Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Crazyforkitties.com
Article 1 Case report
Management of the traumatic oronasal fistula in the cat with a conical silastic prosthetic device
Heloisa Justen M de Souza DVM, MSc, Ph ernanda V Amorim Datia B Corgozinho DVrio R Tavares D
1 Department of Medicine and Surgery, Veterinary Institute, Universidade Federal Rural do Rio
de Janeiro, Br 465, Km 7, Seropédica, Rio de Janeiro, RJ CEP 23890-000, Brazil
2 Cat Clinic Gatos & Gatos Vet, Av. Paranapuã 1885, Ilha do Governador, Rio de Janeiro, RJ
3 Dermatologist of Hospital da Polícia Militar de Niterói, Niterói, Rio de Janeiro, Brazil
Accepted 9 February 2004. Available online 7 January 2005.
Management of a traumatic oronasal fistula with a prosthetic device in an 8-year-old male neutered domestic shorthair cat is described. The animal had fallen from a height of three stories at the age of 1 year. The fall had resulted in a fracture of the hard palate and a split in the palatal mucosa. Two surgical attempts to close the defect had been unsuccessful and an autopolymerizable acrylic resin prosthesis had produced unsatisfactory results. The management of the chronic traumatic fistula with a conical prosthetic device was fast, easy and efficient. The device was removed and a second one was put in place after 2 years. This method would appear particularly useful for obturation of large palatal defects that have failed to heal after attempts at surgical closure and is an alternative treatment for debilitated cats which may not be candidates for longer surgical procedures.
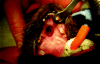
Repair of the caudal hard acquired palatal defect in the cat with a conical silastic nasal septal button. 1A. Chronic 2.2 × 1.6 cm traumatic oronasal fistula in a 7-year-old cat. 1B. The device is shaped by trimming before insertion and placed in the oronasal fistula. 1C. One piece device is positioned on opposite sides of the oronasal fistula. 1D. Prosthodontic obturation.
Article 2
http://www.ncbi.nlm.nih.gov/pubmed/17335424
Repair of oronasal fistulae using auricular cartilage grafts in five cats. Abstract OBJECTIVE:
To describe repair of chronic palatine defects in cats, with free cartilage graft harvested from either the pinna (scapha) or vertical ear canal (annular cartilage).
STUDY DESIGN: ANIMALS:
Cats (n=5) with chronic oronasal fistula.
METHODS:
Cartilage was harvested from either the scapha or annular cartilage and epithelium removed. After preparation of the edges of the palatal defect by separation of the oral and palatal mucosa circumferentially, the graft was inserted between the epithelial layers and secured without tension. The graft acted as a scaffold for migration of granulation tissue and epithelialization.
RESULTS:
Oronasal fistulae were successfully repaired in 5 cats (3 pinna grafts; 2 annular cartilage grafts); 1 cat required a second graft after the first graft was dislodged.
CONCLUSIONS:
Auricular cartilage provides a reliable framework for repair of oronasal fistulae in cats.
CLINICAL RELEVANCE:
Chronic oronasal fistulae refractory to conventional repair can be treated by use of auricular free graft (pinna or annular cartilage) without disfigurement. Use of annular cartilage to support palatal repairs offers surgeons an additional option when other methods have failed. We recommend using conchal cartilage as the initial treatment approach for repair of small oronasal fistulae in cats.
Article 3
Can Vet J. 2006 December; 47(12): 1210–1213. and/or publishing rights held by the Canadian Veterinary Medical Association Surgical repair of traumatic oronasal fistula in a domestic short-haired cat Nicola Wilson Western College of Veterinary Medicine, University of Saskatchewan, 52 Campus Drive, Saskatoon, Saskatchewan S7N 5B4 Address all correspondence and reprint requests to Dr. Wilson. Abstract A 9-month-old, spayed female domestic shorthair was presented with a suspected traumatic oronasal fistula. Two surgical attempts using mucosal advancement flaps and single layer closure failed, likely due to inadequate blood supply that was potentially exacerbated by excess tension and trauma on the graft.
A 9-month-old, spayed female domestic shorthair was referred to the Western College of Veterinary Medicine (WCVM) Small Animal Clinic for perforation of the hard palate and subsequent exposure of the nasal turbinates. The cat’s tongue had also been injured and the mandible deformed. The owner reported that the cat had been sneezing while eating since acquired as a stray at 6 wk of age. Food often came out through the cat’s nose. An oily, matted hair coat demonstrated that the cat had difficulties grooming. An episode of choking on dry cat food when the cat was 6 mo old had required emergency veterinary treatment. There was no history of other medical problems and vaccinations, excluding rabies, were current. The cat had been fed canned food (Felidae Chicken and Rice Formula; Canidae Pet Foods, San Luis Obispo, California, USA) exclusively.
On presentation, the cat was bright and alert but moderately underweight (5% to 10%) at 2.75 kg. The cat’s hair coat was dull and matted. A physical examination revealed normal heart and respiration rates, pink mucus membranes, and a slightly elevated temperature (39.6°C). A small amount of serous discharge was coming from the nostrils and mouth. On the right margin of the hard palate, against the dental arcade, there was an 0.5-cm diameter circular fistula at the level of the canine and first 3 premolar teeNasal turbinates were visible through this fistula and dried food was in the nasal passages. The rostral third of the tongue was grossly scarred and came to a point at the enIt was attached in several places to the underlying oral mucosa. The upper 1st premolar tooth was missing on the right. The mandible was shifted left, resulting in malocclusion of the jaw.
m diameter oronasal fistula at the level of the canine and 1st 3 premolar th.
rostral third of the tongue was grossly scarred and tapered to a point.
When offered food, the cat had a strong interest in eating but difficulty in prehending and ingesting food. Cleft palate was diagnosed, and due to the nature of the defect and the tongue and jaw involvement, the inciting cause was thought to be electrocution, likely the result of biting an electrical cord. Surgical treatments were discussed with the owner. Due to the size of the defect, lack of local tissues for reconstruction, unknown blood supply to the associated tissues, and lack of bony support for surgical flaps, a guarded prognosis was given.
Results from preanesthetic blood studies were unremarkable and skull radiographs revealed a shortened right ramus of the mandible, but no obvious fractures or explanations for the malocclusion. The cat was found to be negative for Feline leukemia virus and Feline immunodeficiency virus. The cat was blood-typed, in the event that blood transfusions would be needed, and found to be type AB.
