento lento que suelen requerir cirugía. La rotura del qui

 SECTION TWO
SECTION TWO 
 to see depression in people with Parkinson's, and depression is often seen even two or three years prior to diagnosis with PD.
There are more drugs coming on board, and we would expect another five or six in the next few years. The choice for patients is increasing, so if one drug doesn't work or doesn't suit, another one may.
Surgery - An Overview
to see depression in people with Parkinson's, and depression is often seen even two or three years prior to diagnosis with PD.
There are more drugs coming on board, and we would expect another five or six in the next few years. The choice for patients is increasing, so if one drug doesn't work or doesn't suit, another one may.
Surgery - An Overview  the brain. In some studies on PD, it has been shown to help some of the stiffness and soreness in the short term.
Section One: Parkinson's Disease | Section Three: Starting Treatment | Section Four: Glossary
About PALS | Parkinson's Disease | Ask the Doctor | Relationships
Yoga and PD | News | Newsletters | Brainteasers | PALS Personal Pages | Email PALS
the brain. In some studies on PD, it has been shown to help some of the stiffness and soreness in the short term.
Section One: Parkinson's Disease | Section Three: Starting Treatment | Section Four: Glossary
About PALS | Parkinson's Disease | Ask the Doctor | Relationships
Yoga and PD | News | Newsletters | Brainteasers | PALS Personal Pages | Email PALS