Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Pii: s0006-3223(99)00059-
The pharmacologic treatment of schizophrenia remains a
for a dopamine hypothesis of antipsychotic drug activity
critical component in the short- and long-term manage-
and, in turn, a dopamine hypothesis of schizophrenia. ment of this disease. Considerable progress has been
At the same time, further developments in establishing
made in delineating different domains of this illness,
the validity and reliability of psychiatric diagnosis resulted
ranging from positive and negative symptoms to cognitive
in a narrowing of the diagnosis of schizophrenia and to
dysfunction and psychosocial vulnerabilities. Increas-
some extent a reevaluation of drug efficacy in more
ingly, treatments are being studied in relation to a variety
selectively defined patient populations. of different outcome measures with functional ability andquality of life achieving appropriate emphasis.
It took many years after the introduction of antipsychot-
The introduction of a new generation of antipsychotic
ics to begin to establish the role of these medications in
drugs has helped to raise optimism and expectations.
long-term treatment, with the intention initially of reduc-
Overall, second-generation drugs do provide clear advan-
ing rates of relapse and rehospitalization. Even after
tages in terms of reducing adverse effects (particularly
relevant studies began to be conducted, very few lasted
drug-induced Parkinsonism, akathesia, and, hopefully,
more than 1 year, and they tended to involve multi-episode
tardive dyskinesia). Advantages in alleviating refractory
or chronically ill patients. At the same time that more and
symptoms, negative symptoms, depression, and suicidal
more data emerged supporting the value of maintenance
behavior are found in some reports; however, much
treatment (Davis 1975), increasing knowledge and con-
remains to be done methodologically in establishing the
cern was developing regarding the long-term risks associ-
relative merits of specific drugs in the multiple domains of
ated with antipsychotic drug treatment (Kane and Smith
Biol Psychiatry 1999;46:1396 –1408 1999
Not surprisingly, outcome measures in clinical trials of
Key Words: Schizophrenia, treatment, psychopharmacol-
antipsychotic drugs initially tended to focus more on
positive symptoms than negative symptoms. Positivesymptoms were more likely to be associated with disrup-tive or troublesome behavior, more likely to result in
Introduction
hospitalization (the focus for most initial clinical trials ofdrug efficacy), and to some extent were felt to be easier to
The modern-age of pharmacologic treatment of schizo- measure.
phrenia began in the mid-1950s with the development
With this background, for the first two decades of
of chlorpromazine. Subsequent to that development, a
widespread clinical use of antipsychotic medication, it was
number of different chemical classes of antipsychotic
generally accepted that among available agents there were
drugs were introduced into clinical practice. Over the next
no significant differences in clinical efficacy. In 100
three decades, considerable progress was made in several
comparisons of different conventional antipsychotic drugs,
areas which influenced subsequent development and uti-
only one study reported a significant difference (Klein and
lization of antipsychotic drugs as well the over all care of
Davis 1969; Janicak et al 1993). This result did not
patients suffering from schizophrenia.
necessarily mean that an individual patient was equally
The observations that antipsychotic drugs were associ-
likely to respond to any drug, but rather in group compar-
ated with a variety of neurologic side effects, most
isons similar proportions of patients responded regardless
commonly drug-induced Parkinsonism, but also tardive
of which drug was involved. The notion that if a particular
dyskinesia and tardive dystonia, helped contribute support
patient did not respond to one drug, then he or she mightrespond to another was widely assumed, however, as wewill discuss below, rarely tested.
From the Department of Psychiatry, Hillside Hospital, Division of Long Island
The discovery that enormous variations in bioavailabil-
Jewish Medical Center, Glen Oaks, New York and Department of Psychiatryand Neuroscience, Albert Einstein College of Medicine, Bronx, New York.
ity and metabolism occurred with these drugs led to
Address reprint requests to John M. Kane, MD, Hillside Hospital, 75-59 263rd
renewed hope that outcome could be improved substan-
Received October 12, 1998; revised February 17, 1999; accepted March 5, 1999.
tially by measuring blood levels following the develop-
ment of steady state and adjusting them up or down
deficiency was a high incidence of acute and chronic
accordingly (Kane et al 1976). Despite a fairly extensive
neurologic effects. Second was frequent poor or only
literature suggesting relationships between blood levels
partial response of both positive and negative symptoms
and clinical response, very few studies confirmed the
with considerable residual disability (psychosocial and
value of these measures by subsequently manipulating
vocational). The third deficiency was high rates of non-
blood levels into a putative therapeutic range, under
compliance, which were felt to be at least partially due to
controlled conditions and demonstrating a clinically and
frequent adverse effects and subjective discomfort. Fourth
statistically significant effect (Volavka et al 1992). The
was the lingering uncertainty as to whether or not antipsy-
reality is that blood levels have not come to be used
chotic drugs were really affecting the long-term course of
routinely as a reliable and valued guide to clinical man-
schizophrenia or merely reducing the more florid mani-
agement. (Whether this is the consequence of lack of
knowledge transfer, impediments related to cost and fea-
It is sobering to note that attempts to assess historical
sibility, or an insufficiently compelling data base could be
trends in the outcome of schizophrenia over the long term
have not shown significant progress in the past several
Another important development in the pharmacologic
treatment of schizophrenia was the introduction of long-
In the 1980s, a number of factors helped to change the
acting injectable (depot) medications. Compliance in oral
scope of both clinical investigation and expectation. First,
medication-taking over long periods of time is an enor-
enhanced methodology was developed for assessing neg-
mous problem (Kane 1985). Initially, the mirror image and
ative symptoms (problems differentiating primary from
controlled trials with these medications led to considerable
secondary negative symptoms on a short-term basis re-
enthusiasm regarding their potential to improve long-term
main evident) and a renewed emphasis was placed on their
outcomes, by reducing rates of relapse and rehospitaliza-
importance. Second, advances in neuropsychology helped
tion. Interestingly, a number of trials comparing oral and
to generate an extensive and more refined data base on
depot medication were not successful in demonstrating as
various aspects of cognitive dysfunction in schizophrenia.
significant a reduction in rates of relapse as expected
These findings contributed to increased awareness of the
(Glazer and Kane 1992). We have argued elsewhere (Kane
relative independence of cognitive dysfunction from pos-
and Borenstein 1985) that, to some extent, this is likely a
itive psychotic symptoms (including the former preceding
result of the methodology employed in these trials. Spe-
the onset of the latter) and its important impact on
cifically, relatively compliant patients were selected given
functional outcome. Third, the renewed interest in and
the nature of the study design (double-blind oral and depot
ultimate marketing of clozapine reenergized the search for
drug, frequent assessments, need for consent, etc.) Perhaps
new drugs with different characteristics and challenged the
most importantly, almost all of these trials lasted only 1
field to look for differential effects of new generation
year. Given the time frame likely involved in becoming
noncompliant and the average lengthy delay between
Much remains to be done in establishing the relative
actually discontinuing medication and subsequent relapse
merits of new generation drugs. The one property that is
in stable or remitted patients (i.e., 3–7 months) a 1-year
clearly apparent in most studies is reduced propensity to
trial is unlikely to find a difference. The only controlled
produce neurologic adverse effects. Some researchers
comparison between oral and depot preparations that
have questioned the role of dosage of the comparative
lasted more than 1 year (Hogarty et al 1979) found a
drug (and the fact that it has usually been haloperidol) in
striking difference in the second year, which did not reach
this context. Interestingly, one study (involving sertindole)
statistical significance because of the small sample size.
(Zimbroff et al 1997) did use three different doses of
Unfortunately, depot drugs were initially administered
haloperidol in a fixed-dose design. The lowest dose (4 mg)
in higher than necessary doses (Glazer and Kane 1992)
was associated with significantly more extrapyramidal
and were presumed to cause more side effects when in
side effects (EPS) than placebo or any dose of sertindole,
reality there is no evidence that this is the case. In addition,
supporting the assumption that the superiority of the
depot drugs have not been widely used in the United States
second-generation drugs regarding EPS is not solely due
for a variety of nonscientific reasons, despite their poten-
tial value in an illness with very high rates of noncompli-
As suggested previously, there are a number of critical
ance. (The role of new generation drugs in potentially
areas in which the new drugs need to be evaluated,
reducing rates of non compliance will be discussed be-
particularly against each other, but in some cases against
conventional drugs as well. Clearly, the management of
The first three decades of widespread antipsychotic use
refractory or poorly responsive patients is a high priority,
highlighted a number of major deficiencies. The first
but so are the domains of negative symptoms, cognitive
dysfunction, compliance, and relapse prevention. Data are
will focus largely on populations of treatment-refractory
beginning to emerge on some of these issues, but defini-
tive conclusions in a number of areas are as yet difficult to
Kane et al (1988) reported on 267 schizophrenia pa-
make. In addition, the question as to whether or not these
tients who met strict criteria for treatment resistance.
drugs can have more of an impact on various domains of
Patients had to fail to respond to adequate trials of at least
outcome if they are introduced earlier in treatment is
three antipsychotic drugs and a prospective, single-blind
beginning to receive appropriate attention. Another oppor-
trial of haloperidol. Clozapine was associated with signif-
tunity given better adverse-effects profiles of new drugs
icantly greater improvement in both positive and negative
might be to attempt to prevent the emergence of psychotic
symptoms. Using a priori criteria for improvement, 30%
symptoms in patients who are exhibiting prodromal signs,
of clozapine-treated patients improved after 6 weeks in
or eventually in those individuals with highly specific risk
comparison with 4% of those receiving chlorpromazine.
factors even prior to becoming symptomatic.