Before surgery, the cat was fasted for 12 h and then pre-medicated, IM, with acepromazine (Ace Atravet; Wyeth-Ayerst, Guelph, Ontario), 0.1 mg/kg bodyweight (BW), and hydromorphone (Hydromorphone HP-10; Sabex, Quebec City, Quebec), 0.1 mg/kg BW. Thirty minutes later, a catheter was placed and anesthesia was induced with ketamine (Vetalar Ketamine Hydrochloride for INJ; Bioniche Animal Health Canada, Belleville, Ontario), 5 mg/kg BW, and valium (Diazepam Injection USP; Sabex), 0.5 mg/kg, IV. The cat was intubated and maintained on isoflurane (IsoFlor; Abbott Laboratories, Saint Laurent, Quebec) with 100% oxygen. The cat was positioned in dorsal recumbency and gauze was placed around the endotracheal tube to block fluid entering the oropharynx and airways. Three mucosal pedicle flaps were used for closure of the fistula. The 1st flap was created by incising the gingival mucosa caudal to the right canine tooth and rostral to the 2nd premolar. These incisions were extended laterally to the mucocutaneous lip margin. A 3rd incision was made along the right border of the defect and the gingival mucosa was undermined to complete the flap. A 2nd flap was created from the left side of the hard palate by twice incising the full length of the hard palate and making a 3rd incision at the rostral end of the flap. When the first 2 flaps were advanced, there was still a small hole remaining at the caudal border of the defect. A 3rd flap was created caudal to the defect to cover the remaining hole. Closure was performed in 1 layer, using 6-0 suture (PDS II Suture; Ethicon, Somerville, New Jersey, USA) in a simple, interrupted fashion at all incisional margins. During surgery, the oral mucosa was noted to be very thin and the blood supply suboptimal. The tongue was then detached from the oral mucosa and its margins debrided to improve function. Intraoperatively, the cat was administered cefazolin (Cefazolin Sodium for INJ; Novopharm, Toronto, Ontario), 22 mg/kg BW, IV, q2h.
After the repairs, an esophagostomy tube (E-tube) was placed nsure optimal nutrition and to diminish trauma to the flaps associated with eating. The position of the tube was verified radiographically. Hydromorphone, 0.05 mg/kg BW, dexamethasone (Dexamethosone 5; Vetoquinol Canada, Lavaltrie, Quebec), 0.1 mg/kg BW, and acepromazine, 0.3 mg/kg BW, were given, IV, postoperatively, and a 25-μg fentanyl patch (Duragesic; Janssen-Ortho, Markham, Ontario) was placed on the right lateral thigh. Postoperative management included lactated Ringer’s solution (Ringer Lactate INJ; Abbott Laboratories) with 20 mEqKCl (Potassium Chloride for INJ; Abbott Laboratories), IV, at 12 mL/h; amoxicillin/potassium clavunate (Clavamox liquid suspension; Pfizer, Kirkland, Quebec), 14 mg/kg BW, by E-tube for 7 d; and
meloxicam (Metacam; Boehringer Ingelheim, Burlington, Ontario), 0.2 mg/kg BW, SC, followed by 0.1 mg/kg BW, SC, q24h for 6 d.
Since the cat was underweight before the surgery, adequate postoperative nutrition was important. The cat was fed a weight management diet (Eukanuba Maximum Calorie [EMC]; Iams, Dayton, Ohio, USA), 40 mL, by E-tube, q6h, followed by warm water (20 mL). This diet was chosen for its concentrated energy content and its appropriate consistency for administration via an E-tube. The feeding dosage was determined according to the manufacturer’s instructions for a 4–8 kg cat and the maximum amount within this range was fed. This was equivalent to 336 kcal/d, or 2.2 times the basal energy requirement (BER). The BER was calculated by multiplying the cat’s weight to the power 0.75, byhe BER was found to be 150 kcal/d. Animals suffering severe burns or trauma can be fed as much as twice the BER per day to account for the additional energy required by the body during healingn the basis of this information, the cat was overfed by approximately 13% daily.
On the day after surgery, the cat was mildly dehydrated and drooling profusely. Dehydration was confirmed by an elevated refractometer reading for total solids (80 g/L; reference range, 51 to 72 g/L). Fluids were increased to twice the maintenance requirement for 2 d, until the hydration status had improved. Two days after surgery, the cat was quiet, but affectionate, and had gained 0.18 kg, so it now weighed 2.94 kg. On the 3rd day after surgery, the cat was bright and alert, but necrosis of 25% of the left lateral flap was detected. The other flaps appeared to be healthy. By day 5, the necrotic tissue had sloughed and the incisions had dehisced completely. The defect resembled the original size. Deficiency of blood supply to the left lateral flap was speculated as the reason for the graft failure.
Following the graft failure, the cat was placed on half a can of a diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition, Topeka, Kansas, USA), q8h. This diet was chosen for its concentrated energy content and high palatability. In addition, its soft texture made it easy to prehend and unlikely to cause damage to the graft. The dose was equivalent to 270 kcal/d or 1.8 times the BER. This was within the manufacturer’s recommended dose for a cat of this size and condition. The E-tube was maintained for future use. In addition, the lower parts of the mouth were rinsed with 0.05% chlorhexidine (Novaldent; Ayerst, Fort Dodge, Iowa, USA) and saline solution, q8h, to help to prevent bacterial contamination in the healing area. By 6 d after surgery, the cat’s appetite was decreased and she had lost 0.14 kg and now weighed 2.80 kg. Part of the weight loss was attributed to fluid loss, but part was attributed to decreased food intake. A weight management diet (EMC), 40 mL, q6h, was added to the feeding regimen, via the E-tube, until the cat’s appetite returned to normal. After 2 d supplementation, the cat’s appetite was good and weight remained steady around 2.77 kg, so tube feeding was discontinued.
