Alcohol & Alcoholism Vol. 36, No. 5, pp. 419–425, 2001
NALTREXONE VERSUS ACAMPROSATE: ONE YEAR FOLLOW-UP OF ALCOHOL
G. RUBIO*, M. A. JIMÉNEZ-ARRIERO, G. PONCE and T. PALOMO
Psychiatric Service, ‘12 de Octubre’ University Hospital, Madrid, Spain
(Received 29 December 2000; in revised form 16 March 2001; accepted 2 April 2001)
Abstract — Naltrexone and acamprosate reduce relapse in alcohol dependence. They have not yet been compared in a published trial. The aim of this study was to compare the efficacy of these compounds in conditions similar to those in routine clinical practice. Random allocation to a year of treatment with naltrexone (50 mg/day) or acamprosate (1665–1998 mg/day) was made in 157 recently detoxified alcohol-dependent men with moderate dependence (evaluated using the Addictions Severity Index and Severity of Alcohol Dependence Scale). All were patients whom a member of the family would accompany regularly to appointments. Alcohol consumption, craving and adverse events were recorded weekly for the first 3 months, and then bi-weekly, by the treating psychiatrist who was not blinded. At 3-monthly intervals, investigators who were blinded to the treatment documented patients’ alcohol consumption based on patients’ accounts, information given by the psychiatrists when necessary, and reports from patients’ families. Serum gamma-glutamyltransferase (GGT) was also measured. Efforts were made to sustain the blindness of the investigators. The same investigator did not assess the same patient twice. The integrity of the blindness was not checked. There was no difference between treatments in mean time to first drink (naltrexone 44 days, acamprosate 39 days) but the time to first relapse (five or more drinks in a day) was 63 days (naltrexone) versus 42 days (acamprosate) (P = 0.02). At the end of 1 year, 41% receiving naltrexone and 17% receiving acamprosate had not relapsed (P = 0.0009). The cumulative number of days of abstinence was significantly greater, and the number of drinks consumed at one time and severity of craving were significantly less, in the naltrexone group compared to the acamprosate group, as was the percentage of heavy drinking days (P = 0.038). More patients in the acamprosate than the naltrexone group were commenced on disulfiram during the study. Naltrexone patients attended significantly more group therapy sessions, though this could not explain their better outcome. There were non-significant trends for the naltrexone group to comply better with medication, to stay in the study longer, and to show greater improvement over baseline in serum GGT.
the time to relapse, to reduce the number of days of con-sumption and to augment the abstinence period (Pelc et al.,
Alcoholism is an important and difficult problem from several
1992; Ladewig et al., 1993; Paille et al., 1995; Sass et al.,
public health perspectives. For a long time, pharmacological
1996; Geerlings et al., 1997; Poldrugo, 1997; Besson et al., 1998;
treatments have been limited mainly to the detoxification period
Tempesta et al., 2000). However, not all the studies confirm
exclusively, and to the use of aversive drugs over the rehabilita-
its efficacy compared to placebo (Chick et al., 2000a). This
tion period (incorporating the time and process during which
compound modulates the GABA-ergic transmission and
‘normal’ levels of intake are attained and maintained). In the
decreases postsynaptic potentials in the neocortex, possibly
last decade, naltrexone and acamprosate have been proposed
via its action on NMDA (N-methyl-D-aspartate) receptors.
for use in the treatment of alcohol dependence.
Hypotheses have been drawn up concerning its actions on
Naltrexone is an opioid receptor antagonist, with a verified
calcium channels as well as on the NMDA receptors reducing
efficacy for the reduction of euphoria, alcohol intake and relapse
conditioned alcohol-withdrawal craving (Littleton, 1995).
risk by alcohol-dependent or -misusing individuals (Volpicelli
The aim of this study was to demonstrate the efficacy and
et al., 1992, 1995a,b, 1997; O’Malley et al., 1992; Anton et al.,
treatment compliance of naltrexone compared to acamprosate
1999; Chick et al., 2000b). These actions seem to be mediated
in typical treatment conditions for these patients. An open
by the property to block opiate receptors (Ulm et al., 1995),
randomized trial has been chosen for two reasons: (1) this is
not least in forebrain areas. This antagonism appears to inhibit
the experimental situation most similar to daily clinical practice;
the actions of endogenous opioids, released because of alcohol
(2) if a double-blind trial had been carried out, both drugs
intake, upon the mesolimbic pathway, which would otherwise
would have to be administered in three doses per day (because
produce a rise in dopamine (DA) in the accumbens nuclei
of the pharmacokinetics of acamprosate and manufacturer’s
(Benjamin et al., 1993; Valenzuela and Harris, 1997; Catafau
recommendations). However, taking into account the resist-
et al., 1999). Naltrexone efficacy has been demonstrated in
ance to treatment compliance in these patients, especially in
short-term double-blind studies (6–12 weeks) (O’Malley et al.,
the medium and long-term, a double-blind trial in which the
1992; Volpicelli et al., 1992, 1995a, 1997; Anton et al., 1999;
medication was administered three times a day would place
Chick et al., 2000b). However, from the available evidence,
naltrexone at a disadvantage since this drug is usually given in
naltrexone efficacy has not yet been verified in long-term
Long-term efficacy studies (6–12 months) have been carried
out, however, on acamprosate, calcium acetyl homotaurinate,
a drug marketed in Europe. This has been shown to increase
This was a randomized 12-month single-blind trial of
*Author to whom correspondence should be addressed at: Servicio dePsiquiatría, Hospital Universitario 12 de Octubre, Avda, Córdoba s/n. 28041,
naltrexone versus acamprosate. The treatment conditions were
as similar as possible to daily clinical practice.
