Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Edisi 03_2009-utama
Management of Heart Failure in Elderly Patients Idrus Alwi Department of Internal Medicine, Faculty of Medicine, University of Indonesia-dr. Cipto Mangunkusumo Hospital.Jl. Diponegoro no. 71, Jakarta Pusat 10430.Correspondence mail to:[email protected]. ABSTRACT INTRODUCTION Heart failure is a clinical syndrome, associated with high
Heart failure is a clinical syndrome, associated with
mortality and frequent as well as long hospitalization
high mortality and frequent as well as long hospitalization
duration. Several cohort studies in elderly patients with >80
duration.1 The prevalence of heart failure is increasing
years of age for 1 year duration demonstrate a very high
with age.2 Several surveys, e.g. the Euro Heart Failuremortality rate for 3 months and 12 months hospitalization.Survey I (EHFS I),3 reported poor outcome, especially
Major Cardiovascular Events (MACE) observed during
in elderly patients4 since the management is frequently
follow up is also increased significantly. These findings
complicated due to multiple co-morbidity factors.4-7
support the idea that age is a strong predictor and
Moreover, evidence-based therapies are still infrequently
independent concerning mortality in patients with heartfailure. There are different factors associated with mortality
applied and under-prescribing, i.e. giving drug less than
during hospitalization and follow-up.
the recommended dose, is commonly found in elderly
Poor ejection fraction, a strong mortality predictor inyoung people, is not an independent factor in octogenarian
Several cohort studies in elderly patients with >80
population. This owes to the high prevalence of heart
years of age for 1 year duration demonstrate a very high
failure with normal ejection fraction (preserved ejection
mortality rate for 3 months and 12 months hospitalization. fraction), and only one fifth of echocardiography results
Major Cardiovascular Events (MACE) observed during
demonstrate ejection fraction < 30%. The use of ACE-I or
follow up is also increased significantly. These findings
ARBs is associated with better one-year-outcome.
support the idea that age is a strong predictor andindependent concerning mortality in patients with heart
Key words: heart failure, cardiovascular, elderly patients.
There are different factors associated with
mortality during hospitalization and follow-up. Hospital-ization mortality is primarily correlated to acute clinicalconditions; while long-term mortality is associated withdisability14 and the presence of other co-morbidities, suchas diabetes and kidney dysfunction. Previous studyshowed that kidney function is a strong predictor formortality during hospitalization and follow up.15
Poor ejection fraction, a strong mortality predictor in
young people,16 is not an independent factor inoctogenarian population. This owes to the highprevalence of heart failure with normal ejection fraction(preserved ejection fraction), and only one fifth ofechocardiography results demonstrate ejection fraction< 30%. The use of ACE-I or ARBs is associated withbetter one-year-outcome.17-20
AGE AS PREDISPOSITION FOR HEART FAILURE
is a presumption of the existence of other disease, based
Age is one of predisposing factors for the
on the anamnesis and physical examination.
development of heart failure through various mechanisms. First, heart failure is a common outcome for every
THE MANAGEMENT OF HEART FAILURE IN ELDERLY
cardiovascular disease. Thus, patients with
PATIENTS
cardiovascular diseases (such as hypertension, acute
ACC-AHA has recently announced the guideline of
coronary syndrome, heart surgery, etc) tend to develop
heart failure in general23 (not exclusively for elderly
and experience ventricular remodeling and heart failure
patients). The management of heart failure based on the
in their older age. Second, in spite of cardiovascular
diseases, elderly itself is associated with decreasing aortaland left ventricle compliance, and increasing aortal
EXERCISE AND LIFE STYLE MODIFICATION
impedance as well as abnormal left ventricle diastolicfunctions. These conditions lower the threshold of heart
The benefit of exercise on heart failure includes
failure progression when the heart is exposed to
decreasing neuro-hormonal activity, improving
precipitating factors, such as hypertension and/or
endothelial and physiological function of skeletal muscle
tachyarrhythmia (mainly, atrial fibrillation). The last
and the sensation of improved quality of life. Patients
mechanism explains why the clinical manifestation of
shall have education in regard of dietary modification
heart failure in elderly patients is basically different from
syndromes described and studied on randomized clinical
Recommendations
Exercise training is beneficial as an adjunctive
Heart failure is more frequently found in female
approach to improve clinical status in ambulatory
patients because of their longer life expectation age;
patients with current or prior symptoms of heart failure
hence, they tend to suffer more risk of having
and reduced left ventricular systolic function. (Class I,
hypertension, normal left ventricular ejection fraction and
a great number of co-morbidities.21 Compared to youngpeople, elderly patients are more frequently experienc-
PHARMACOLOGICAL TREATMENT FOR HEART
ing inadequate assessment during hospitalization, and
FAILURE IN ELDERLY PATIENTS
more often received under-prescribing or having
Data regarding optimal pharmacological therapy for
treatment less than the recommended dose for life
heart failure in extremely elderly patients (age >80 years)
saving therapies. Age is also a predictor of higher
is very limited. Small studies and sub-group analysis on
large scale clinical trial demonstrates the safety andefficacy of treatment, especially adjusted for elderly
HEART FAILURE DIAGNOSIS IN ELDERLY PATIENTS
patients with congestive heart failure.