Since that report, a number of controlled trials have
As we learn more about the complexity of this disease
confirmed clozapine’s superiority over conventional drugs
(or diseases), we should also remain open to the possibility
in improving positive symptoms (Pickar et al 1992; Breier
that a combination of different pharmacologic agents as
et al 1994). However, clozapine’s impact on primary
well as nonsomatic treatment could be necessary to pro-
negative symptoms or deficit state remains the subject of
duce optimum results. We seem, at times, to harbor what
ongoing debate (Carpenter et al 1995; Kane 1996a; Melt-
might be an unrealistic expectation that a single agent will
zer 1995). For example, in a 6-month, double-blind
influence some basic pathophysiologic factor that is pri-
comparison of clozapine and a modest dose of haloperidol
mary to all of the diverse manifestations of this illness,
(10 mg/day) conducted in poor or partially responsive
rather than recognizing the more likely possibility that
outpatients, we found clozapine to be superior in positive
palliative treatments are necessary in diverse areas of brain
symptoms, but not on negative symptoms.
function, while we await a deeper understanding of etiol-
Two relatively long-term controlled trials have now
been reported with clozapine. Essock et al (1996a) carriedout an effectiveness trial of clozapine in which 227treatment-refractory, state hospital inpatients were ran-
Clozapine
domly assigned to nonblind, continued “usual care” ortreatment with clozapine. There was no significant differ-
The introduction of clozapine into clinical practice helped
ence between clozapine and the usual care condition in the
to set the stage for a variety of new perspectives on
rate of discharge over the 24-month follow-up period, nor
antipsychotic drug treatment, drug development and out-
were there any significant differences on measures of
come assessment. Clozapine was the first drug to demon-
psychopathology. However, clozapine subjects who were
strate a qualitative difference in propensity to produce
discharged were significantly less likely to be rehospital-
neurologic side effects (Casey 1989) and the first drug to
ized than those in the comparison group.
show clear superiority over other drugs in the treatment of
Rosenheck et al (1997) conducted a randomized, 1-year,
refractory patients (Kane et al 1988).
double-blind, comparative trial of clozapine and haloper-
As a result, an enormous amount of research has been
idol in 423 patients at 15 Veterans Affairs Medical
conducted to determine what neuropharmacologic charac-
Centers. Significantly, more (57%) clozapine-treated pa-
teristics of clozapine are responsible for these novel
tients continued on the assigned treatment for the whole
effects. At present, there are an extraordinary array of
year in comparison with only 28% in the haloperidol
findings showing differences between clozapine and con-
group. Also, significantly more haloperidol patients dis-
ventional drugs on neuroimaging, and neurophysiologic
continued drug treatment due to worsening of symptoms
and neurochemical measures. However, at present it is
or lack of efficacy (51%) in comparison with clozapine
difficult to make definitive statements as to what charac-
patients (15%). Among subjects taking clozapine, a 20%
teristic(s) account for clozapine’s clinical profile.
reduction in the total score on the Positive and Negative
As a result of clozapine’s adverse effect profile, specif-
Syndrome Scale was seen in 24% of subjects after 6 weeks
ically, what initially appeared to be a 1–2% risk of
and 37% after 1 year. However, this difference was not
potentially fatal agranulocytosis (incidence estimates have
significant from the 13% and 32%, respectively, who
been revised downward and now are below 0.4% in the
showed the same level of improvement on haloperidol.
first year of treatment [Novartis, unpublished data]), the
The data regarding relapse are intriguing. In general, we
use of this drug has generally been confined to treatment-
do not think of those patients who relapse despite contin-
refractory, or in some cases, treatment-intolerant patients.
ued maintenance medications as “refractory,” but clearly
Therefore, any discussion of clozapine’s clinical effects
this subgroup is not responding optimally. Even with
guaranteed medication delivery (i.e., depot drugs), approx-
slightly less than 10% considered unchanged or worse). In
imately 15–20% of patients will experience a relapse over
more recent trials, the proportion of patients considered to
a 1-year period (Kane 1996b). There are hardly any data to
have an inadequate response appears to be somewhat
inform clinical strategies for managing such patients. We
higher. Representative trials that attempted to exclude
(Pollack et al 1998) also have observed in a mirror image
refractory patients published in the 1990s reported an
analysis of hospitalization before and after clozapine in 81
average good response rate of 50% (Levinson et al 1990;
patients that the rate on clozapine was significantly re-
Van Putten et al 1990; Rifkin et al 1991; Volavka et al
duced. Clearly, given the mirror image design there are
other factors that may have contributed to this difference.
This response rate raises the question as to whether or
With clozapine’s evidence of novel properties, a con-
not response to medication has declined over the past three
trolled trial focusing on relapse prevention in patients who
decades. There certainly are a number of factors that could
have “broken through” other drugs would be of consider-
have contributed to the appearance of such a decline. First,
the nosology has changed considerably during that inter-
There have been a series of reports suggesting superiority
val, with the definition of schizophrenia becoming nar-
for clozapine in a number of areas such as hostility and
rower and that of affective illness becoming broader (at
violence (Mallya et al 1992), substance abuse (Albanese et al
least in the United States). Therefore, it is possible that
1994; Buckley et al 1994), and suicidal behavior (Meltzer
more modern-day trials include a relatively more homog-
and Okayli 1995). These observations have been derived
enous population of patients with schizophrenia. Second,
mainly from uncontrolled observations of primarily chronic
the prevalence of substance abuse among patients with
refractory or partially drug-responsive patients.
schizophrenia has increased enormously over the past 20
It is important now, given the availability of alternative
years. Some studies (Regier et al 1990; Shaner et al 1993)
second-generation drugs, to examine these effects in
find a 50% lifetime prevalence of substance abuse among
controlled trials. Despite the proven advantages of cloza-
patients with schizophrenia. Although it is clear that drugs
pine, this drug has been largely underused in clinical
of abuse can exacerbate symptoms of psychosis, the extent
practice. This was the case even before the introduction of
to which chronic drug abuse alters the potential respon-
other second-generation, or putative “atypical” com-
siveness of the underlying condition to antipsychotic
medication has not been determined adequately. Because,however, some of the same receptors are involved in theseeffects, there is reason for concern. Treatment Refractoriness: General Issues
A third possible factor is the trend in recent years to
The success of clozapine in refractory patients led to
limit hospitalization whenever possible. This trend could
renewed interest in and hope for developing better treat-
have resulted in a change in the population of patients
ment strategies for such patients. The first consideration in
available for clinical trials. In addition, there may be an
this context is the definition or criteria by which patients
inherent bias in the way patients are selected for clinical
are identified. In the original multicenter clozapine trial
trials. Especially when placebo controls are utilized, pa-
(Kane et al 1988), a very stringent definition was used;
tients who have responded well to medication might be
however, it is clear that many other patients (who would
reluctant to risk placebo exposure or exposure to an
not necessarily meet those criteria) derive only partial
experimental drug. In contrast, those patients who have
benefit from conventional drugs. As a rule, definitions of
had only poor or partial response and/or those who have
treatment resistance have relied more heavily on positive
had significant adverse effects from earlier treatment
symptom assessment, yet it is clear that many patients
might be more likely to participate in such trials unless
suffer from persistent negative symptoms such as apathy,
explicit efforts are made to exclude them.
anhedonia, or affective impairment. In addition, many
Recently, we (Kane and Borenstein unpublished data)
patients suffer in the so-called third factor domain of
reviewed response rates in more than 700 haloperidol-
disorganization and cognitive dysfunction. (We have al-
treated patients participating in placebo-controlled, new
luded previously to the problem of those patients who
drug development trials and found that the proportion of
“break through” adequate maintenance or prophylactic
patients improving 30% or more on the Brief Psychiatric
treatment as another subgroup who might be considered
Rating Scale (BPRS) total score ranged from 12% to 45%.