The participants were alcohol-dependent males who had
were ‘open’ groups. Therapy was less structured than in classical
requested detoxification in the Addictive Behaviour Unit of
relapse prevention programmes. Basic relapse prevention was
‘Doce de Octubre Hospital’. Inclusion criteria were as follows:
tackled (dealing with situations of risk, craving and negative
(1) male gender aged between 18 and 65 years; (2) meeting
emotional states). Abstinence was positively reinforced.
DSM-III-R criteria for alcohol-dependence (American Psy-
Patients also received symptom-directed pharmacological treat-
chiatric Association, 1987); (3) having a stable family environ-
ment for complaints, such as anxiety, depression, insomnia,
ment so that the family can help with treatment compliance
etc., when these symptoms presented during follow-up. If
and provide information during follow-up visits. Exclusion
anxiety or depression emerged, sertraline could be prescribed
criteria were: (1) presence of another substance use disorder
(100–200 mg/day), and for insomnia patients were given hydroxy-
(with the exception of nicotine); (2) presence of another psy-
zine, an H receptor antagonist of the piperazine family used
chiatric disorder diagnosed by SCID for DSM-III-R (SCID);
as a hypnotic (50–100 mg/night). In cases of relapses which
(3) a medical condition which could hinder treatment com-
were difficult to control pharmacologically or psychothera-
pliance; (4) impaired liver function [an aspartate aminotrans-
peutically, disulfiram was added to the treatment until the
ferase (AST) or alanine aminotransferase (ALT) value more than
relapse was fully over (2–3 weeks).
three times normal values]; (5) previous treatment withnaltrexone or acamprosate.
After completing detoxification, in the hospital or as an out-
Study data on outcome were collected by investigators
patient, the subjects were informed about the study objectives.
(at 3, 6 and 12 months) who were blind to the drug taken by
They were informed about the two pharmacological treatments,
the patients. They used the following sources of data: (1) the
naltrexone or acamprosate, elective treatments at the time of
patient himself, who was asked not to talk about the type of
the study for the treatment of alcohol-dependence, but were
medication he was receiving; (2) the psychiatrist appointed to
told that the drug they would receive would be chosen at
the case, who provided any data required from the clinical
random. They would know which drug they would receive.
records, including biochemical results, and who was requested
They were told that relapse, or not taking the prescribed
not to divulge the treatment prescribed; (3) the patient’s family
treatment punctually, would not lead to their being asked to
who provided information about drinking and any attempts by
leave the trial. However, they would be taken out of the trial if
the patient to cease the pharmacological treatment. The degree
they did not keep in touch with the investigators for more than
of concordance between data from the family and the psy-
15 days (i.e. two consecutive visits). They were also told that
chiatrists increased from 80% in the first few months to 95%
they could choose to leave the study at any time.
It was hoped that asking the family would help reduce the
bias, which could occur if the information were obtained
After signing the informed consent, participants were
only from the psychiatrist who had prescribed the treatment.
assessed with the following instruments: a structured clinical
The investigators never interviewed the same patient at the three
interview for DSM-III-R (SCID) (Spitzer et al., 1992); the
time points, since, at the end of an interview, they could have
Addiction Severity Index (ASI) (McLellan et al., 1980),
knowledge of the type of treatment the patient was receiving,
Severity of Alcohol Dependence Scale (SADS) (Rubio et al.,
which could affect future interviews with the same patient.
1998); three analogue scales to measure craving (frequency,
Patients and relatives were asked not to tell the investigator
duration and intensity) (Anton et al., 1999); and a weekly
the name of the treatment they were taking, its appearance, or
calendar in which participants recorded all alcohol consumed,
how often per day they were taking it. Information from the
so that the ‘time-line follow-back’ method could be used to
psychiatrist was to complement that obtained from patients
document the pattern of consumption during follow-up
and their families and consisted mainly of data from clinical
(Miller, 1996). The following baseline biological parameters
records and results of analyses. The main role of the psy-
were determined: serum aspartate aminotransferase (AST),
chiatrists in the study was to encourage patients to take the
alanine aminotransferase (ALT), gamma-glutamyltransferase
medication and to attend psychotherapy sessions.