Symptoms of heart failure, such as tiredness and
breathing difficulty, may be mistaken as aging process. DIURETICS
Delirium, the presence of decreasing functional status,
Diuretics are prescribed to all patients who have
recent peripheral edema, or nocturnal symptoms (cough,
evidence of symptoms or signs of pulmonary or systemic
dyspnea) calls for further evaluation in regard of heart
congestion. Once daily dose is more preferred.
Moreover, renal function and electrolyte balance should
The basic examination for heart failure in elderly
be monitored during treatment Patients who have
patients is not significantly different, i.e.: complete blood
hypo-perfusion symptoms or exaggerated kidney
count, routine biochemistry, including liver and kidney
insufficiency during the titration of neuro-hormonal
function test, NT-proBNP test, chest x-ray and electro-
blockade treatment should reduce their diuretics dose.
cardiography (ECG). Just as in young patients, objective
For long-term treatment, diuretics dose can be altered
assessment of left ventricle function should be performed
several times to allow other drugs titration, and to obtain
by means of echocardiography. Patients who seem to
the lowest dose that can stabilize body weight and
be having acute pulmonary edema must undergo
examination and evaluation to find out the etiology thattriggers the development of disease (infection, ischemia,
Recommendation
arrhythmia, change of drug regimens or non-compliance
Diuretics and salt restriction are indicated in patients
to therapy). Other examination depends on whether there
with current or prior symptoms of heart failure and
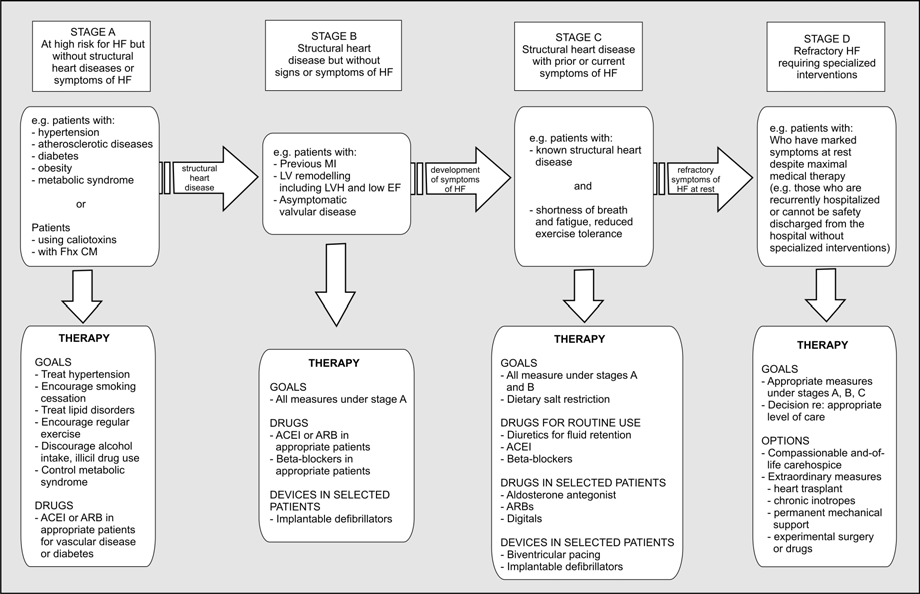
Management of Heart Failure in Elderly Patients
Figure 1. Algorithm of heart failure management
reduced left ventricular systolic function who have
pressure should be measure in standing, sitting and lying
evidence of fluid retention. (Class I, Level of Evidence:
position. The renal function and potassium serum level
should be evaluated after altering ACE inhibitors anddiuretics dose or if there is any change in clinical
ANGIOTENSIN CONVERTING ENZYME (ACE) INHIBITOR
Angiotensin converting enzyme (ACE) inhibitor
ACE inhibitor study in elderly patients is reported on
PEP-HF study28 (Perindopril in Elderly People with
should be considered for all elderly patients with chronic
Chronic Heart Failure). The incidence of primary
heart failure, although the data regarding the effective-
endpoint all-cause death or heart failure hospitalization
ness of this drug in elderly patients is still limited.