Surgery was repeated approximately 3 wk after the initial graft breakdown. Results from the preanesthetic blood studies were again unremarkable. The cat was medicated and prepared for surgery, as previously described. For the 2nd surgery, all of the teeth remaining in the upper arcade (incisors, premolars, molars, and right canine) were extracted, in order to increase the size of buccal flaps, after blocking the infraorbital nerves bilaterally with bupivicaine (Marcaine; Abbott Laboratories), 2 mg/kg BW. The associated palatine bone was removed with a high speed burr in order to smooth the edges and thereby decrease the amount of tissue necessary to reach the defect. Three pedicle advancement flaps were used to close the defect. The first 2 flaps were created by incising the right and left palatine and buccal mucosae. First, an incision was made
where the canine tooth had been on the right and just caudal to the canine tooth on the left. Second, incisions were made rostral to where the molars had been. Third, incisions were made along the right and left margins of the defect. The incisions were extended into the buccal mucosa and the gingival and buccal mucosae were undermined to create the flaps. A 3rd advancement flap was created caudal to the defect, as previously described. Since there was inadequate tissue to do a two-layer closure without creating excessive tension, an artificial layer was created by using a piece of polypropylene mesh (Monofilament Polypropylene Mesh; Bard, Tempe, Arizona, USA) fitted under the defect. The mesh was sutured to the rostral palatine mucoperiosteum and glued (Vetbond Tissue Adhesive; 3M, St. Paul, Minnesota, USA) to the remaining palatine bone in order to provide a base to support the flaps. The flaps were then advanced and closure was performed, as previously described. The closure appeared tension-free. Cefazolin was administered, 22 mg/kg BW, IV, q2h during surgery.
After surgery, the cat had some breathing difficulties due to bleeding in the nasal passages and was monitored in the intensive care unit overnight. Butorphanol (Torbugesic; Wyeth, Saint Laurent, Quebec), 0.3 mg/kg BW, IV, q4–6h for 36h, was administered. Postoperative management included IV fluids (6% Dextran 75; Abbott Laboratories), for 2 d; ampicillin (Ampicillin Sodium for injection; Novopharm, Toronto, Ontario), 60 mg, via E-tube for 11 d; and meloxicam, 0.1 mg/kg BW, SC, q24h for 6d.
The cat was fed a diet specially formulated to increase caloric intake for speedy recovery (Clinicare Feline Liquid Diet, Abbott Laboratories), 40 mL, via E-tube, q6h, followed by warm water (5 mL), instead of the previously utilized diet. This diet was chosen on the basis of its concentrated energy content and appropriate consistency for administration via a feeding tube. The cat was fed 160 kcal/d following the 2nd surgery. This was equivalent to approximately 1.1 times the BER.
Immediately after surgery, the graft appeared intact and pink. Two days following surgery, the cat ate dry cat food ravenously. The following morning, there was some slight dehiscence on the rostral right flap, but most of the graft appeared viable and to be healing nicely. By day 4, the edges of the rostral right flap were pale gray and 25% of the flap appeared nonviable along the incision. By day 5, all incisions had dehisced and the defect was quite large, although the mesh remained in place, effectively separating the nasal and oral cavities and limiting food passage to the nose. Tube feeding was discontinued at this time and the cat was placed on the diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition), ad libitum. The E-tube was removed 9 d after surgery. Again, inadequate blood supply was the suspected cause of the graft failure, although trauma to the site from eating dry cat food likely played a role.
The cat remains in hospital. Her appetite continues to be excellent and weight steady. She is still 5% to 10% underweight. Discussion of a 3rd surgery is underway.
Traumatic oronasal fistulas occur when trauma to the skull results in destruction of the palate separating the oral and nasal cavities. Many causes of traumatic palatal defects have been described, such as chronic infection from periodontal disease, bite wounds, blunt trauma, neoplasia, and electrocutihese defects can be repaired by using various flap and prosthetic implant tecgical correction is directed to restoring normal eating and drinking ability through functional separation of the oral and nasal cavities. Due to the rich blood supply and adequate strong, elastic donor tissue in the oral cavity, large defects can be
closed successfully by using gingival mucosal flapouble-layer closures are preferred when there is adequate tissue to provide tensionless appositle-layer flap technique has also been succeIn the case of this cat, tissue was inadequate to accommodate a double-layer closure without extracting teeth, so initially a single-layer closure was attempted. The thin oral mucosa, combined with surgical trauma, likely resulted in destruction of the blood supply to the mucosal flaps and subsequent graft failure. It is also possible that a tensionless apposition was not achieved or that physical trauma to the graft contributed to failure.
Several clinicians worked on this case, resulting in disparity in feeding regimens. Ideally, the cat would have been fed 1.25 to 2 times the BER daily. This would have met the basal metabolic needs of the cat and compensated for the additional energy required to heal from the trauma of surgeryood and water would have been administered via an esophagostomy tube, with nothing being given by mouth for approximately 2 wk. This would have minimized trauma to the graft from food particles and excess tongue movement, and maintained maximal cleanliness in the oral cavity, effectively reducing the chance of infection. Energy dense, highly palatable diets with an appropriate consistency (Eukanuba Maximum Calorie and Clinicare Feline Liquid Diet) were appropriate for this purpose. Trauma associated with the oral feeding of liquids postoperatively has been implicated in graft dehiscence in the region of the hard palate is possible that the ingestion of dry cat food 2 d following the 2nd surgery contributed significantly to the failure in this case. For the 3rd surgical repair, all attempts will be made to perform a proper 2-layer closure, paying close attention to maintaining the blood supply, eliminating tension, and minimizing trauma to the incision. It may be necessary to attempt more complicated reconstruction that uses microvascular techniques in order to bring in more tissue and ensure an adequate blood supply.
The author thanks Drs. Mitch Gillick, Kathleen Linn, and Lori MacDougall for their guidance with the case, and Dr. Cindy Shmon for her advice with the manuscript. CVJ
Winner of the CVMA Pet Food Certification Nutrition Award
Nicola Wilson’s current address is Oklahoma State University, College of Veterinary Medicine, Veterinary Clinical Sciences, 1 Boren Veterinary Medical Teaching Hospital, Stillwater, Oklahoma 74078, USA.
Dr. Wilson will receive 50 free reprints of her article, courtesy of The Canadian Veterinary Journal.