(GGT), bilirubin, and carbohydrate-deficient transferrin (CDT).
After randomizing the patients (using a random numbers
table), patients received either one tablet (50 mg) per day of
The primary outcome variables were: days of accumulated
naltrexone, or six tablets (or five if of lower body weight) of
abstinence and days to first relapse (relapse is defined as the
acamprosate (i.e. 1665–1998 mg/day) divided into three doses
consumption of more than five drinks or 40 g ethanol per day).
following the manufacturer’s recommendation. Patients
Additional outcome variables were number of drinks consumed
visited their psychiatrists every 7 days (± 3 days) over the first
per week, number of drinks consumed at a time, craving,
3 months, after which they visited every 15 days, till the end
abandonment of pharmacological treatment, drop-out from the
of the study. In the event of relapse, the frequency of visits was
increased in order to help curtail the relapse and to offer thepatient assistance if required. At each visit, entries in the diary
of alcohol consumption were checked, together with craving,
Pairwise χ2- and t-tests were used to analyse differences
and whether the patient continued the treatment. Consumption
between the two therapeutic groups, naltrexone versus
and compliance data were compared with information given
acamprosate. All outcome analyses were conducted under an
intention-to-treat analysis plan, with drop-outs regarded as
Both groups of patients were offered supportive group
relapsed for the abstinence and relapse analyses. Time to
therapy, once weekly over the entire study period. The groups
relapse and time to first drink were analysed by Kaplan–Meier
NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
survival analysis. The difference in variables, such as number
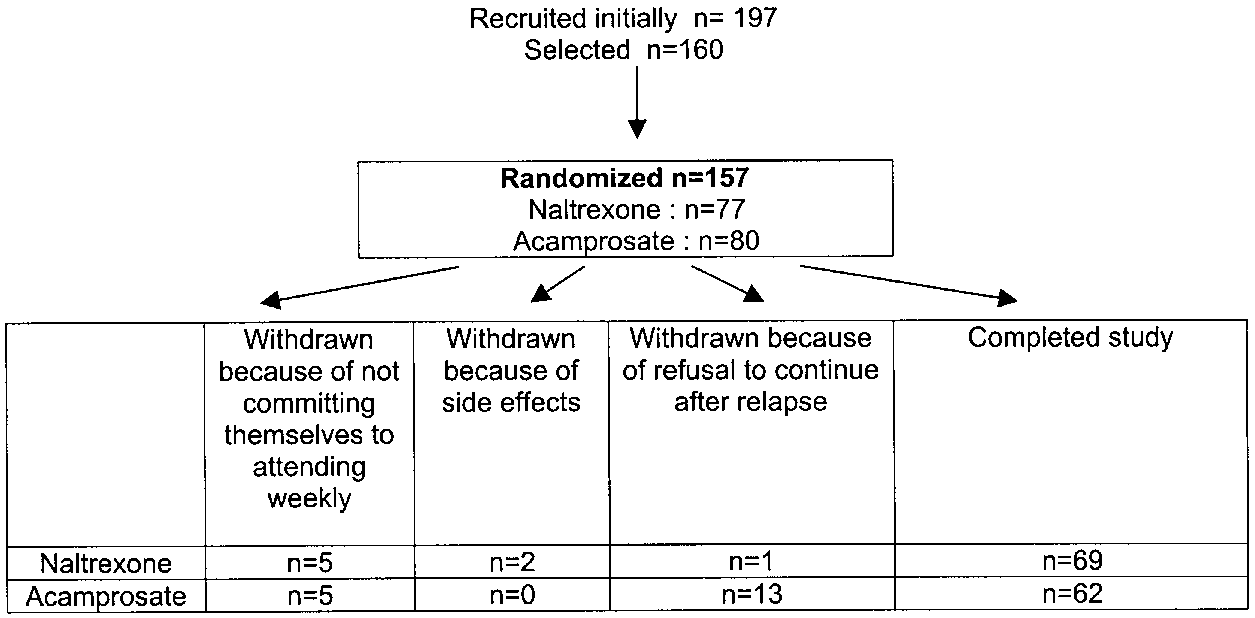
four in the 4th, one in the 7th and one in the 8th month. The
of drinks consumed per day, drinks consumed at one time or
reasons for drop-out are shown Fig. 1.
percentage of days abstinent, were analysed by analysis ofcovariance (ANCOVA), taking baseline levels as covariants,
and for drop-outs using the last observation carried forward.