tend to be reduced with perindopril than with placebo in
CONSENSUS study24 (enalapril) excludes patients who
one year time [hazard ratio (HR) 0.69, 95% confidence
are over 75 years, and SOLVD study25 (enalapril) and
interval (CI) 0.47 – 1.01; P=0.055]. However, such
SAVE study26 (captopril) exclude patients who are over
tendency was not found at the end of this study [HR
80 years. AIRE study27 (ramipril) does not exclude
patients based on age alone, and there is a tendencytoward better end-result in population of over 65 years,
Recommendation
however, the sample size is not large enough to achieve
Angiotensin converting enzyme inhibitors are
recommended for all patients with current or prior
When performing ACE inhibitors dose titration in
symptoms of heart failure and reduced left ventricular
elderly patients, it is important to start with low dose and
systolic function, unless contraindicated. (Class I, Level
increase gradually in accordance with the target dose in
clinical trial or maximal lower dose that can still betolerated. Diuretics dose can be reduce if there is no
ANGIOTENSIN II RECEPTOR BLOCKERS
water retention, to maintain stable blood pressure.In
VAL-HEFT study29 (Valsartan Heart Failure Trial),
several elderly patients, it would be more helpful if the
with mean age of 63±11 years old (47% patients were
consumption time of ACE inhibitor and diuretics are
> 65 years), and CHARM study30 (Candesartan in Heart
separated, to prevent peak hemodynamic effect. Blood
Failure Assessment of Reduction in Mortality and
Morbidity), with mean age of 66±11 years old (23%
SPIRONOLACTONE
patients were >75 years), demonstrate the benefit of
Study on the role of aldosterone antagonist in elderly
ARB on similar outcome in patients <65 years of >65
patients is still lacking. Low- dose spironolactone (mean
26 mg/day) has been researched on RALES study36(Randomized Aldactone Evaluation Study). Subjects of
Recommendation
Angiotensin II receptor blockers are recommended
RALES study were population with mean age of 65
in all patients with current or prior symptoms of heart
years with severe heart failure (NYHA III-IV, LVEF
failure and reduced left ventricular systolic function, who
< 35%), who had been receiving ACE inhibitors and loop
are ACE inhibitor-intolerant. (Class I, Level of Evidence:
diuretics treatment. However, patients with renal
dysfunction (creatinine level > 220 μmol/L) or with othersignificant co-morbidities were excluded. Spironolactonedecreases mortality about 30%, as well as hospitalization
BETA BLOCKERS
due to heart failure as much as 35% and significantly
Beta blockers are also beneficial for elderly patients,
improves NYHA functional class. Thus, low dose
since there is greater role of activation of sympathetic
spironolactone is recommended for patients with severe
nervous system compared to the renin-angiotensin
heart failure, albeit having received optimal medical
system. CIBIS II study31, MERIT HF study32, and
management. Gynecomastia occurs in 10% male patients.