Overall, the demographic and treatment history character-
By far the largest category of patients appears to be poor
istics of patients participating in these trials reveals that
or partial responders. In those trials conducted in the 1960s
most are male, have an average age in the mid-to-late 30s,
(Klein and Davis 1969), approximately 38% of patients
have had six or more prior hospitalizations, and have been
derived little if any benefit from medication (including the
These demographics underscore the fact that patients
for a study such as our original clozapine study; however,
participating in these trials represent a particular subgroup
given increasing pressure on length of stay clinicians are
at a chronic phase of illness. It is likely that this population
frequently inclined to try alternatives even within a rela-
may have limitations or differences in terms of delineating
tively brief time frame if patients are not improving. A
the potential impact of novel pharmacologic agents on the
sample of 156 acutely ill patients were enrolled initially.
course of schizophrenia in comparison with patients who
At the end of 4 weeks of fluphenazine, 115 subjects had
completed this portion of the trial and 68% of those stillhad a score of moderate or more on at least one psychoticitem. Fifty-eight patients entered a second 4-week phase in
Alternative Treatment Strategies
which they were randomly assigned double-blind to con-
When patients do not respond adequately, clinicians face a
tinue on fluphenazine 20 mg/day; have the dose increased
challenge as to when and if to abandon the current
to 80 mg/day; or be switched to haloperidol 20 mg/day.
treatment, to increase the dose, to add adjunctive medica-
Only 9% of subjects who completed this phase achieved
tion, when to switch to another drug, and which drug to
the a priori response criteria and there were no significant
switch to. Despite the frequency of this situation, there are
differences between the three alternatives.
still inadequate data by which to inform clinical practice.
It is possible, however, that further improvement would
The dilemmas faced for years by clinicians with conven-
be observed with specific alternatives administered over a
tional drugs are now being repeated in many cases with the
longer period of time than 4 – 8 weeks. Shalev et al (1993)
evaluated the proportion of acutely exacerbated schizo-
It is sobering to look at the literature with conventional
phrenic patients who remained unimproved after consec-
drugs to suggest what lessons might be learned for current
utive administration of haloperidol, chlorpromazine, and
and future research with newer medications. When drugs
perphenazine in randomly determined order. Two criteria
are developed initially, the pharmaceutical companies do
were used concurrently to define therapeutic success: a
not necessarily have an incentive for studying a broad
decrease of 30% in a modified version of the BPRS; and
range of doses or even establishing clearly what the
clinical improvement sufficient to permit discharge back
maximum tolerated dose will be. As a result, once a drug
to the community. Sixty patients completed the trial (58%
is marketed there is a natural tendency among clinicians to
were woman, the mean age was 33 years, and the number
try higher doses (assuming they are tolerated) in patients
of previous admissions averaged four). Each phase of the
who are not responding adequately. This practice became
study averaged 28 –33 days. Patients who did not improve
such a widespread tendency with the conventional drugs
during each 4-week period were switched to the next drug
that it was not at all uncommon to see many patients
according to their predetermined schedule; however, if
treated with extremely high doses of fluphenazine or
there was a “subthreshold” improvement, the drug was
haloperidol (or other mid-to-high potency drugs). Al-
continued another week before determining ultimate re-
though some studies suggested that high-dose or even
sponse to that phase. The average daily doses were 27–30
“megadose” treatment might be beneficial in a proportion
mg for haloperidol, 350 –380 mg for chlorpromazine, and
of refractory patients, well-designed studies (Prien and
Cole 1968; Quitkin et al 1975; Bjorndal et al 1980) found
The total improvement rate was 95%; only 3 of 60
little consistent advantage. Despite this lack of data, many
patients remained unimproved after the three phases of the
clinicians continue to use high doses, especially in patients
study. Of the patients entering each phase of the trial, 67%
who are exhibiting hostile or aggressive behavior (Rem-
improved after the first drug, 55% after the second, and
67% after the third. The differences in improvement rates
There are remarkably few studies assessing the value of
between the phases were not statistically significant, nor
switching from one antipsychotic drug to another, either
were differences found between men and women. The
with conventional drugs or with the new generation drugs.
differences in improvement rates between the three drugs
In addition, studies remain to be conducted of dosage
over the entire trial were not statistically significant.
escalation (or reduction) in poor or partially responsive
The disparity in results between these two trials might
patients with the new generation drugs.
be due at least in part to differences in the criteria for good
We (Kinon et al 1993) reported results from a study
response. Whereas the Kinon et al (1993) study required
designed to compare the relative efficacy of treatment
ratings of no more than “mild” on any psychotic item, the
alternatives using conventional drugs in patients who
Shalev et al (1993) study required a 30% improvement on
continued to exhibit clinically significant positive symp-
the total BPRS scale. In addition, the Shalev study used a
toms after a 4-week trial of fluphenazine (20 mg/day).
4-point version of the BPRS so the rating scale data cannot
These were by no means patients who would meet criteria
be compared easily. It is also not possible to determine
whether or not the improvement occurring in the second
mean dose 7.75 mg) or clozapine (n ϭ 57, mean dose 420
and third phases was in fact due to the change in drug or
mg/day) over an average of 12 weeks. Utilizing a response
the passage of additional time. In addressing this issue,
criterion of a 20% reduction in total Positive and Negative
Shalev et al (1993) rightly point out that it is difficult to
Syndrome Scale (PANSS) score, 44% of the clozapine-
maintain poor responders on the same drug for 12 weeks.
treated and 28% of the risperidone-treated patients re-
It is notable that none of the drugs appeared superior in
sponded. Bondolfi et al (1998) have reported on 86
this context, despite some differences in receptor binding
inpatients with treatment refractory schizophrenia as-
signed randomly to an 8-week double-blind trial of ris-
We have already discussed the role of clozapine in
peridone or clozapine. The mean daily dose for clozapine
treatment-refractory schizophrenia. In general, clozapine
was 291 mg and for risperidone 6.4 mg. The criterion for
has the most data supporting its efficacy in this population.
categorizing patients as improved was a 20% reduction in
A recent meta-analysis conducted by Wahlbeck (1998)
total PANSS score. At the end of the study, 67% of
involved a review of 2,560 randomized participants from
risperidone-treated patients and 65% of clozapine-treated
31 mainly short-term trials. Wahlbeck concluded that
patients met response criteria. This study has been criti-
clozapine was clearly more effective than conventional
cized on the grounds that the dose of clozapine was low by
antipsychotics in reducing symptoms of schizophrenia,
some standards and the response rate was higher than
both in treatment-resistant and nonresistant patients. How-
generally seen in 8-week trials of clozapine in refractory
ever, Wahlbeck found no convincing evidence that the
patients, suggesting this population may have been some-
superior clinical effect of clozapine results in improved
levels of functioning. It is not possible to determine to
Additional data will be necessary to clarify the relative
what extent this is a result of inadequate methodology or
value of risperidone in treatment-refractory patients and a
number of relevant trials are currently underway.
Other treatment strategies for refractory patients have
included adjunctive treatments such as lithium, benzodi-azapines, anticonvulsants ,and electroconvulsive therapy.