At the end of the treatment year the number of abstinent
The biological drinking markers, CDT and GGT levels, were
patients in the naltrexone group was twice that in the acam-
evaluated by both repeated measures and end-point ANCOVA
prosate group and the accumulated abstinence was significantly
with baseline levels as covariants. A composite craving severity
greater in the former (Table 2). The survival until the first
score was created, as the average of the three scale scores
relapse was longer for naltrexone than acamprosate patients
(intensity, duration and frequency). Group differences were
(P = 0.02) (Fig. 2). At the end of the study, 41% of the nal-
analysed by repeated measures ANCOVA with baseline values
trexone group had not relapsed and 54% were abstinent since
on the respective scales used as covariants.
the last assessment (6 months), compared to 17 and 27%,respectively, in the group treated with acamprosate. Table 2shows further alcohol consumption data, including the drinks
consumed in a session, which was less for patients receivingnaltrexone than those receiving acamprosate. In the group treated
with naltrexone fewer patients used disulfiram. If a patient
The total number of patients from the different health centres
drank some alcohol, relapse occurred on average 12 days later
considered for inclusion in the study was 356, of whom 197
in the naltrexone group (SD = 16) whereas it occurred in the
were examined at the start of the study (Fig. 1). Of these, some
group treated with acamprosate after 6 days (SD = 8).
were not selected: 30% refused to participate; in 30% the
A survival curve of time to first alcohol consumption revealed
family could not commit themselves to accompany the patient
no significant differences between the two groups (the mean
to the Centre throughout the follow-up period; 27% had been
number of days to the first consumption was 44 for the nal-
treated previously with naltrexone or acamprosate; 25% pre-
trexone group and 39 for the acamprosate group; P = 0.34).
sented comorbidity of another disorder; and in 15% naltrexone
Regarding the composite score, severity of craving, patients
was contra-indicated because of impaired liver function. Of
receiving naltrexone had significantly lower scores over the
160 subjects selected, three then refused to participate, so
157 were submitted to the pre-treatment analysis.
Randomization gave 77 (naltrexone) and 80 (acamprosate).
Sociodemographic variables respectively were: age (mean ± SD
In the naltrexone group there was a trend towards fewer
= 43 ± 10; and mean = 44 ± 12 years), married (95 and 92%),
drop-outs, fewer attempts to abandon pharmacological treat-
employed full time (75 and 75%), secondary education
ment, more weeks of completed treatment, and greater attend-
(84 and 85%). There was no significant difference between
ance at psychotherapy support sessions. The latter reached
the groups in any of these variables. There was no significant
statistical significance. We considered the hypothesis that the
difference between the variables when related to severity of
number of days of abstinence could be related to attendance at
dependence; in both groups the severity of dependence meas-
therapy sessions, rather than to the use of naltrexone or acam-
ured with both the ASI and the SADS was moderate (Table 1).
prosate. To test this, we compared the mean number of days of
The average period between the last drink and the start of
abstinence at 3, 6 and 12 months follow-up, taking the number
treatment was 16 days (range 10–22).
of psychotherapy sessions as the covariant (ANCOVA). The
A total of 26 patients dropped out during the study (eight
results showed that, in the naltrexone group the mean number
naltrexone, 18 acamprosate). In the naltrexone group, two
of days of abstinence remained constant after the 3rd month,
patients dropped out in the 1st month, four in the 3rd month
whereas in the acamprosate group the mean number of days
and two in the 4th month. In the acamprosate group, two
of abstinence decreased over the follow-up period (F = 8.23,
dropped out in the 1st month, five in the 2nd, five in the 3rd,
Table 1. Severity of alcoholism, recent consumption pattern and
The GGT determinations done at 3, 6 and 12 months were
biological markers of drinking at study entry
compared with baseline levels and ANCOVA showed signifi-cant temporal improvements in the whole sample (F = 52.3,
df = 2, P < 0.0001). Table 3 shows the number of days of
heavy drinking and the mean values of GGT. There was a non-significant trend for greater improvement in GGT in the
naltrexone patients but a significant reduction in percentage ofdays of heavy drinking.
Side-effects were more common in the group receiving
naltrexone, the most important of which were: nausea (25 vs
4%, χ2 = 14.1, P = 0.0001), abdominal pain (23% vs 4%,
χ2 = 12.9, P = 0.0003), drowsiness (35 vs 2%, χ2 = 27.4,
P = 0.0000), nasal congestion (23 vs 1%, χ2 = 12, P = 0.0004),
headache (13 vs 6%, χ2 = 2.0, P = 0.15), diarrhoea (1 vs 4%,
Fisher test P = 0.3 ) and epigastric discomfort (4 vs 4%, Fisher
test P = 0.64). These side-effects gradually disappeared after
No significant group differences were detected (P > 0.05). All
comparisons were t-tests with df = 155.
Sertraline was prescribed for two patients in whom a
Naltrexone was associated with reducing relapse, achieving
depressive episode emerged, and hydroxyzine was prescribed
more days of accumulated abstinence, reducing the number of
to 16 patients because of inability to fall asleep. The distribu-
drinks consumed at any one time and reducing craving, com-
tion between treatment groups was even, although this was
pared to acamprosate. There was a trend for naltrexone to be
not the case with prescriptions for disulfiram, which was
associated with a greater retention in the treatment programme.
prescribed to significantly more patients in the acamprosate
It is difficult to compare our results with those of other studies,
group than the naltrexone group (Table 2).
since ours is the first published comparative study of these two
% subjects abstinent since last assessment (6 months)
No. of subjects who received sertraline to treat depression
No. of subjects receiving hydroxyzine to treat insomnia
Patients who tried to abandon pharmacological treatmenta
Days to first relapse (≥5 drinks per day)
No. of days abstinence (accumulated abstinence)
aThis information was provided by the family member accompanying the patient. bKaplan–Meier survival (log-rank) statistic.
NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
drinking (Anton et al., 1999). Whichever explanation, the higherdegree of control over their drinking achieved by patients treatedwith naltrexone could explain their lesser use of disulfiramand their achieving more days of abstinence and a greater useof therapy. In our opinion, this effect could be explained asfollows: the craving triggered by consumption is slightly lesswith naltrexone than with acamprosate, which enables thosetreated with naltrexone to stop drinking earlier. Since relapsesare very common in these patients, those treated with naltrexonewould be more capable of interrupting the relapse or diminishingits intensity. This would help to prevent progression in alcoholconsumption and increase the probability that the patient seekshelp from a therapist and, therefore, ultimately, curtail relapse. This is supported by the fewer absences from therapy in thenaltrexone-treated group. Since naltrexone reduces theintensity of relapse, patients attend more therapy sessions.
Fig. 2. Survival analysis to first relapse.
Although this latter effect has not been found by other authors
᭜, naltrexone; , acamprosate. *Five or more drinks per day.
(Anton et al., 1999), this could be due to the shorter durationof their studies. Finally, the increased number of attempts to
drugs. With regards to other research on naltrexone, in previous
abandon treatment with acamprosate may relate to the number
studies abstinence rates after 6 weeks were 23–62% (O’Malley
of doses required daily, and this could contribute to the smaller
et al., 1992; Volpicelli et al., 1992, 1997; Anton et al., 1999; Chick
percentage of days of abstinence achieved by these patients. et al., 2000b). The results of our study, which was four times
Anticraving effects of naltrexone were more important than
longer than the aforementioned ones, are within this range. The
those of acamprosate, although this difference could be due
levels of abstinence with acamprosate in placebo-controlled
to their different mechanisms of action and the fact that most
trials with a 1-year follow-up are between 18 and 35% (Paille
patients drank alcohol during the study period. Given that
et al., 1995; Sass et al., 1996; Whitworth et al., 1996; Besson et al.,
acamprosate probably exerts its anticraving action by reducing
1998). In our study, we recorded a rate of 17%. If we extrapo-
the intensity of the symptoms of the conditioned withdrawal
late these results, it seems that long-term treatment of patients
syndrome and naltrexone probably reduces the reinforcing
with naltrexone is more beneficial than with acamprosate.
effects of the alcohol, this difference would favour the use of
Two hypotheses could explain the benefits of naltrexone
naltrexone in patients who are likely to consume some alcohol.
seen in our study. First, it may be that naltrexone increases the
This would explain why the patients treated with naltrexone
period elapsed before the subject takes the first drink. Prolong-
reported less craving than the acamprosate group over the study
ing the abstinence period enables the learning of strategies
period (Rubio et al., 1999). It is also possible that naltrexone
taught in the support therapy and increases feelings of self-
would be more effective at reducing craving in patients with
efficacy. Second, it may be that naltrexone has an effect on
moderate dependence, in whom craving mechanisms related
control of alcohol consumption once this has already begun,
to positive reinforcement could be over-represented. Since our
resulting in a delay in relapse. This could also increase the
sample was of patients with moderate dependence, this could
The first of these hypotheses was not confirmed, because
With regards to the tolerability of both drugs, although the
the survival time to the first drink did not differentiate between
group treated with naltrexone experienced more side-effects,
treatments. In contrast, the action of naltrexone on control
these only lasted for the first 2 weeks of the study and there
of alcohol consumption is shown in the survival curve to first
was no significant difference in the rate of drop-out due to this.
relapse and in the number of drinks consumed at any one time. This effect has been described in other studies and has been
explained by a reduction in the reinforcing effects of ethanol
This was an open study, and there is the possibility that the
after drinking (O’Malley et al., 1996a,b), or by an improve-
investigators did not remain blinded. We tried to prevent the
ment in the ability to resist thoughts or cravings to continue
investigators from gaining direct information about the type of
Table 3. Percentage of days of heavy drinking and serum gamma-glutamyltransferase (GGT) from baseline to 1 year
% of days heavy drinking differed between the groups (F = 5.04; df = 1, 140; P = 0.038). GGT (mean ± SD): not significant.
pharmacological treatment taken by the patients, although it
Catafau, A. M., Etcheberrigaray, A., Pérez de los Cobos, J.,
is possible that they could have guessed the treatment from
Estorch, M., Guardia, J. and Flotats, A. (1999) Regional cerebralblood flow changes in chronic alcoholic patients induced by
the patients’ side-effects. However, this can also occur in
naltrexone challenge during detoxification. Journal of Nuclear
double-blind trials, except in studies with total integrity of the
Medicine 40, 19–24.
double-blindedness (Moncrieff and Drummond, 1997). Objective
Chick, J., Howlett, H., Morgan, M. Y., Ritson, B. and UKMAS inves-
outcome criteria are not subject to bias: in our study, GGT
tigators (2000a) United Kingdom Multicentre Acamprosate Study
(which is a helpful, but not perfect, marker of drinking) appeared
(UKMAS): a 6-month prospective study of acamprosate versusplacebo in preventing relapse after withdrawal from alcohol. Alcohol
to corroborate a better reported outcome in the naltrexone
and Alcoholism 35, 176–187.
group, but the advantage failed to reach statistical significance.