COPERNICUS study33 demonstrate that beta blockers
Also have to bear in mind that potassium and renal
can increase survival as much as 30-35% and also
function were routinely monitored in this study, i.e. on
increase left ventricle systolic function. The mean age
the 1st, 2nd, 3rd, 6th, 9th and 12th month and then 6 months
of the patients in randomized clinical trial meta-analysis
later. With strict monitoring, we expect that
range from 60 to 65 years, and < 30% patients were
hyperkalemia and renal dysfunction will not occur. Oral
> 70 years and there were very few patients who were
potassium supplement is not required, unless there is
>80 years. Sub-group analysis shows that there is no
significant interaction between age and the effect of beta
Sub-group analysis on RALES study demonstrates
blockers effect on the outcome.34 Beta blockers should
effect on similar outcome of patients with <67 years and
be started with the lowest dose, increase gradually in
>67 years of age. Moreover, age is associated with
weeks up to months duration. Monitoring shall be
increased side effects, particularly hyperkalemia.22
performed on heart rate, blood pressure and patients’
Spironolactone study in patients who have heart failure
and ejection fraction > 45% is currently being conducted
The role of beta blockers nebivolol in elderly patients
and it will evaluate whether spironolactone is effective
who have heart failure (> 70 years) with normal left
for heart failure with normal ejection fraction.
ventricle systolic function (diastolic heart failure) wasreported in the SENIORS study.35 There was a decline
Recommendation
Addition of aldosterone antagonist is recommended
of primary outcome (all-cause mortality or cardiovascu-
in selected patients with moderately severe to severe
lar hospitalization) of lower rate compared to other
symptoms of heart failure and reduced left ventricular
previous beta blockers studies [HR 0.86; 95% CI 0.74 –
systolic function, who can be carefully monitored for
0.99; P=0.039]; and it was also different from previous
preserved renal function and normal potassium level.
studies which had young patients as study subjects, since
Creatinine level should be < 2.5 mg/dL for male and <2.0
it did not affect the mortality [HR 0.88; 95% CI 0.71 –
mg/dL for female and potassium should be < 5 mEq/L.
1.08; P=0.21]. In sub-group analysis, nebivolol effect on
primary outcome was significant in patients <75 years(median value), but it was not significant in patients >75years.
Study of digitalis on heart failure, which is called DIG
Recommendation
(Digitalis Investigation Group) reported the advantages
Beta blockers (using 1 from 3 proven to reduce
of digoxin for stable heart failure, particularly in patients
mortality, i.e. bisoprolol, carvedilol and sustained release
with left ventricle systolic dysfunction (LVEF < 45%).
metoprolol succinate) are recommended for stable
In addition, the other several small adjunct studies are
patients with current or prior symptoms of heart failure
also evaluating patients with LVEF > 45%. Twenty seven
and reduced left ventricular systolic function, unless
percent subjects were > 70 years. The benefit of treat-
contraindicated. (Class I, Level of Evidence: A)23
ment in decreasing hospitalization was demonstrated in
Management of Heart Failure in Elderly Patients
all age groups.37 However, increased age was associ-
Cardiologists and the French Geriatrics Society. Eur Heart J.
ated with higher rate of hospitalization due to assumed
12. Lee DS, Austin PC, Rouleau JL,et al. Predicting mortality among
patients hospitalized for heart failure: derivation and
mortality rate. In DIG study, digoxin dose was managed
validation of a clinical model. JAMA. 2003;290:2581–7.
by using an algorithm in accordance with age, sex, weight
13. Pocock SJ, Wang D, Pfeffer MA, et al. Predictors of mortality
and renal function.38 Digoxin should be used cautiously
and morbidity in patients with chronic heart failure. Eur Heart
(particularly for those with renal dysfunction). It may
14. Cacciatore F, Abete P, Mazzella F, et al. Frailty predicts longterm
alleviate patients’ complains and decrease hospitalization
mortality in elderly subjects with chronic heart failure. Eur J
for patients with severe heart failure symptoms and very
15. Smith GL, Lichtman JH, Bracken MB, et al. Renal impairment
In the sub-study, which was conducted in parallel
and outcomes in heart failure: systematic review and meta-
with the main study, there were almost 1000 patients
analysis. J Am Coll Cardiol. 2006;47:1987–96.