References 1. Coles BH, Underwood LC. Repair of the traumatic oronasal fistula in the cat with a prosthetic acrylic implant. Vet Rec. 1988;122:359–
2. Seim HB, Willard MD. Postoperative care of the surgical patient. In: Fossum TW, ed. Small Animal Surgery. 2nd ed. St. Louis, Missouri: Mosby, 2002:71–72. 3. Griffiths LG, Sullivan M. Bilateral overlapping mucousal single-pedicle flaps for correction of soft palate defects. J Am Anim Hosp Assoc. 2001;37:183– 4. Howard DR, Davis DG, Merkley DF, Krahwinkel DJ, Schirmer RG, Brinker WO. Mucoperiosteal flap technique for cleft palate repair in dogs. J Am Vet Soc. 1974;156:352–354. 5. Luskin IR. Reconstruction of oral defects using mucogingival pedicle flaps. Clin Tech Small Anim Pract. 2000;15:251– 6. Mathews KA. Veterinary Emergency and Critical Care Manual. Guelph: Lifelearn, 1997:19–18. 7. Rickards DA. Disjunction of the upper and jaw and traumatic cleft palate. Feline Pract. 1975;2:51–52. 8. Robertson JR, Dean PW. Repair of a traumatically induced oronasal fistula in a cat with a rostral tongue flap. Vet Surg. 1987;16:164–
Springfield, Illinois – Leonard A. Sherman, Director of the Illinois Department of Professional Regulation, announced the following disciplinary actions taken by the Department during the month of March 2001. ARCHITECTURE Alexander Bernhardt, Chicago – architect license (001-014185) reprimanded and fined $1,000 for practicing on a non-renewed license. Michael Leary, Chic
J Pharm Educ Res Vol. 2, Issue No. 1, June 2011 Inorganics/bioinorganics: Biological, medicinal and pharmaceutical uses Bhupinder Singh Sekhon PCTE Institute of Pharmacy, near Baddowal Cantt, Ludhiana 142 021, India. Email:[email protected] Received May 06, 2011; Accepted May 22, 2011 ABSTRACT Metal ions function in numerous metalloenzymes, are incorporated into pharmaceuticals and



 Article 1
Article 1  Repair of the caudal hard acquired palatal defect in the cat with a conical silastic nasal septal button. 1A. Chronic 2.2 × 1.6 cm traumatic oronasal fistula in a 7-year-old cat. 1B. The device is shaped by trimming before insertion and placed in the oronasal fistula. 1C. One piece device is positioned on opposite sides of the oronasal fistula. 1D. Prosthodontic obturation.
Article 2
Repair of the caudal hard acquired palatal defect in the cat with a conical silastic nasal septal button. 1A. Chronic 2.2 × 1.6 cm traumatic oronasal fistula in a 7-year-old cat. 1B. The device is shaped by trimming before insertion and placed in the oronasal fistula. 1C. One piece device is positioned on opposite sides of the oronasal fistula. 1D. Prosthodontic obturation.
Article 2 
 Article 3
Article 3  rostral third of the tongue was grossly scarred and tapered to a point.
When offered food, the cat had a strong interest in eating but difficulty in prehending and ingesting food. Cleft palate was diagnosed, and due to the nature of the defect and the tongue and jaw involvement, the inciting cause was thought to be electrocution, likely the result of biting an electrical cord. Surgical treatments were discussed with the owner. Due to the size of the defect, lack of local tissues for reconstruction, unknown blood supply to the associated tissues, and lack of bony support for surgical flaps, a guarded prognosis was given.
Results from preanesthetic blood studies were unremarkable and skull radiographs revealed a shortened right ramus of the mandible, but no obvious fractures or explanations for the malocclusion. The cat was found to be negative for Feline leukemia virus and Feline immunodeficiency virus. The cat was blood-typed, in the event that blood transfusions would be needed, and found to be type AB.
Before surgery, the cat was fasted for 12 h and then pre-medicated, IM, with acepromazine (Ace Atravet; Wyeth-Ayerst, Guelph, Ontario), 0.1 mg/kg bodyweight (BW), and hydromorphone (Hydromorphone HP-10; Sabex, Quebec City, Quebec), 0.1 mg/kg BW. Thirty minutes later, a catheter was placed and anesthesia was induced with ketamine (Vetalar Ketamine Hydrochloride for INJ; Bioniche Animal Health Canada, Belleville, Ontario), 5 mg/kg BW, and valium (Diazepam Injection USP; Sabex), 0.5 mg/kg, IV. The cat was intubated and maintained on isoflurane (IsoFlor; Abbott Laboratories, Saint Laurent, Quebec) with 100% oxygen. The cat was positioned in dorsal recumbency and gauze was placed around the endotracheal tube to block fluid entering the oropharynx and airways. Three mucosal pedicle flaps were used for closure of the fistula. The 1st flap was created by incising the gingival mucosa caudal to the right canine tooth and rostral to the 2nd premolar. These incisions were extended laterally to the mucocutaneous lip margin. A 3rd incision was made along the right border of the defect and the gingival mucosa was undermined to complete the flap. A 2nd flap was created from the left side of the hard palate by twice incising the full length of the hard palate and making a 3rd incision at the rostral end of the flap. When the first 2 flaps were advanced, there was still a small hole remaining at the caudal border of the defect. A 3rd flap was created caudal to the defect to cover the remaining hole. Closure was performed in 1 layer, using 6-0 suture (PDS II Suture; Ethicon, Somerville, New Jersey, USA) in a simple, interrupted fashion at all incisional margins. During surgery, the oral mucosa was noted to be very thin and the blood supply suboptimal. The tongue was then detached from the oral mucosa and its margins debrided to improve function. Intraoperatively, the cat was administered cefazolin (Cefazolin Sodium for INJ; Novopharm, Toronto, Ontario), 22 mg/kg BW, IV, q2h.
After the repairs, an esophagostomy tube (E-tube) was placed nsure optimal nutrition and to diminish trauma to the flaps associated with eating. The position of the tube was verified radiographically. Hydromorphone, 0.05 mg/kg BW, dexamethasone (Dexamethosone 5; Vetoquinol Canada, Lavaltrie, Quebec), 0.1 mg/kg BW, and acepromazine, 0.3 mg/kg BW, were given, IV, postoperatively, and a 25-μg fentanyl patch (Duragesic; Janssen-Ortho, Markham, Ontario) was placed on the right lateral thigh. Postoperative management included lactated Ringer’s solution (Ringer Lactate INJ; Abbott Laboratories) with 20 mEqKCl (Potassium Chloride for INJ; Abbott Laboratories), IV, at 12 mL/h; amoxicillin/potassium clavunate (Clavamox liquid suspension; Pfizer, Kirkland, Quebec), 14 mg/kg BW, by E-tube for 7 d; and
meloxicam (Metacam; Boehringer Ingelheim, Burlington, Ontario), 0.2 mg/kg BW, SC, followed by 0.1 mg/kg BW, SC, q24h for 6 d.