Chick, J., Anton, R., Checinski, K., Croop, R., Drummond, C., Farmer, R.,
Some of the advantages of naltrexone seen in this study
Labriola, D., Marshall, J., Moncrieff, J., Morgan, M., Peters, T.
could be explained by the fact that the participants were patients
and Ritson, B. (2000b) A multicentre, randomized, double-blind,
with moderate alcohol dependence. Impaired liver function
placebo-controlled trial of naltrexone in the treatment of alcohol dependence or abuse. Alcohol and Alcoholism 35, 587–593.
as an exclusion criterion will have ruled out some of the most
Geerlings, P. J., Ansoms, C. and van den Brink, W. (1997)
severe cases. Possibly, the latter would have responded better
Acamprosate and prevention of relapse in alcoholics. EuropeanJournal of Addiction Research 3, 129–137.
At the start of the study, the psychiatrists did not know
Ladewig, D., Knecht, Th., Lehert, P. H. and Fend, A. (1993)
Acamprosat — ein stabilisierungsfktor in der langzeitentwohnung
which pharmacological treatment would be most effective
von alkoholabhangigen. Therapeutische Umschau 50, 182–187.
and, therefore, had a similar attitude towards encouraging
Littleton, J. (1995) Acamprosate in alcohol dependence: how does it
compliance with both treatments. However, as the study pro-
work? Addiction 90, 1179–1188.
gressed and subjects treated with naltrexone appeared to have
McLellan, A. T., Luborsky, L., Woody, G. E. and O’Brien, C. P.
a better outcome, the psychiatrist may have made more effort
(1980) An improved diagnostic evaluation instrument for substanceabuse patients: the Addiction Severity Index. Journal of Nervous and
to encourage compliance with naltrexone treatment, which
Mental Disease 168, 26–33.
could, at least hypothetically, have then introduced a bias.
Miller, W. R. (1996) Form 90: A Structured Assessment Interview for
Our assessment of the degree of compliance to the
Drinking and Related Behaviors Test Manual: NIAAA Project Match
pharmacological treatment was conducted by questionnaires
Monograph Series, vol. 5, Mattson, M. E. and Marshall, L. A. eds,
corroborated by information from the family. It would have
pp. 14–22. National Institute on Alcoholism and Alcohol Abuse,Rockville, MD.
been more accurate to use a urinary marker such as riboflavin.
Moncrieff, J. and Drummond, D. C. (1997) New drug treatments for
A difficulty in extrapolating the results of this study to other
alcohol problems: a critical appraisal. Addiction 92, 939–947.
treatment settings could be that, in our study, there was a high
O’Malley, S. S., Jaffe, A. J., Chang, G., Schottenfeld, R S., Meyer, R. E.
level of family support available to patients. If this had
and Rounsaville, B. (1992) Naltrexone and coping skills therapy for alcohol dependence. Archives of General Psychiatry 49,
not been available, the retention levels, and compliance with
medication, might have been lower for both treatments, and
O’Malley, S. S., Jaffe, A. J., Rode, S. and Rounsaville, B. (1996a)
there would possibly have been no measurable difference
Experience of a ‘slip’ among alcoholics treated with naltrexone or
between them. In our opinion, further studies comparing the
placebo. American Journal of Psychiatry 153, 281–283.
efficacy of these two drugs are required in varying therapeutic
O’Malley, S. S., Jaffe, A. J., Chang, G., Rode, S., Schottenfeld, R. S.,
Meyer, R. E. and Rounsaville, B. (1996b) Six-month follow-up of
contexts in patients with different severity profiles.
naltrexone and psychotherapy for alcohol dependence. Archives of General Psychiatry 53, 217–224. Acknowledgements — We thank the Fundacion Cerebro y Mente for funding
Paille, F. M., Guelfi, J. D., Perkins, A. C., Royer, R. J., Steru, L. and
this research. This foundation is dedicated to neuroscience research. The
Parot, P. (1995) Randomised multicentre trial of acamprosate in a
funding received from this institution was used to remunerate the investigators
maintenance programme of abstinence after alcohol detoxification.
who received no other funding for this work from any other institution or
Alcohol and Alcoholism 30, 239–247.