Though some patients may benefit from these strategies,
Olanzapine was marketed in the United States beginning
the proportion of such patients is low (Christison et al
in 1996. Several large-scale trials have been conducted
1991). We continue to struggle with the question of which
demonstrating olanzapine’s efficacy in the treatment of
alternatives should be pursued when the one or two most
schizophrenia. Most studies were controlled with placebo
likely to succeed do not. Clinicians must balance the
and/or haloperidol, but more recently studies are being
appropriateness of trying numerous unproven treatments
reported comparing olanzapine with risperidone or cloza-
or accepting the possibility that with our current state of
pine. As is the case with all new drugs, in the initial studies
knowledge we are not always successful.
conducted for drug regulatory purposes the patient demo-graphics were such that the efficacy results might have
Second-Generation Antipsychotics
underestimated the impact in younger patients, and/orpatients closer to the onset of the illness. In general, the
studies showed at least equivalent antipsychotic efficacy
Risperidone was marketed beginning in 1994 in the United
to haloperidol, with some evidence of superiority on
States and has been used widely since then. Risperidone’s
negative symptoms and depression (Beasley et al 1996;
efficacy was established in seven clinical studies of
Tollefson et al 1997b, 1998). Clear superiority was evident
acutely psychotic patients (Borison et al 1992; Claus et al
concerning neurologic side effects and several other ad-
1992; Muller-Spahn 1992; Ceskova and Svestka 1993;
Chouinard et al 1993; Heinrich et al 1994; Marder and
In addition, analysis of double-blind, continuation data
Meibach 1994). In the United States-Canadian multicenter
from patients receiving olanzapine or haloperidol revealed
trial, 6 or 16 mg of risperidone per day were superior to
a significantly lower incidence of treatment-emergent
haloperidol (20 mg/day) on reduction in total positive and
dyskinesia among olanzapine-treated patients (Tollefson
negative syndrome scale scores. At present, there is no
et al 1997a). The incidence observed with haloperidol was
evidence that doses higher than 6 mg/day offer any
similar to that observed in incidence studies involving
advantage and are associated with a higher incidence of
conventional antipsychotics (Kane 1995), a result that is
EPS. In initial trials (Marder and Meibach 1994), risperi-
helpful in supporting the validity of the findings.
done appeared to be helpful for some refractory patients.
In a more recent study (Tran et al 1997), olanzapine was
Flynn et al (1998) described a series of cases of refractory
compared with risperidone in 339 schizophreniform,
patients treated openly with either risperidone (n ϭ 29,
schizophrenia, and schizoaffective patients over a 28-week
treatment period. The mean dosage of olanzapine was 16.9
of double-blind trials (Arvanitis et al 1997; Peuskens and
mg/day and that of risperidone 7.3 mg/day. Side effects,
Link 1997). Superiority was demonstrated over placebo on
particularly extrapyramidal, were more common in the
measures of positive and negative symptoms. No signifi-
risperidone group at week 8 and week 28. The olanzapine
cant superiority in efficacy was demonstrated in compar-
treatment group showed significantly greater improvement
ison with conventional drugs, but quetiapine was shown to
on measures of negative symptoms, and a significantly
produce very low levels of EPS and to be generally well
lower rate of exacerbation during the 28-week trial. The
tolerated. To date, there are no published data available in
average dose of risperidone used in this study was some-
treatment-refractory patients for quetiapine. Concern
what greater than is generally recommended today for the
about possible ophthalmologic effects has led to recom-
treatment of psychosis and this difference might have
mendations of eye examinations at baseline and during
influenced the higher rate of adverse effects seen with
risperidone. However, half the patients on risperidone
In summary, as a class, the second-generation antipsy-
received dosages less than 6 mg/day.
chotics clearly have advantages over conventional drugs
Studies are beginning to be reported examining olanza-
particularly in the area of adverse effects (with the
pine’s potential for improving outcome in treatment-
exception of weight gain). Data with regard to positive and
refractory patients. In one open trial of olanzapine, 36% of
negative symptom superiority are still inconsistent and
patients achieved response criteria (Martin et al 1997) and
limited by methodologic considerations.
in another, 48% of treatment refractory patients were
When differences have been found between new com-
reported to have responded to olanzapine (Baldacchino et
pounds and standard agents (i.e., haloperidol), the effect
sizes have generally been small to medium. Schooler
Conley et al (1998) reported on an 8-week, double-blind
(1998) reviewed data on representative studies and found
comparison of olanzapine and chlorpromazine in 84 treat-
a mean effect size of .20 in comparison with haloperidol
ment-refractory subjects. No difference in efficacy was
on negative symptoms (with the highest being .53).
observed on measures of psychopathology. Seven percent
Clearly, diminution of parkinsonian side effects can
of the olanzapine-treated patients responded according to a
have important effects on appearance, subjective well-
priori criteria and no chlorpromazine-treated patients re-
being, and functioning, so these gains are considerable. In
sponded; however, this difference was nonsignificant. The
addition, reducing the need for the adjunctive antiparkin-
mean dosage of chlorpromazine was 1,173 mg/day. All
sonism medications has other potential benefits.
olanzapine-treated patients received 25 mg/day. Overall,
Other domains of outcome are now being explored as
neither drug group experienced substantial change in the
well. Increasing attention has been focused on cognitive
severity of psychosis from their baseline state.
function as an area of considerable impairment in schizo-
Breier and Hamilton (1999) reported on a subpopulation
phrenia. An estimated 75% of patients with schizophrenia
of patients meeting retrospectively applied criteria for
exhibit some neuropsychological dysfunction (Gold and
treatment-refractory schizophrenia, selected from a large
Harvey 1993). It has been shown that cognitive dysfunc-
prospective, double-blind, 6-week study of olanzapine and
tion can be an important determinant of poor social and
haloperidol (Tollefson et al 1997b). Olanzapine showed
vocational outcome and can play more of a role in these
superiority over haloperidol for those who completed the
domains than psychotic signs or symptoms (Green 1996).
study on most of the major measures of psychopathology.
It also appears that some type of cognitive dysfunction
This study was limited by the retrospective nature of the
precedes the overt onset of a schizophrenic illness (Erlen-
determination of nonresponse, which relied on failure to
respond to at least one 8-week trial of a neuroleptic during
The new generation antipsychotics appear to hold con-
the previous 2 years and presence of a specified level of
siderable promise in either improving or not worsening
severity at baseline when subjects were still being treated
specific aspects of cognitive functioning. So far, there
with a prior neuroleptic. These criteria are not as clear or
remain only a relatively small number of studies and very
selective as those used in Conley’s study.
few controlled trials focusing on the impact of second
Further research is necessary to clarify the role of
generation drugs on cognitive function.
olanzapine in treatment-refractory patients.
Reports on clozapine are mixed and somewhat contra-
dictory (Hagger et al 1993; Goldman et al 1996). Reportson risperidone are beginning to emerge (Green et al 1997)
as are data on olanzapine (Canadian Cognition and Out-
The most recently marketed antipsychotic in the United
come Study Group 1998), but it is too soon to draw firm
States is quetiapine. This compound was also compared
with placebo and conventional antipsychotics in a number
A critical area for assessing the ultimate impact of
Figure 1. Cumulative rates of relapse amongpatients with schizophrenia after 1 year of main-tenance therapy with various doses of antipsy-chotic drugs, in six studies. Most patients hadhad more than one prior psychotic episode. Fluphenazine decanoate was given biweekly,and haloperidol decanoate was given monthly. Doses of fluphenthixol decanoate, which wasused in some of the studies, are expressed interms of estimated equivalent doses of fluphen-azine decanoate. The number of patients in eachgroup in these studies ranged from 29 to 63.
intervention strategies involves measures of functioning.
effects in relatively short-term trials, there has been far
Here too, results from controlled trials (even with cloza-
less activity in the maintenance treatment arena. In addi-
pine) are not as clear-cut as one would like, but this will
tion, such trials are difficult to conduct, take long periods
become an increasingly important domain in comparing
of time, and can be very expensive. At the same time, if we
the impact of different treatment strategies.
really are interested in altering the course and improving
Overall, there are still too few direct comparisons of the
functional outcome of this disease, it is producing and
new drugs against each other. There are also no data
sustaining gains over the long-term that is critical.
providing predictors of response that might help clinicians
The importance of maintenance medication has been
to choose the ideal drug for a specific patient. There is
well established in numerous double-blind, placebo-con-
hope that pharmacogenomics may provide important guid-
trolled trials (Davis 1975; Kane and Lieberman 1987;
ance; however, we have not yet seen consistent results in
Gilbert et al 1995). Even if the focus is just on patients
this regard (Arranz et al 1995; Malhotra et al 1996).
who had been in remission for a year or more, availablestudies indicate that approximately 75% will relapsewithin 12–18 months after the discontinuation of antipsy-
Maintenance Treatment
chotic medication (Kissling 1991; Davis et al 1994). These
Given the nature of schizophrenia and its long-term
data are particularly important for clinicians to appreciate
course, the role of maintenance treatment is absolutely
because it is not uncommon for both patients and clini-
critical. Because drug development relies heavily on acute
cians to develop a false sense of security regarding
Figure 2. Rates of relapse among patientswith schizophrenia after 1 year of contin-uous or intermittent maintenance therapy,in five studies. Black bars represent con-tinuous treatment, and shaded bars inter-mittent treatment. Most patients had hadmore than one prior psychotic episode. The number of patients in each group inthese studies ranged from 27 to 121.