Since the cat was underweight before the surgery, adequate postoperative nutrition was important. The cat was fed a weight management diet (Eukanuba Maximum Calorie [EMC]; Iams, Dayton, Ohio, USA), 40 mL, by E-tube, q6h, followed by warm water (20 mL). This diet was chosen for its concentrated energy content and its appropriate consistency for administration via an E-tube. The feeding dosage was determined according to the manufacturer’s instructions for a 4–8 kg cat and the maximum amount within this range was fed. This was equivalent to 336 kcal/d, or 2.2 times the basal energy requirement (BER). The BER was calculated by multiplying the cat’s weight to the power 0.75, byhe BER was found to be 150 kcal/d. Animals suffering severe burns or trauma can be fed as much as twice the BER per day to account for the additional energy required by the body during healingn the basis of this information, the cat was overfed by approximately 13% daily.
On the day after surgery, the cat was mildly dehydrated and drooling profusely. Dehydration was confirmed by an elevated refractometer reading for total solids (80 g/L; reference range, 51 to 72 g/L). Fluids were increased to twice the maintenance requirement for 2 d, until the hydration status had improved. Two days after surgery, the cat was quiet, but affectionate, and had gained 0.18 kg, so it now weighed 2.94 kg. On the 3rd day after surgery, the cat was bright and alert, but necrosis of 25% of the left lateral flap was detected. The other flaps appeared to be healthy. By day 5, the necrotic tissue had sloughed and the incisions had dehisced completely. The defect resembled the original size. Deficiency of blood supply to the left lateral flap was speculated as the reason for the graft failure.
Following the graft failure, the cat was placed on half a can of a diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition, Topeka, Kansas, USA), q8h. This diet was chosen for its concentrated energy content and high palatability. In addition, its soft texture made it easy to prehend and unlikely to cause damage to the graft. The dose was equivalent to 270 kcal/d or 1.8 times the BER. This was within the manufacturer’s recommended dose for a cat of this size and condition. The E-tube was maintained for future use. In addition, the lower parts of the mouth were rinsed with 0.05% chlorhexidine (Novaldent; Ayerst, Fort Dodge, Iowa, USA) and saline solution, q8h, to help to prevent bacterial contamination in the healing area. By 6 d after surgery, the cat’s appetite was decreased and she had lost 0.14 kg and now weighed 2.80 kg. Part of the weight loss was attributed to fluid loss, but part was attributed to decreased food intake. A weight management diet (EMC), 40 mL, q6h, was added to the feeding regimen, via the E-tube, until the cat’s appetite returned to normal. After 2 d supplementation, the cat’s appetite was good and weight remained steady around 2.77 kg, so tube feeding was discontinued.
Surgery was repeated approximately 3 wk after the initial graft breakdown. Results from the preanesthetic blood studies were again unremarkable. The cat was medicated and prepared for surgery, as previously described. For the 2nd surgery, all of the teeth remaining in the upper arcade (incisors, premolars, molars, and right canine) were extracted, in order to increase the size of buccal flaps, after blocking the infraorbital nerves bilaterally with bupivicaine (Marcaine; Abbott Laboratories), 2 mg/kg BW. The associated palatine bone was removed with a high speed burr in order to smooth the edges and thereby decrease the amount of tissue necessary to reach the defect. Three pedicle advancement flaps were used to close the defect. The first 2 flaps were created by incising the right and left palatine and buccal mucosae. First, an incision was made
where the canine tooth had been on the right and just caudal to the canine tooth on the left. Second, incisions were made rostral to where the molars had been. Third, incisions were made along the right and left margins of the defect. The incisions were extended into the buccal mucosa and the gingival and buccal mucosae were undermined to create the flaps. A 3rd advancement flap was created caudal to the defect, as previously described. Since there was inadequate tissue to do a two-layer closure without creating excessive tension, an artificial layer was created by using a piece of polypropylene mesh (Monofilament Polypropylene Mesh; Bard, Tempe, Arizona, USA) fitted under the defect. The mesh was sutured to the rostral palatine mucoperiosteum and glued (Vetbond Tissue Adhesive; 3M, St. Paul, Minnesota, USA) to the remaining palatine bone in order to provide a base to support the flaps. The flaps were then advanced and closure was performed, as previously described. The closure appeared tension-free. Cefazolin was administered, 22 mg/kg BW, IV, q2h during surgery.
After surgery, the cat had some breathing difficulties due to bleeding in the nasal passages and was monitored in the intensive care unit overnight. Butorphanol (Torbugesic; Wyeth, Saint Laurent, Quebec), 0.3 mg/kg BW, IV, q4–6h for 36h, was administered. Postoperative management included IV fluids (6% Dextran 75; Abbott Laboratories), for 2 d; ampicillin (Ampicillin Sodium for injection; Novopharm, Toronto, Ontario), 60 mg, via E-tube for 11 d; and meloxicam, 0.1 mg/kg BW, SC, q24h for 6d.
The cat was fed a diet specially formulated to increase caloric intake for speedy recovery (Clinicare Feline Liquid Diet, Abbott Laboratories), 40 mL, via E-tube, q6h, followed by warm water (5 mL), instead of the previously utilized diet. This diet was chosen on the basis of its concentrated energy content and appropriate consistency for administration via a feeding tube. The cat was fed 160 kcal/d following the 2nd surgery. This was equivalent to approximately 1.1 times the BER.
Immediately after surgery, the graft appeared intact and pink. Two days following surgery, the cat ate dry cat food ravenously. The following morning, there was some slight dehiscence on the rostral right flap, but most of the graft appeared viable and to be healing nicely. By day 4, the edges of the rostral right flap were pale gray and 25% of the flap appeared nonviable along the incision. By day 5, all incisions had dehisced and the defect was quite large, although the mesh remained in place, effectively separating the nasal and oral cavities and limiting food passage to the nose. Tube feeding was discontinued at this time and the cat was placed on the diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition), ad libitum. The E-tube was removed 9 d after surgery. Again, inadequate blood supply was the suspected cause of the graft failure, although trauma to the site from eating dry cat food likely played a role.