pharmaceutical laboratory. Since this was an open study, the patients were
Pelc, Y., Le Bon, O., Verbanck, P., Lehert, P. H. and Opsomer, L.
prescribed their pharmacological treatments on National Health Service
(1992) Calcium acetyl homotaurinate for maintaining abstinence in
prescriptions from their psychiatrists. We would also like to thank the doctors
weaned alcoholic patients; a placebo controlled double-blind multi-
Roberto Rodriguez, Jesus Pascual and Jose Ramon Lopez-Trabada for collab-
centre study. In Novel Pharmacological Interventions for Alcoholism,
orating in the study and Luis Miguel Molinero for his advice on the statistical
Naranjo, C. and Sellers, E. M. (eds), pp. 348–352. Springer-Verlag,
Poldrugo, F. (1997) Acamprosate treatment in a long-term community
based alcohol rehabilitation programme. Addiction 92, 1537–1547.
Rubio, G., Urosa, B. and Santo-Domingo, J. (1998) Validación de
la escala de la intensidad de la dependencia alcohólica (EIDA). Psiquiatría Biológica 10 (Suppl. 1), 44–47.
American Psychiatric Association (1987) Diagnostic and Statistical
Rubio, G., Ponce, G., Jiménez-Arriero, M. A. and Santo-Domingo, J. Manual of Mental Disorders, 3rd edn, revised. American Psychiatric
(1999) La pérdida de control en la dependencia alcohólica:
conceptualización. Adicciones 11, 143–158.
Anton, R. F., Moak, D. H., Waid, L. R., Latham, P. K., Malcolm, R. J.
Sass, H., Soyka, M., Mann, K. and Zieglgansberger, W. (1996) Relapse
and Dias, J. K. (1999) Naltrexone and cognitive behavioral therapy for
prevention by acamprosate: results from a placebo controlled study
the treatment of outpatient alcoholics: results of a placebo-controlled
on alcohol dependence. Archives of General Psychiatry 53, 673–680.
trial. American Journal of Psychiatry 156, 1758–1764.
Spitzer, R. L., Williams, J. B. W., Gibbon, M. and First, M. B. (1992)
Benjamin, D., Grant, E. R. and Phorecky, L. (1993) Naltrexone reverses
The Structures Clinical Interview for DSM-III-R (SCID), I: History,
ethanol-induced dopamine release in the nucleus accumbens in
rationale, and description. Archives of General Psychiatry 49,
awake, freely moving rats. Brain Research 621, 137–140.
Besson, J., Aeby, F., Kasas, A., Lehert, P. and Potgieter, A. (1998)
Tempesta, E., Janiri, L., Bignamini, A., Chabac, S. and Potgieter, A.
Combined efficacy of acamprosate and disulfiram in the treatment of
(2000) Acamprosate and relapse prevention in the treatment
alcoholism: a controlled study. Alcoholism: Clinical and Experimental
of alcohol dependence: a placebo-controlled study. Alcohol andResearch 22, 573–579. Alcoholism 35, 202–209.
NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
Ulm, R. R., Volpicelli, J. R. and Volpicelli, L. A. (1995) Opiates
Volpicelli, J. R., Watson, N. T., King, A. C., Sherman, C. E.
and alcohol self-administration in animals. Journal of Clinical
and O’Brien, C. P. (1995b) Effect of naltrexone on alcohol
Psychiatry 56 (Suppl. 7), 5–14.
‘high’ in alcoholics. American Journal of Psychiatry 152,
Valenzuela, F. and Harris, A. (1997) Alcohol: neurobiology. In
Substance Abuse. A Comprehensive Textbook, 3rd edn, Lowinson,
Volpicelli, J. R., Rhines, K. C., Rhines, J. S., Volpicelli, L. A.,
J. H., Ruiz, P., Millman, R. B., Langrod, J. G. eds, pp. 119–142.
Alterman, A. I. and O’Brien, C. P. (1997) Naltrexone and alcohol
dependence. Role of subject compliance. Archives of General
Volpicelli, J. R., Alterman, A. I., Hayashida, M. and O’Brien, C. P. Psychiatry 54, 737–742.
(1992) Naltrexone in the treatment of alcohol dependence. Archives
Whitworth, A. B., Fisher, F., Lesch, O., Nimmerrichter, A.,
of General Psychiatry 49, 876–880.
Oberauer, H., Platz, T., Potgieter, A., Walter, H. and Fleischhacker,
Volpicelli, J. P., Clay, K. L., Watson, N. T. and O’Brien, C. P. (1995a)
W. W. (1996) Comparison of acamprosate and placebo in
Naltrexone in the treatment of alcoholism: predicting response to
long-term treatment of alcohol dependence. Lancet 347,
naltrexone. Journal of Clinical Psychiatry 56, 39–44.