diminished need for medication when the patient has been
treatment is feasible, but that the risk of relapse during
in remission for a year or more. Current American
therapy is somewhat greater than if the maintenance dose
Psychiatric Association (APA) guidelines (Herz et al
is higher (Figure 1). Although lower doses were associated
1997) recommend that individuals recovering from their
with fewer adverse effects, in general, this relationship has
first episode of illness should probably be treated for 1–2
not been demonstrated clearly with respect to tardive
years; however, 75% of patients will have relapses after
therapy is discontinued. These guidelines should be re-
Intermittent treatment is a strategy intended to take
vised as fears of long-term drug toxicity decline. Patients
advantage of the observation that many individuals do not
who have had two or more episodes should receive
experience a relapse until several months after the discon-
maintenance treatment for at least 5 years (according to
tinuation of antipsychotic medication. This strategy in-
current APA guidelines) and many experts believe they
cludes the discontinuation of antipsychotic medication in
should be treated indefinitely (Davis et al 1994). We have
stable outpatients who are in remission and the reinstitu-
been hard pressed to identify subgroups of patients to
tion of medication if and when prodromal signs of relapse
whom these recommendations do not apply. It is also
occur. The hope of this “early intervention” is to prevent
clear, as previously discussed, that 15–20% of patients
a full-blown psychotic relapse. The overall goal is to
will relapse within a year despite guaranteed medication
reduce the cumulative exposure to antipsychotic drugs and
delivery (i.e., depot drugs). When rates of noncompliance
limit adverse effects. Five major studies have examined
are also taken into consideration, the frequency and
this strategy (Jolly et al 1989, 1990; Carpenter et al 1991;
consequences of relapse take on enormous public health
Herz et al 1991; Pietzcker et al 1993; Schooler et al 1997).
proportions (Weiden and Olfson 1995).
All of the patients in these trials were treated for 2– 6
An important focus of recent research with conventional
months before therapy was discontinued in those individ-
antipsychotic drugs has been to improve the overall
uals who were assigned to the intermittent treatment
benefit-to-risk ratio of long-term antipsychotic drug treat-
groups. The cumulative rates of relapse after 1 year in the
ment by establishing optimal strategies. Studies comparing
groups that received continuous treatment were similar to
different fixed doses and comparing continuous with
those reported for the conventional doses of antipsychotic
intermittent therapy have been conducted. Six studies
drugs in the trials involving low-dose therapy. The results
involving different doses given for at least 1 year have
with intermittent treatment, however, were in general
been reported (Kane et al 1983, 1986, 1993a; Marder et al
discouraging (Figure 2). The rates of relapse during the
1984, 1987; Johnson et al 1987; Hogarty et al 1988;
1-year study follow-up interval were high and in addition
Schooler et al 1997). All involved long-acting, injectible
there was little benefit in terms of psychosocial adjust-
medication given at intervals of 2– 4 weeks. The results
ment, enhanced subjective well-being, or diminished inci-
were similar in suggesting that low-dose maintenance
dence of tardive dyskinesia. In light of the overall twofold
increase in the risk of relapse, this approach is difficult to
oral medication), but in addition providing some further
justify. On the other hand, the intermittent approach may
protection against relapse for several weeks, allowing all
be useful to those patients who adamantly refuse to take
interested parties to respond to this “crisis.”
It is noteworthy that all of these studies involving
Conclusion
alternative maintenance treatment strategies used depotantipsychotic drugs. The reason for this method is that
Considerable progress has been made in multiple areas of
investigators attempting to make comparisons between
schizophrenia research. Undoubtedly, these advances will
different dosage levels or different strategies for adminis-
help to set the stage for further gains. At present, there are
tration need to be absolutely certain that the patient is
more new antipsychotic drugs and more activity in drug
taking the medication as prescribed. The only way that it
development than at any time in the past three decades.
has been possible to ensure compliance up until now has
New generation medications are demonstrating important
been by giving long-acting injectible medications. It is
advantages over conventional drugs, particularly in the
ironic, however, that in clinical practice these drugs are
area of adverse neurologic effects. Further research will
used far less frequently (Glazer and Kane 1992). Now,
clarify their impact on negative symptoms, depression,
with the introduction of a new generation of antipsychotic
cognitive dysfunction, suicidal ideation or behavior, and,
drugs, which appear to be associated with a lower risk of
ultimately, the most critical domain of functional outcome.
neurologic adverse effects, the clinician faces a dilemma
The improved benefit-to-risk ratio of new drugs should
in terms of patients who are potentially noncompliant.
reduce ambivalence about long-term treatment and en-
None of the new drugs are currently available in a
hance the possibility of early intervention in prodromal
long-acting injectible form. It is assumed that the reduc-
tion in adverse effects expected over long-term treatment
It is critical that methodologic rigor and replication of
with the new antipsychotic drugs will lead to a reduction
findings as well as appropriate knowledge transfer be
in rates of noncompliance. However, this hypothesis
facilitated to solidify and implement the gains that have
remains untested so far and it is also clear to clinicians and
investigators that adverse effects of medication do notexplain all of the variance in the development of noncom-pliance. We continue, therefore, to be faced with the
This work was supported by the following NIMH grants: MH 31776; MH
dilemma of increasing our certainty of preventing relapse,
32369; MH 3992; MH 41960; MH 42929; MH 46633.
This work was presented at the conference, “Schizophrenia: From
but also increasing the potential risk of adverse effects
Molecule to Public Policy,” held in Santa Fe, New Mexico, in October
such as tardive dyskinesia. It is hoped that new medication
1998. The conference was sponsored by the Society of Biological
delivery methods will become available for the new
Psychiatry through an unrestricted educational grant provided by Eli Lily
generation antipsychotic drugs to resolve this dilemma.
Another interesting aspect of long-acting injectible
medication is the suggestion that even following the
References
discontinuation of such drugs, relapse rates are reducedbecause of the very gradual withdrawal resulting from the
Albanese MJ, Khantzian EJ, Mercy FL, Green AI (1994):
pharmacokinetic properties of these agents. Viguera et al
Decreased substance use in chronically psychotic patientstreated with clozapine. Am J Psychiatry 151:780 –781.
(1997) reported that with abrupt cessation of oral antipsy-
Arranz M, Collier D, Sodhi M, et al (1995): Association between
chotic drugs the relapse rate reached 50% within 30
clozapine response and allelic variation in 5-HT 2A receptor
weeks, with little additional risk thereafter up to 3.7 years.
The risk was lower, however, after gradual discontinuation
Arvanitis LA, Miller DG and the Seroquel Trial Thirteen Study
of oral treatment. A similar finding was reported by
Group (1997): Multiple fixed doses of “SEROQOUEL”
Gilbert et al (1995) in their review of the literature on
(quetiapine) in patients with acute exacerbation of schizo-
discontinuation of maintenance medication. The conclu-
phrenia: a comparison with haloperidol and placebo. Biol
sions that can be drawn from these reviews are tentative
because of methodologic concerns (lack of random assign-
Baldacchino AM, Stubbs JH, Nevison-Andrews D (1998): The
use of olanzapine in non-compliant or treatment-resistant
ment in comparison groups, etc.); however, this finding
clozapine populations in hospital. Pharm J 260:207–209.
should be considered in planning future studies.
Beasley CM, Tollefson G, Tran P, et al (1996): Olanzapine
Depot medications, therefore, have the advantage of not
versus placebo and haloperidol: acute phase results of the
only making it clear to family members and clinicians
North American double-blind olanzapine trial. Neuropsycho-
when medication has been discontinued (which may not
necessarily be the case when an individual is receiving
Bjorndal N, Bjerre M, Gerlach J, et al (1980): High dosage
haloperidol therapy in chronic schizophrenic patients: a dou-
Essock SM, Hargreaves WA, Covell NH, Goethe J (1996a):
ble-blind study of clinical response, side effects, serum
Clozapine’s effectiveness for patients in state hospitals: re-
haloperidol, and serum prolactin. Psychopharmacology 67:
sults from a randomized trial. Psychopharmacol Bull 32:683–
Bondolfi G, Dufour H, Patris M, et al (1998): Risperidone versus
Essock SM, Hargreaves WA, Dohm F-A, Goethe J, Carver L,
clozapine in treatment-resistant chronic schizophrenia: a ran-
Hipshman L (1996b): Clozapine eligibility among state hos-
domized double-blind study. Am J Psychiatry 155:499 –504.
pital patients. Schizophr Bull 22:15–25.
Borison RL, Pathiraja AP, Diamond BI, Meibach RC (1992):
Flynn SW, MacEwan GW, Altman S, Kopala LC (1998): An
Risperidone; clinical safety and efficacy in schizophrenia.
open comparison of clozapine and risperidone. Pharmacopsy-Psychopharmacol Bull 28:213–218.