The cat remains in hospital. Her appetite continues to be excellent and weight steady. She is still 5% to 10% underweight. Discussion of a 3rd surgery is underway.
Traumatic oronasal fistulas occur when trauma to the skull results in destruction of the palate separating the oral and nasal cavities. Many causes of traumatic palatal defects have been described, such as chronic infection from periodontal disease, bite wounds, blunt trauma, neoplasia, and electrocutihese defects can be repaired by using various flap and prosthetic implant tecgical correction is directed to restoring normal eating and drinking ability through functional separation of the oral and nasal cavities. Due to the rich blood supply and adequate strong, elastic donor tissue in the oral cavity, large defects can be
rostral third of the tongue was grossly scarred and tapered to a point.
When offered food, the cat had a strong interest in eating but difficulty in prehending and ingesting food. Cleft palate was diagnosed, and due to the nature of the defect and the tongue and jaw involvement, the inciting cause was thought to be electrocution, likely the result of biting an electrical cord. Surgical treatments were discussed with the owner. Due to the size of the defect, lack of local tissues for reconstruction, unknown blood supply to the associated tissues, and lack of bony support for surgical flaps, a guarded prognosis was given.
Results from preanesthetic blood studies were unremarkable and skull radiographs revealed a shortened right ramus of the mandible, but no obvious fractures or explanations for the malocclusion. The cat was found to be negative for Feline leukemia virus and Feline immunodeficiency virus. The cat was blood-typed, in the event that blood transfusions would be needed, and found to be type AB.
Before surgery, the cat was fasted for 12 h and then pre-medicated, IM, with acepromazine (Ace Atravet; Wyeth-Ayerst, Guelph, Ontario), 0.1 mg/kg bodyweight (BW), and hydromorphone (Hydromorphone HP-10; Sabex, Quebec City, Quebec), 0.1 mg/kg BW. Thirty minutes later, a catheter was placed and anesthesia was induced with ketamine (Vetalar Ketamine Hydrochloride for INJ; Bioniche Animal Health Canada, Belleville, Ontario), 5 mg/kg BW, and valium (Diazepam Injection USP; Sabex), 0.5 mg/kg, IV. The cat was intubated and maintained on isoflurane (IsoFlor; Abbott Laboratories, Saint Laurent, Quebec) with 100% oxygen. The cat was positioned in dorsal recumbency and gauze was placed around the endotracheal tube to block fluid entering the oropharynx and airways. Three mucosal pedicle flaps were used for closure of the fistula. The 1st flap was created by incising the gingival mucosa caudal to the right canine tooth and rostral to the 2nd premolar. These incisions were extended laterally to the mucocutaneous lip margin. A 3rd incision was made along the right border of the defect and the gingival mucosa was undermined to complete the flap. A 2nd flap was created from the left side of the hard palate by twice incising the full length of the hard palate and making a 3rd incision at the rostral end of the flap. When the first 2 flaps were advanced, there was still a small hole remaining at the caudal border of the defect. A 3rd flap was created caudal to the defect to cover the remaining hole. Closure was performed in 1 layer, using 6-0 suture (PDS II Suture; Ethicon, Somerville, New Jersey, USA) in a simple, interrupted fashion at all incisional margins. During surgery, the oral mucosa was noted to be very thin and the blood supply suboptimal. The tongue was then detached from the oral mucosa and its margins debrided to improve function. Intraoperatively, the cat was administered cefazolin (Cefazolin Sodium for INJ; Novopharm, Toronto, Ontario), 22 mg/kg BW, IV, q2h.
After the repairs, an esophagostomy tube (E-tube) was placed nsure optimal nutrition and to diminish trauma to the flaps associated with eating. The position of the tube was verified radiographically. Hydromorphone, 0.05 mg/kg BW, dexamethasone (Dexamethosone 5; Vetoquinol Canada, Lavaltrie, Quebec), 0.1 mg/kg BW, and acepromazine, 0.3 mg/kg BW, were given, IV, postoperatively, and a 25-μg fentanyl patch (Duragesic; Janssen-Ortho, Markham, Ontario) was placed on the right lateral thigh. Postoperative management included lactated Ringer’s solution (Ringer Lactate INJ; Abbott Laboratories) with 20 mEqKCl (Potassium Chloride for INJ; Abbott Laboratories), IV, at 12 mL/h; amoxicillin/potassium clavunate (Clavamox liquid suspension; Pfizer, Kirkland, Quebec), 14 mg/kg BW, by E-tube for 7 d; and
meloxicam (Metacam; Boehringer Ingelheim, Burlington, Ontario), 0.2 mg/kg BW, SC, followed by 0.1 mg/kg BW, SC, q24h for 6 d.
Since the cat was underweight before the surgery, adequate postoperative nutrition was important. The cat was fed a weight management diet (Eukanuba Maximum Calorie [EMC]; Iams, Dayton, Ohio, USA), 40 mL, by E-tube, q6h, followed by warm water (20 mL). This diet was chosen for its concentrated energy content and its appropriate consistency for administration via an E-tube. The feeding dosage was determined according to the manufacturer’s instructions for a 4–8 kg cat and the maximum amount within this range was fed. This was equivalent to 336 kcal/d, or 2.2 times the basal energy requirement (BER). The BER was calculated by multiplying the cat’s weight to the power 0.75, byhe BER was found to be 150 kcal/d. Animals suffering severe burns or trauma can be fed as much as twice the BER per day to account for the additional energy required by the body during healingn the basis of this information, the cat was overfed by approximately 13% daily.
On the day after surgery, the cat was mildly dehydrated and drooling profusely. Dehydration was confirmed by an elevated refractometer reading for total solids (80 g/L; reference range, 51 to 72 g/L). Fluids were increased to twice the maintenance requirement for 2 d, until the hydration status had improved. Two days after surgery, the cat was quiet, but affectionate, and had gained 0.18 kg, so it now weighed 2.94 kg. On the 3rd day after surgery, the cat was bright and alert, but necrosis of 25% of the left lateral flap was detected. The other flaps appeared to be healthy. By day 5, the necrotic tissue had sloughed and the incisions had dehisced completely. The defect resembled the original size. Deficiency of blood supply to the left lateral flap was speculated as the reason for the graft failure.