16. Vasan RS, Larson MG, Benjamin EJ, et al. Congestive heart
with had heart failure and normal systolic function, who
failure in subjects with normal versus reduced left ventricular
were usually elderly patients. Digoxin demonstrated a
ejection fraction: prevalence and mortality in a population-
tendency of early advantage on improved outcome,
based cohort. J Am Coll Cardiol. 1999;33:1948–55.
although it is difficult to explain the underlying
17. Masoudi FA, Rathore SS, Wang Y, et al. National patterns of use
and effectiveness of angiotensin converting enzyme
inhibitors in older patients with heart failure and leftventricular systolic dysfunction. Circulation. 2004;110:724–31.
18. Gianni M, Bosch J, Pogue J, et al. Effect of long-term ACE-
REFERENCES
inhibitor therapy in elderly vascular disease patients. Eur HeartJ. 2007;28:1382–8.
Redfield MM. Heart failure—an epidemic of uncertain
19. Havranek EP, Abrams F, Stevens E, et al. Determinants of
proportions. N Engl J Med. 2002;347:1442–4.
mortality in elderly patients with heart failure: the role of
McMurray JJ, Pfeffer MA. Heart failure. Lancet. 2005;365:
angiotensin-converting enzyme inhibitors. Arch Int Med.
Komajda M, Hanon O, Hochadel M, et al. Management of
20. Johnson D, Jin Y, Quan H,et al. Beta-blockers and angiotensin-
octogenarians hospitalized for heart failure in Euro Heart
converting enzyme inhibitors/receptors blockers prescriptions
Failure Survey I. Eur Heart J. 2007;28:1310–8.
after hospital discharge for heart failure are associated with
Mahjoub H, Rusinaru D, Soulie‘re V, et al. Long-term survival
decreased mortality in Alberta, Canada. J Am Coll Cardiol.
in patients older than 80 years hospitalised for heart failure. A
5-year prospective study. Eur J Heart Fail. 2008;10:78–84.
21. Rich MW. Office management of heart failure in the elderly.
Gambassi G, Forman DE, Lapane KL, et al. Management of
heart failure among very old persons living in long-term care:
22. Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC
has the voice of trials spread? The SAGE Study Group. Am
Guidelines for the diagnosis and treatment of acute and chronic
heart failure 2008: the Task Force for the Diagnosis and Treat-
Lien CT, Gillespie ND, Struthers AD, et al. Heart failure in frail
ment of Acute and Chronic Heart Failure 2008 of the European
elderly patients: diagnostic difficulties, co-morbidities,
Society of Cardiology. Developed in collaboration with the
polypharmacy and treatment dilemmas. Eur J Heart Fail.
Heart Failure Association of the ESC (HFA) and endorsed by
the European Society of Intensive Care Medicine (ESICM).
Havranek EP, Masoudi FA,Westfall KA,et al. Spectrum of heart
failure in older patients: results from the National Heart Failure
23. Jessup M, Abraham WT, Casey DE. 2009 Focused Update:
project. Am Heart J. 2002;143:412–7.
ACCF/AHA Guidelines for the Diagnosis and Management of
Heart failure treatment with angiotensin-converting enzyme
Heart Failure in Adults: A Report of the American College of
inhibitors in hospitalized Medicare patients in 10 large states.
Cardiology Foundation/American Heart Association Task Force
The Large State Peer Review Organization Consortium. Arch
on Practice Guidelines: Developed in Collaboration With the
International Society for Heart and Lung Transplantation.
Gustafsson F, Torp-Pedersen C, Seibaek M, et al. DIAMOND
study group. Effect of age on short and long-term mortality in
24. The CONSENSUS tiral study group. Effects of enalapril on
patients admitted to hospital with congestive heart failure. Eur
mortality in severe congestive heart failure; results of the
Cooperative North Scandanavian Enalapril Survival Study
10. Pulignano G, Del Sindaco D, Tavazzi L, et al. IN-CHF
(CONSENSUS). N Engl J Med. 1987;316:1429-35.
Investigators Clinical features and outcomes of elderly
25. The SOLVD Investigators. Effect of enalapril on survival in
outpatients with heart failure followed up in hospital
patients with reduced ejection fractions and congestive heart
cardiology units: data from a large nationwide cardiology
failure. N Engl J Med. 1991;325:293-302.
database (IN-CHF Registry). Am Heart J. 2002;143:45–55.