Breier A, Buchanan RW, Kirkpatrick B, et al (1994): Effects of
Gilbert PL, Harris NJ, McAdams LA, Jeste DV (1995): Neuro-
clozapine on positive and negative symptoms in outpatients
leptic withdrawal in schizophrenic patients: a review of the
with schizophrenia. Am J Psychiatry 151:20 –26.
literature. Arch Gen Psychiatry 52:173–188.
Breier A, Hamilton SH (1999): Comparative efficacy of olanza-
Glazer WM, Kane JM (1992): Depot neuroleptic therapy: an
pine and haloperidol for patients with treatment-resistant
underutilized treatment option. J Clin Psychiatry 53:426 –
schizophrenia. Biol Psychiatry 45:403– 411.
Buckley P, Thompson P, Way L, Melter HY (1994): Substance
Gold JM, Harvey PD (1993): Cognitive deficits in schizophrenia.
abuse among patients with treatment-resistant schizophrenia:
Psychiatr Clin North Am 16:295–312.
characteristics and implications for clozapine in therapy. Am J
Goldman RS, Bates JA, Bilder RM, Kane J, Schooler N, Marter
S (1996): The effects of clozapine and haloperidol on mem-
Canadian Cognition and Outcome Study Group (1998): Neuro-
psychological change in early phase schizophrenia over
twelve months of treatment with olanzapine, risperidone orhaloperidol. Schizophr Res 29:152–153.
Green MF (1996): What are the functional consequences of
neurocognitive deficits in schizophrenia? Am J Psychiatry
Carpenter WT Jr, Conley RR, Buchanan RW, Breier A, Tam-
minga CA (1995): Patient response and resource manage-ment: another view of clozapine treatment of schizophrenia.
Green MF, Marshal VD, Wirshing WC, et al (1997): Risperidone
Am J Psychiatry 152:827– 832.
effects on verbal working memory. Schizophr Res 24:214.
Carpenter WT Jr, Hanlon TE, Heinrichs DW, et al (1990):
Hagger C, Buckley P, Kenny JT, Freedman L, Ubogy D, Meltzer
Continuous versus targeted medication in schizophrenic out-
HY (1993): Improvement in cognitive functions and psychi-
patients: outcome results. Am J Psychiatry 147:1138 –1148
atric symptoms in treatment-refractory schizophrenic patients
[Erratum, Am J Psychiatry 1991;148:819].
receiving clozapine. Biol Psychiatry 34:702–712.
Casey DE (1989): Clozapine: neuroleptic-induced EPS and
Hegarty JD, Baldessarini RJ, Tohen M, Waternaux C, Open G
tardive dyskinesia. Psychopharmacology 99(suppl):S47–S53.
(1994): One hundred years of schizophrenia: a meta-analysisof the outcome literature. Am J Psychiatry 151:1409 –1416.
Ceskova E, Svestka J (1993): Double-blind comparison of
risperidone and haloperidol in schizophrenia and schizoaffec-
Herz MI, Glazer WM, Mostert MA, et al (1991): Intermittent vs
tive psychoses. Pharmacopsychiatry 26:121–124.
maintenance medication in schizophrenia: two-year results.
Chouinard G, Jones B, Remington G, et al (1993): A Canadian
Arch Gen Psychiatry 48:333–339.
multicenter placebo-controlled study of fixed doses of risperi-
Herz MI, Liberman RP, Lieberman Ja, et al (1997): American
done and haloperidol in the treatment of chronic schizo-
Psychiatric Association practice guideline for the treatment of
phrenic patients. J Clin Psychopharmacol 13:25– 40 [Erra-
patients with schizophrenia. Am J Psychiatry 154(suppl):1–
tum, J Clin Psychopharmacol 1993;13:149].
Christison GW, Kirch DG, Wyatt RJ (1991): When symptoms
Hogarty GE, McEvoy JP, Munetz M, et al (1988): Dose of
persist choosing among alternative somatic treatments for
fluphenazine, familial expressed emotion, and outcome in
schizophrenia. Schizophr Bull 17:217–245.
schizophrenia results in a two-year controlled study. Arch
Claus A, Bollen J, De Cuyper H, et al (1992): Risperidone versus
Gen Psychiatry 45:797– 805.
haloperidol in the treatment of chronic schizophrenic inpa-
Hogarty GE, Schooler N, Ulorich RF, Mussare F, Ferro P,
tients: a multicentre double-blind comparative study. Acta
Horron E (1979): Fluphenazine and social therapy in the
Psychiatr Scand 85:295–305.
aftercare of schizophrenic patients: relapse analysis of two-
Conley RR, Taminga CA, Bartko JJ, et al (1998): Olanzapine
year controlled study of fluphenazine decanoate and fluphen-
compared with clopromazine in treatment-resistant schizo-
azine hydrochloride. Arch Gen Psychiatry 36:1283–1294.
phrenia. Am J Psychiatry 155:914 –920.
Janicak PG, Davis JM, Preskorn SH, Ayd FJ Jr (1993): Princi-
Davis JM (1975): Overview: maintenance therapy in psychiatry. ples and Practice of Psychopharmacotherapy. Baltimore:
I. Schizophrenia. Am J Psychiatry 132:1237–1245.
Williams & Wilkins, pp 104 –106.
Davis JM, Matalon L, Watanabe MD, Blake L (1994): Depot
Johnson DA, Ludlow JM, Street K, Taylor RD (1987): Double-
antipsychotic drugs: place in therapy. Drugs 47:741–773
blind comparison of half-dose and standard-dose flupenthixol
[Erratum, Drugs 1994;48:616].
decanoate in the maintenance treatment of stabilized out-
Erlenmeyer-Kimling L, Cornblatt BA, Rock D, et al (1993): The
patients with schizophrenia. Br J Psychiatry 151:634 – 638.
New York High-Risk Project: Anhedonia, attentional devi-
Jolley AG, Hirsch SR, McRink A, Manchanda R (1989): Trial of
ants, and psychopathology. Schizophr Bull 19:141–153.
brief intermittent neuroleptic prophylaxis for selected schizo-
phrenic outpatients: clinical outcome at one year. Br Med J
Malhotra AK, Goldman D, Ozaki N, Breier A, Buchanan R,
Pickar D (1996): Lack of association between poly-mor-
Jolley AG, Hirsch SR, Morrison E, McRink A, Wilson L (1990):
phisms in the 5-HT 2A receptor gene and the antipsychotic
Trial of brief intermittent neuroleptic prophylaxis for selected
response to clozapine. Am J Psychiatry 153:1092–1094.
schizophrenic outpatients: clinical and social outcome at two
Mallya AR, Roos PD, Roebuck-Colgan K (1992): Restraint,
seclusion and clozapine. J Clin Psychiatry 53:395–397.
Kane JM (1985): Compliance issues in outpatient treatment.
Marder SR, Meibach RC (1994): Risperidone in the treatment of
J Clin Psychopharmacol 5:22S–27S.
schizophrenia. Am J Psychiatry 151:825– 835.
Kane JM (1995): Tardive dyskinesia: epidemiological and clin-
Marder SR, Van Putten T, Mintz J, et al (1984): Costs and
ical presentation. In: Bloom FE, Kupfer DJ, editors. Psycho-
benefits of two doses of fluphenazine. Arch Gen Psychiatrypharmacology: The Fourth Generation of Progress. New
Marder SR, Van Putten T, Mintz J, Lebell M, McKenzie J, May
Kane JM (1996a): Who shall decide when doctors disagree?
PR (1987): Low-and conventional-dose maintenance therapy
Am J Psychiatry 153:1507–1508.
with fluphenazine decanoate: two-year outcome. Arch Gen
Kane JM (1996b): Schizophrenia. N Engl J Med 334:34 – 41.
Kane JM, Borenstein M (1985): Compliance in the long-term
Martin J, Gomez J-C, Garcia-Bernardo E, Cuesta M, Alvarez E,
treatment of schizophrenia. Psychopharmacol Bull 21:23–27.
Gurpegui M (1997): Olanzapine and treatment-refractoryschizophrenia: results of an open-label study. J Clin Psychi-
Kane JM, Davis JM, Schooler NR, Marder SR, Brauzer B, Casey
DE (1993a): A one-year comparison of four dosages ofhaloperidol decanoate [abstract]. Schizophr Res 9:239 –240.