Following the graft failure, the cat was placed on half a can of a diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition, Topeka, Kansas, USA), q8h. This diet was chosen for its concentrated energy content and high palatability. In addition, its soft texture made it easy to prehend and unlikely to cause damage to the graft. The dose was equivalent to 270 kcal/d or 1.8 times the BER. This was within the manufacturer’s recommended dose for a cat of this size and condition. The E-tube was maintained for future use. In addition, the lower parts of the mouth were rinsed with 0.05% chlorhexidine (Novaldent; Ayerst, Fort Dodge, Iowa, USA) and saline solution, q8h, to help to prevent bacterial contamination in the healing area. By 6 d after surgery, the cat’s appetite was decreased and she had lost 0.14 kg and now weighed 2.80 kg. Part of the weight loss was attributed to fluid loss, but part was attributed to decreased food intake. A weight management diet (EMC), 40 mL, q6h, was added to the feeding regimen, via the E-tube, until the cat’s appetite returned to normal. After 2 d supplementation, the cat’s appetite was good and weight remained steady around 2.77 kg, so tube feeding was discontinued.
Surgery was repeated approximately 3 wk after the initial graft breakdown. Results from the preanesthetic blood studies were again unremarkable. The cat was medicated and prepared for surgery, as previously described. For the 2nd surgery, all of the teeth remaining in the upper arcade (incisors, premolars, molars, and right canine) were extracted, in order to increase the size of buccal flaps, after blocking the infraorbital nerves bilaterally with bupivicaine (Marcaine; Abbott Laboratories), 2 mg/kg BW. The associated palatine bone was removed with a high speed burr in order to smooth the edges and thereby decrease the amount of tissue necessary to reach the defect. Three pedicle advancement flaps were used to close the defect. The first 2 flaps were created by incising the right and left palatine and buccal mucosae. First, an incision was made
where the canine tooth had been on the right and just caudal to the canine tooth on the left. Second, incisions were made rostral to where the molars had been. Third, incisions were made along the right and left margins of the defect. The incisions were extended into the buccal mucosa and the gingival and buccal mucosae were undermined to create the flaps. A 3rd advancement flap was created caudal to the defect, as previously described. Since there was inadequate tissue to do a two-layer closure without creating excessive tension, an artificial layer was created by using a piece of polypropylene mesh (Monofilament Polypropylene Mesh; Bard, Tempe, Arizona, USA) fitted under the defect. The mesh was sutured to the rostral palatine mucoperiosteum and glued (Vetbond Tissue Adhesive; 3M, St. Paul, Minnesota, USA) to the remaining palatine bone in order to provide a base to support the flaps. The flaps were then advanced and closure was performed, as previously described. The closure appeared tension-free. Cefazolin was administered, 22 mg/kg BW, IV, q2h during surgery.
After surgery, the cat had some breathing difficulties due to bleeding in the nasal passages and was monitored in the intensive care unit overnight. Butorphanol (Torbugesic; Wyeth, Saint Laurent, Quebec), 0.3 mg/kg BW, IV, q4–6h for 36h, was administered. Postoperative management included IV fluids (6% Dextran 75; Abbott Laboratories), for 2 d; ampicillin (Ampicillin Sodium for injection; Novopharm, Toronto, Ontario), 60 mg, via E-tube for 11 d; and meloxicam, 0.1 mg/kg BW, SC, q24h for 6d.
The cat was fed a diet specially formulated to increase caloric intake for speedy recovery (Clinicare Feline Liquid Diet, Abbott Laboratories), 40 mL, via E-tube, q6h, followed by warm water (5 mL), instead of the previously utilized diet. This diet was chosen on the basis of its concentrated energy content and appropriate consistency for administration via a feeding tube. The cat was fed 160 kcal/d following the 2nd surgery. This was equivalent to approximately 1.1 times the BER.
Immediately after surgery, the graft appeared intact and pink. Two days following surgery, the cat ate dry cat food ravenously. The following morning, there was some slight dehiscence on the rostral right flap, but most of the graft appeared viable and to be healing nicely. By day 4, the edges of the rostral right flap were pale gray and 25% of the flap appeared nonviable along the incision. By day 5, all incisions had dehisced and the defect was quite large, although the mesh remained in place, effectively separating the nasal and oral cavities and limiting food passage to the nose. Tube feeding was discontinued at this time and the cat was placed on the diet formulated for animals recovering from serious illness or injury (Hills A/D; Hills Pet Nutrition), ad libitum. The E-tube was removed 9 d after surgery. Again, inadequate blood supply was the suspected cause of the graft failure, although trauma to the site from eating dry cat food likely played a role.
The cat remains in hospital. Her appetite continues to be excellent and weight steady. She is still 5% to 10% underweight. Discussion of a 3rd surgery is underway.
Traumatic oronasal fistulas occur when trauma to the skull results in destruction of the palate separating the oral and nasal cavities. Many causes of traumatic palatal defects have been described, such as chronic infection from periodontal disease, bite wounds, blunt trauma, neoplasia, and electrocutihese defects can be repaired by using various flap and prosthetic implant tecgical correction is directed to restoring normal eating and drinking ability through functional separation of the oral and nasal cavities. Due to the rich blood supply and adequate strong, elastic donor tissue in the oral cavity, large defects can be
 closed successfully by using gingival mucosal flapouble-layer closures are preferred when there is adequate tissue to provide tensionless appositle-layer flap technique has also been succeIn the case of this cat, tissue was inadequate to accommodate a double-layer closure without extracting teeth, so initially a single-layer closure was attempted. The thin oral mucosa, combined with surgical trauma, likely resulted in destruction of the blood supply to the mucosal flaps and subsequent graft failure. It is also possible that a tensionless apposition was not achieved or that physical trauma to the graft contributed to failure.