26. Pfeffer MA, Braunwald E, Moye LA, et al. Effect of captopril
11. Cohen-Solal A, Desnos M, Delahaye F, et al. A national survey
on mortality and morbidity in patients with left ventricular
of heart failure in French hospitals. The Myocardiopathy and
dysfunction after myocardial infarction. Results of the
Heart Failure Working Group of the French Society of
survival and ventricular enlargement trial. The SAVE
Cardiology, the National College of General Hospital
Investigators. N Engl J Med. 1992;327(10):669-77.
27. The Acute Infarction Ramipril Efficacy (AIRE) Study
33. Packer M, Bristow MR, Cohn JN, et al. The effect of carvedilol
Investigators. Effect of ramipril on mortality and morbidity of
on morbidity and mortality in patients with chronic heart
survivors of acute myocardial infarction with clinical evidence
failure. U.S. Carvedilol Heart Failure Study Group. N Engl J
of heart failure. Lancet. 1993;342:821-8.
28. Cleland JG, Tendera M, Adamus J, Freemantle N, Polonski L,
34. Dulin BR, Haas SJ, Abraham WT, et al. Do elderly systolic
Taylor J; PEP-CHF Investigators. The perindopril in elderly
heart failure patients benefit from beta blockers to the same
people with chronic heart failure(PEP-CHF) study. Eur Heart
extent as the non-elderly? Meta-analysis of .12,000 patients in
large-scale clinical trials. Am J Cardiol. 2005;95:896–8.
29. Pfeffer MA, McMurray JJ, Velazquez EJ, et al. Valsartan,
35. Flather MD, Shibata MC, Coats AJ, et al. Randomized trial to
captopril, or both in myocardial infarction complicated by heart
determine the effect of nebivolol on mortality and cardiovascular
failure, left ventricular dysfunction, or both. N Engl J Med.
hospital admission in elderly patients with heart failure
(SENIORS). Eur Heart J. 2005;26:215–25.
30. Granger CB, McMurray JJ, Yusuf S, et al. Effects of candesartan
36. Pitt B, Zannad F, Remme WJ, et al. The effect of
in patients with chronic heart failure and reduced left-
spironolactone on morbidity and mortality in patients with
ventricular systolic function intolerant to angiotensin-
severe heart failure. Randomized Aldactone Evaluation Study
converting enzyme inhibitors: the CHARM-Alternative trial.
Investigators. N Engl J Med. 1999;341(10):709-17.
37. Rich MW, McSherry F, Williford WO, Yusuf S. Digitalis
31. CIBIS-II Investigators and Committee. The Cardiac
Investigation Group. Effect of age on mortality,
Insufficiency Bisoprolol Study II (CIBIS-II): a randomised trial.
hospitalizations and response to digoxin in patients with heart
failure: the DIG study. J Am Coll Cardiol. 2001;38:806–13.
32. Hjalmarson A, Goldstein S, Fagerberg B, et al. Effects of
38. The Digitalis Investigation Group. The effect of digoxin on
controlled release metoprolol on total mortality,
mortality and morbidity in patients with heart failure. N Engl J
hospitalizations, and well-being in patients with heart failure:
the Metoprolol CR/XL Randomized Intervention Trial in
39. Ahmed A, Rich MW, Fleg JL, et al. Effects of digoxin on
congestive heart failure (MERIT-HF). MERIT-HF Study
morbidity and mortality in diastolic heart failure: the ancillary
digitalis investigation group trial. Circulation. 2006;114:397–403.
Clinical Are you short or TALL? Reducing risk of drug errors Keith Underwood Medical Devices Trainer, Scarborough and North East Yorkshire Healthcare NHS Trust Abstract Drug errors pose great risks to patients, that uses capital letters to distinguish similar. However, the system itself is not standardised, and this is a necessary next step to further minimise drug error
Start Thinking About Reducing Secondhand Smoke! Issue Twelve Back to school with Update from the national STARSS community Linda in New Brunswick reported that the Family Wellness Challenge was a Because school-aged success, and she hopes to continue it on an annual basis. STARSS fit into children are headed to the healthy environments piece of the event ver
 Management of Heart Failure in Elderly Patients
Figure 1. Algorithm of heart failure management
Management of Heart Failure in Elderly Patients
Figure 1. Algorithm of heart failure management