Glaukomentwicklung – medikamentöse Prävention ist möglich S eit Jahren beklagen Ophthalmolo- Design der OHTS-Studie Studien zufolge ein vier- bis fünffach er-wäre eine solche langjährige Präventiv- zeigen, erhalten weniger als 50 % der groß angelegten Langzeitstudie in 22 kli-nischen Zentren in den USA [1,2].Sie soll- sichtsfeldausfall eine angemessene te verlässliche Daten ü
A HandstückB Blitzauslösungs-KnopfF Knöpfe zum Lösen der Lampen- kassette (links und rechts - beide gleichzeitig drücken) (nach 1500 Impulsen eine Neue einsetzen)H HandstückhalterungI GehäuseL Mit 2 Pfeilen geht die Leistung hoch, mit den Sobald Sie diesen drücken,erscheint das Licht im Handstück und das Gerät ist bereit. Vorwort Herzlichen Glückwunsch zum Kauf Ihres eigenen Haarent
 NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
survival analysis. The difference in variables, such as number
four in the 4th, one in the 7th and one in the 8th month. The
of drinks consumed per day, drinks consumed at one time or
reasons for drop-out are shown Fig. 1.
NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
survival analysis. The difference in variables, such as number
four in the 4th, one in the 7th and one in the 8th month. The
of drinks consumed per day, drinks consumed at one time or
reasons for drop-out are shown Fig. 1.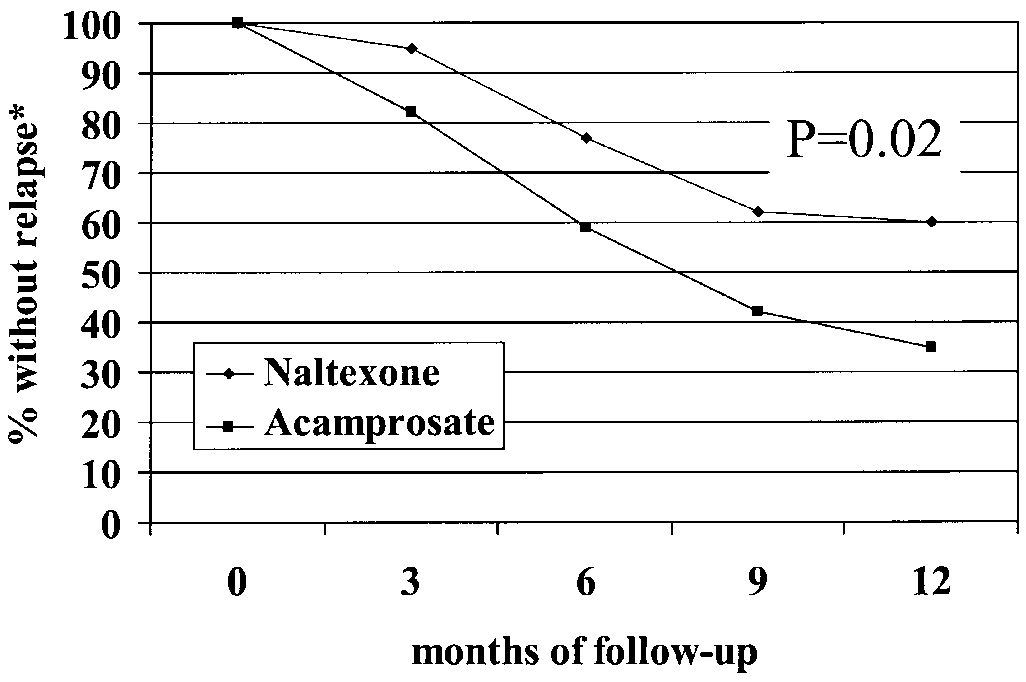 NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
drinking (Anton et al., 1999). Whichever explanation, the higherdegree of control over their drinking achieved by patients treatedwith naltrexone could explain their lesser use of disulfiramand their achieving more days of abstinence and a greater useof therapy. In our opinion, this effect could be explained asfollows: the craving triggered by consumption is slightly lesswith naltrexone than with acamprosate, which enables thosetreated with naltrexone to stop drinking earlier. Since relapsesare very common in these patients, those treated with naltrexonewould be more capable of interrupting the relapse or diminishingits intensity. This would help to prevent progression in alcoholconsumption and increase the probability that the patient seekshelp from a therapist and, therefore, ultimately, curtail relapse.
NALTREXONE VERSUS ACAMPROSATE IN ALCOHOLISM
drinking (Anton et al., 1999). Whichever explanation, the higherdegree of control over their drinking achieved by patients treatedwith naltrexone could explain their lesser use of disulfiramand their achieving more days of abstinence and a greater useof therapy. In our opinion, this effect could be explained asfollows: the craving triggered by consumption is slightly lesswith naltrexone than with acamprosate, which enables thosetreated with naltrexone to stop drinking earlier. Since relapsesare very common in these patients, those treated with naltrexonewould be more capable of interrupting the relapse or diminishingits intensity. This would help to prevent progression in alcoholconsumption and increase the probability that the patient seekshelp from a therapist and, therefore, ultimately, curtail relapse.