Meltzer HY (1995): Clozapine: is another view valid? Am J
Kane JM, Honigfeld G, Singer J, Meltzer H and the Clozaril
Collaborative Study Group (1988): Clozapine for the treat-
Meltzer HY, Okayli O (1995): Reduction of suicidality during
ment-resistant schizophrenic: a double blind comparison with
clozapine treatment of neuroleptic-resistant schizophrenia:
clopromazine. Arch Gen Psychiatry 45:789 –796.
impact on risk– benefit assessment. Am J Psychiatry 152:183–190.
Kane JM, Lieberman JA (1987): Maintenance pharmacotherapy
in schizophrenia. In: Meltzer HY, editor. Psychopharmacol-
Muller-Spahn F (1992): Risperidone in the treatment of chronic
ogy: The Third Generation of Progress. New York: Raven
schizophrenic patients: an international double-blind parallel-
group study versus haloperidol. Clin Neuropharmacol15(suppl 1):90A–91A.
Kane JM, Rifkin A, Quitkin F, Klein DF (1976): Antipsychotic
drug blood levels and clinical outcome. In: Klein DF, Gittel-
Peuskens J, Link CGG (1997): A comparison of quetiapine and
man-Klein R, editors. Progress in Psychiatric Drug Treat-
clopromazine in the treatment of schizophrenia. Acta Psychi-ment. New York: Brunner Mazel, pp 399 – 408.
Kane JM, Rifkin A, Woerner MG, et al (1983): Low-dose
Pickar D, Owen RR, Litman RE, Konicki E, Gutierrez R,
neuroleptic treatment of outpatient schizophrenia. I. Prelimi-
Rappoport MH (1992): Clinical and biologic response to
nary results for relapse rates. Arch Gen Psychiatry 40:893–
clozapine in patients with schizophrenia: crossover compari-
son with fluphenazine. Arch Gen Psychiatry 49:345–353.
Kane JM, Smith J (1982): Tardive dyskinesia: prevalence and
Pietzcker A, Gaebel W, Kopcke W, et al (1993): Intermittent
risk factors 1959 –1979. Arch Gen Psychiatry 39:473– 481.
versus maintenance neuroleptic long-term treatment in
Kane JM, Woerner MG, Pollack S, Safferman AZ, Lieberman JA
schizophrenia—2-year results of German multicenter study.
(1993b): Does clozapine cause tardive dyskinesia? J ClinJ Psychiatr Res 27:321–339.
Pollack S, Woerner MG, Howard A, Fireworker RB, Kane JM
Kane JM, Woerner MG, Sarantakos S (1986): Depot neurolep-
(1998): Clozapine reduces rehospitalization among schizo-
tics: a comparative review of standard, intermediate, and
phrenia patients. Psychopharmacol Bull 34:89 –92.
low-dose regimens. J Clin Psychiatry 47(suppl):30 –33.
Prien RF, Cole JO (1968): High dose of chlorpromazine in
Kinon BJ, Kane JM, Johns C, Perovich R, Ismi M, Koreen A
chronic schizophrenia. Arch Gen Psychiatry 18:482– 495.
(1993): Treatment of neuroleptic resistant schizophrenic re-
Quitkin F, Rifkin A, Klein D (1975): Very high dosage vs.
lapse. Psychopharmacol Bull 29:309 –314.
standard dosage fluphenazine in schizophrenia. A double-
Kissling W, editor (1991): Guidelines for Neuroleptic Relapse
blind study of non-chronic treatment-refractory patients. ArchPrevention in Schizophrenia. Berlin, Germany: Springer-
Gen Psychiatry 32:1276 –1281.
Regier DA, Farmer ME, Rae DS, et al (1990): Co-morbidity of
Klein DF, Davis JM (1969): Diagnosis and Drug Treatment of
mental disorders with alcohol and other drug abuse. JAMAPsychiatric Disorders. Baltimore: Williams & Wilkins.
Klieser E, Lehman E, Kinzler E, et al (1995): Randomized,
Remington G, Pollock B, Voineskos G, Reed K, Coulter K
double-blind controlled trial of risperidone versus clozapine
(1993): Acutely psychotic patients receiving high-dose halo-
in patients with chronic schizophrenia. J Clin Psychophar-
peridol therapy. J Clin Psychopharmacol 13:41– 45.
Rifkin A, Doddi S, Karajgi B, Borenstein M, Wachspress M
Levinson DF, Simpson GM, Singh H, et al (1990): Fluphenazine
(1991): Dosage of haloperidol for schizophrenia. Arch Gen
dose, clinical response, and extrapyramidal symptoms during
acute treatment. Arch Gen Psychiatry 47:761–768.
Rosenheck R, Cramer J, Xu W, et al (1997): A comparison of
clozapine and haloperidol in hospitalized patients with refrac-
Tollefson GD, Sanger TM, Lou Y, Thieme ME (1998): Depres-
tory schizophrenia. N Engl J Med 337:809 – 815.
sive signs and symptoms in schizophrenia: a trial of olanza-
Schooler N (1998, May): Comparing new anti-psychotic medi-
pine and haloperidol. Arch Gen Pyschiatry 55:250 –258. cations: what do the data say. Presented at the Society of
Tran PV, Hamilton SH, Kuntz AJ, et al (1997): Double-blind
Biological Psychiatry Annual Meeting, Toronto Canada.
comparison of olanzapine versus risperidone in the treatment
Schooler NR, Keith SJ, Severe JB, et al (1997): Relapse and
of schizophrenia and other psychotic disorders. J Clin Psy-
reshospitalization during maintenance treatment of schizo-
phrenia. Arch Gen Psychiatry 54:453– 463.
Van Putten T, Marder SR, Mintz J (1990): A controlled dose
Shalev A, Hermash H, Rothberg J, Munitz H (1993): Poor
comparison of haloperidol in newly admitted schizophrenic
neuroleptic response in acutely exacerbated schizophrenic
patients. Arch Gen Psychiatry 47:754 –758.
patients. Acta Psychiatr Scand 87:86 –91.
Viguera AC, Baldessarini RJ, Hegarty JD, et al (1997): Clinical
risk following abrupt and gradual withdrawal of maintenance
Shaner A, Khalsa MA, Roberts L, Wilkins J, Anglin D, Hsieh SC
neuroleptic treatment. Arch Gen Psychiatry 54:49 –55.
(1993): Unrecognized cocaine use among schizophrenic pa-tients. Am J Psychiatry 150:758 –762.
Volavka J, Cooper T, Czobor P, et al (1992): Haloperidol blood
levels and clinical effects. Arch Gen Psychiatry 49:354 –361.
Tollefson GD, Beasley CM Jr, Tamura RN, Tran PV, Potvin JH
(1997a): Blind, controlled, long-term study of the compara-
Wahlbeck K (1998, February 7–13): Evidence of clozapine
tive incidence of treatment-emergent tardive dyskinesia with
effectiveness in schizophrenia. Presented at the Ninth Bien-
olanzapine or haloperidol. Am J Psychiatry 154:1248 –1254.
nial Winter Workshop on Schizophrenia, Davos Switzerland.
Tollefson GD, Beasley CM, Tran P, Street JS, Kruger JA,
Weiden PJ, Olfson M (1995): Cost of relapse in schizophrenia.
Tamura RN (1997b): Olanzapine versus haloperidol and the
Schizophr Bull 21:419 – 429.
treatment of schizophrenia and schizoaffective and schizo-
Zimbroff DL, Kane JM, Tamminga CA, et al (1997): A con-
phreniform disorders: results of an international collaborative
trolled, dose–response study of sertindole and haloperidol in
trial. Am J Psychiatry 154:457– 465.
schizophrenia. Am J Psychiatry 154:782–791.