Several clinicians worked on this case, resulting in disparity in feeding regimens. Ideally, the cat would have been fed 1.25 to 2 times the BER daily. This would have met the basal metabolic needs of the cat and compensated for the additional energy required to heal from the trauma of surgeryood and water would have been administered via an esophagostomy tube, with nothing being given by mouth for approximately 2 wk. This would have minimized trauma to the graft from food particles and excess tongue movement, and maintained maximal cleanliness in the oral cavity, effectively reducing the chance of infection. Energy dense, highly palatable diets with an appropriate consistency (Eukanuba Maximum Calorie and Clinicare Feline Liquid Diet) were appropriate for this purpose. Trauma associated with the oral feeding of liquids postoperatively has been implicated in graft dehiscence in the region of the hard palate is possible that the ingestion of dry cat food 2 d following the 2nd surgery contributed significantly to the failure in this case. For the 3rd surgical repair, all attempts will be made to perform a proper 2-layer closure, paying close attention to maintaining the blood supply, eliminating tension, and minimizing trauma to the incision. It may be necessary to attempt more complicated reconstruction that uses microvascular techniques in order to bring in more tissue and ensure an adequate blood supply.
The author thanks Drs. Mitch Gillick, Kathleen Linn, and Lori MacDougall for their guidance with the case, and Dr. Cindy Shmon for her advice with the manuscript. CVJ
Winner of the CVMA Pet Food Certification Nutrition Award
Nicola Wilson’s current address is Oklahoma State University, College of Veterinary Medicine, Veterinary Clinical Sciences, 1 Boren Veterinary Medical Teaching Hospital, Stillwater, Oklahoma 74078, USA.
Dr. Wilson will receive 50 free reprints of her article, courtesy of The Canadian Veterinary Journal.
References 1. Coles BH, Underwood LC. Repair of the traumatic oronasal fistula in the cat with a prosthetic acrylic implant. Vet Rec. 1988;122:359–
2. Seim HB, Willard MD. Postoperative care of the surgical patient. In: Fossum TW, ed. Small Animal Surgery. 2nd ed. St. Louis, Missouri: Mosby, 2002:71–72. 3. Griffiths LG, Sullivan M. Bilateral overlapping mucousal single-pedicle flaps for correction of soft palate defects. J Am Anim Hosp Assoc. 2001;37:183– 4. Howard DR, Davis DG, Merkley DF, Krahwinkel DJ, Schirmer RG, Brinker WO. Mucoperiosteal flap technique for cleft palate repair in dogs. J Am Vet Soc. 1974;156:352–354. 5. Luskin IR. Reconstruction of oral defects using mucogingival pedicle flaps. Clin Tech Small Anim Pract. 2000;15:251– 6. Mathews KA. Veterinary Emergency and Critical Care Manual. Guelph: Lifelearn, 1997:19–18. 7. Rickards DA. Disjunction of the upper and jaw and traumatic cleft palate. Feline Pract. 1975;2:51–52. 8. Robertson JR, Dean PW. Repair of a traumatically induced oronasal fistula in a cat with a rostral tongue flap. Vet Surg. 1987;16:164–
closed successfully by using gingival mucosal flapouble-layer closures are preferred when there is adequate tissue to provide tensionless appositle-layer flap technique has also been succeIn the case of this cat, tissue was inadequate to accommodate a double-layer closure without extracting teeth, so initially a single-layer closure was attempted. The thin oral mucosa, combined with surgical trauma, likely resulted in destruction of the blood supply to the mucosal flaps and subsequent graft failure. It is also possible that a tensionless apposition was not achieved or that physical trauma to the graft contributed to failure.
Several clinicians worked on this case, resulting in disparity in feeding regimens. Ideally, the cat would have been fed 1.25 to 2 times the BER daily. This would have met the basal metabolic needs of the cat and compensated for the additional energy required to heal from the trauma of surgeryood and water would have been administered via an esophagostomy tube, with nothing being given by mouth for approximately 2 wk. This would have minimized trauma to the graft from food particles and excess tongue movement, and maintained maximal cleanliness in the oral cavity, effectively reducing the chance of infection. Energy dense, highly palatable diets with an appropriate consistency (Eukanuba Maximum Calorie and Clinicare Feline Liquid Diet) were appropriate for this purpose. Trauma associated with the oral feeding of liquids postoperatively has been implicated in graft dehiscence in the region of the hard palate is possible that the ingestion of dry cat food 2 d following the 2nd surgery contributed significantly to the failure in this case. For the 3rd surgical repair, all attempts will be made to perform a proper 2-layer closure, paying close attention to maintaining the blood supply, eliminating tension, and minimizing trauma to the incision. It may be necessary to attempt more complicated reconstruction that uses microvascular techniques in order to bring in more tissue and ensure an adequate blood supply.
The author thanks Drs. Mitch Gillick, Kathleen Linn, and Lori MacDougall for their guidance with the case, and Dr. Cindy Shmon for her advice with the manuscript. CVJ
Winner of the CVMA Pet Food Certification Nutrition Award
Nicola Wilson’s current address is Oklahoma State University, College of Veterinary Medicine, Veterinary Clinical Sciences, 1 Boren Veterinary Medical Teaching Hospital, Stillwater, Oklahoma 74078, USA.
Dr. Wilson will receive 50 free reprints of her article, courtesy of The Canadian Veterinary Journal.
References 1. Coles BH, Underwood LC. Repair of the traumatic oronasal fistula in the cat with a prosthetic acrylic implant. Vet Rec. 1988;122:359–
2. Seim HB, Willard MD. Postoperative care of the surgical patient. In: Fossum TW, ed. Small Animal Surgery. 2nd ed. St. Louis, Missouri: Mosby, 2002:71–72. 3. Griffiths LG, Sullivan M. Bilateral overlapping mucousal single-pedicle flaps for correction of soft palate defects. J Am Anim Hosp Assoc. 2001;37:183– 4. Howard DR, Davis DG, Merkley DF, Krahwinkel DJ, Schirmer RG, Brinker WO. Mucoperiosteal flap technique for cleft palate repair in dogs. J Am Vet Soc. 1974;156:352–354. 5. Luskin IR. Reconstruction of oral defects using mucogingival pedicle flaps. Clin Tech Small Anim Pract. 2000;15:251– 6. Mathews KA. Veterinary Emergency and Critical Care Manual. Guelph: Lifelearn, 1997:19–18. 7. Rickards DA. Disjunction of the upper and jaw and traumatic cleft palate. Feline Pract. 1975;2:51–52. 8. Robertson JR, Dean PW. Repair of a traumatically induced oronasal fistula in a cat with a rostral tongue flap. Vet Surg. 1987;16:164–