NUOVO REGOLAMENTO ANTIDOPING CODICE MONDIALE ANTIDOPING RELAZIONE 2007 PROF ANTONIO SPATARO MEDICO FEDERALE FEDERAZIONE ITALIANA CANOTTAGGIO Il 01-01-2004 e’ entrato in vigore il nuovo regolamento antidoping della Agenzia Mondiale Antidoping (WADA), organismo creato per garantire l’armonizzazione e la migliore pratica dei programma antidoping internazionale
The Truth about Prescription Drugs like Prilosec , Prevacid and Nexium , and Over-the-Counter Antacids Lyle Loughry Copyright--August 2008 If you're one of the 100 million Americans who suffer from Heartburn, Indigestion, Bloating, Diarrhea, Upset stomach, Acid indigestion, Embarrassing gas, Occasional constipation, and a host of other digestive problems … most l
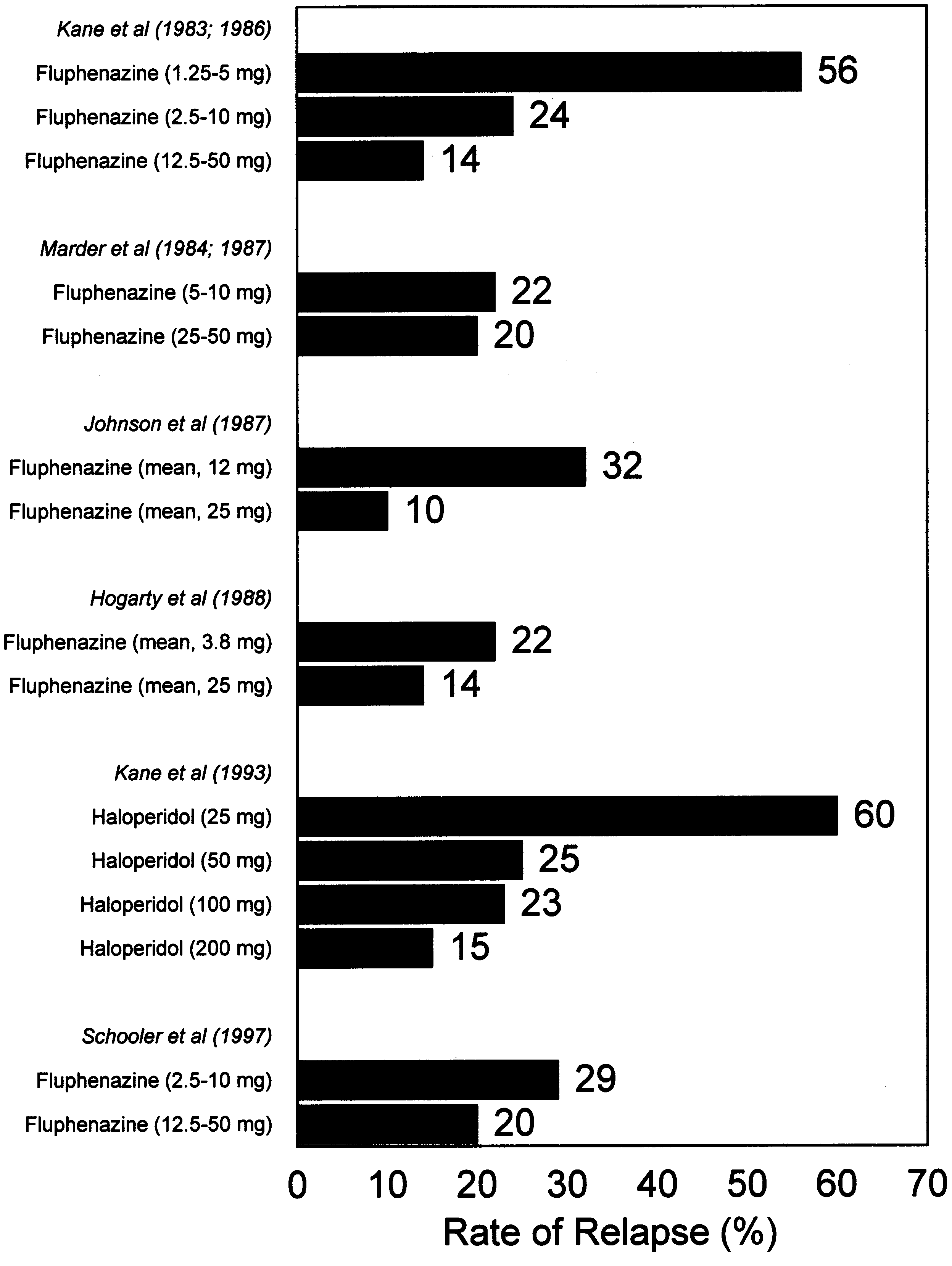 Figure 1. Cumulative rates of relapse amongpatients with schizophrenia after 1 year of main-tenance therapy with various doses of antipsy-chotic drugs, in six studies. Most patients hadhad more than one prior psychotic episode.
Figure 1. Cumulative rates of relapse amongpatients with schizophrenia after 1 year of main-tenance therapy with various doses of antipsy-chotic drugs, in six studies. Most patients hadhad more than one prior psychotic episode.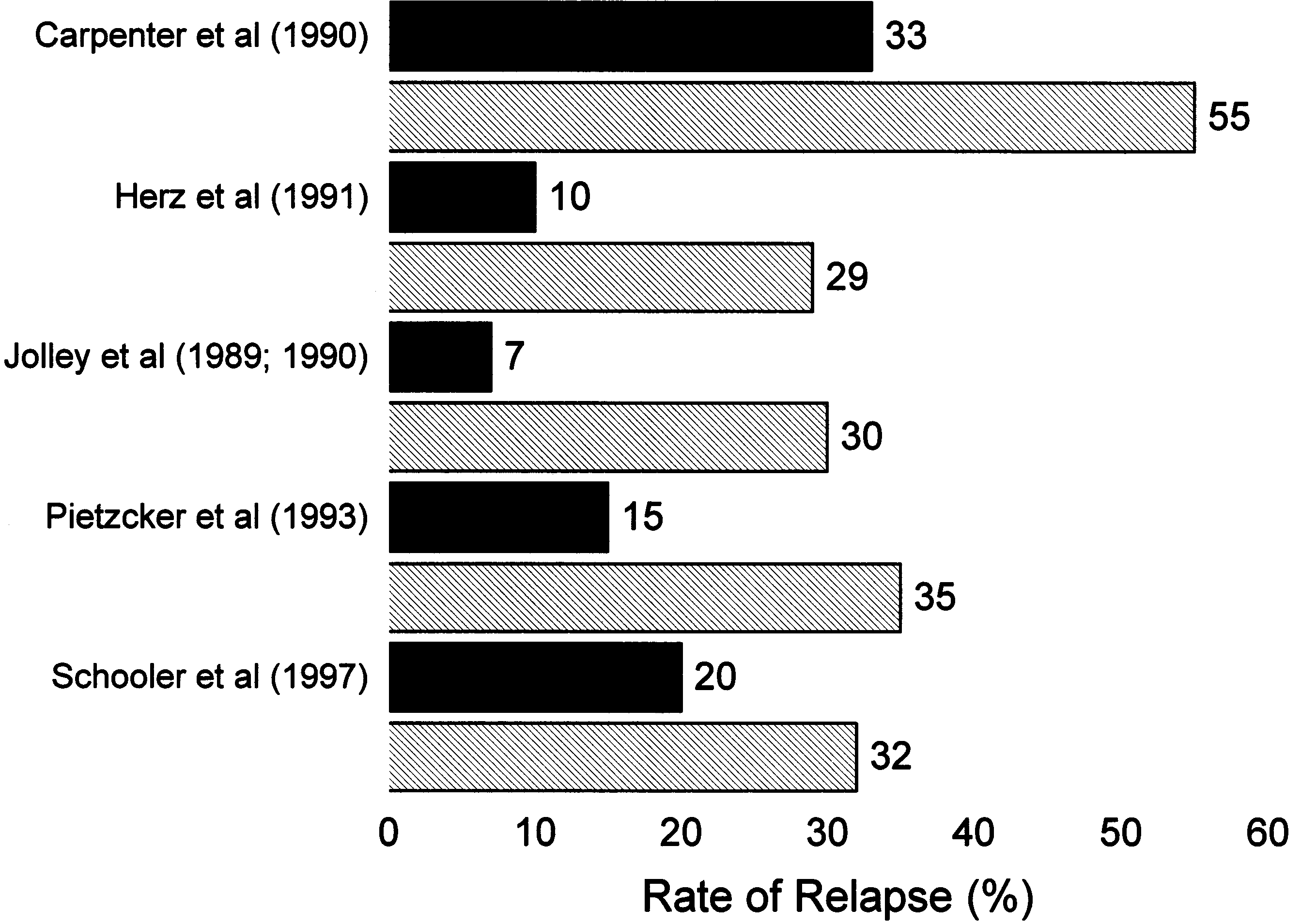 Figure 2. Rates of relapse among patientswith schizophrenia after 1 year of contin-uous or intermittent maintenance therapy,in five studies. Black bars represent con-tinuous treatment, and shaded bars inter-mittent treatment. Most patients had hadmore than one prior psychotic episode.
Figure 2. Rates of relapse among patientswith schizophrenia after 1 year of contin-uous or intermittent maintenance therapy,in five studies. Black bars represent con-tinuous treatment, and shaded bars inter-mittent treatment. Most patients had hadmore than one prior psychotic episode.