Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Paraquat poisoning
Paraquat is a safe and effective herbicide when used as directed on the label. However, exposure to toxic doses of paraquat (largely with suicidal intention) is oftenfatal, despite aggressive medical intervention. Early recognition, and attempts atremoval of paraquat from the body remain the cornerstone of therapy.
In recent years there has been little change in the general management of paraquatpoisoning, but this booklet is structured in a way to emphasise the importance ofearly recognition and early treatment. It also includes a section on the mechanism ofparaquat toxicity, a flow chart to aid early management and an update on the latest
PARAQUAT POISONING
laboratory techniques (and their availability). The booklet has been jointly producedby members of the Health Assessment and Environmental Safety Department ofSyngenta and the Medical Toxicology Unit, Guy’s & St Thomas’ Hospital NHS Trust,
a practical guide to diagnosis, first aid and
This guide aims to present current best practice in the treatment of paraquat
poisoning. However, it needs to be emphasised, that the availability of treatmentmaterials varies enormously between countries and primary health care providersneed to be familiar with local practices and the availability of laboratory analyses. Disclaimer
Although the authors of this booklet have given the advice contained herein in good faith and on thebasis of the best and most recent knowledge available at the time of this booklet going to print, nowarranty is given or may be implied as to the correctness of the advice nor can any liability be acceptedby the authors in respect thereof. Further, the likelihood of success of any treatment will also depend onother extraneous factors over which the authors have no control and which include, for example, thegeneral health of the affected person, the period of time between ingestion and the beginning of thetreatment and the quantity of product which has been ingested. Initial Hospital Management
• Ensure Airway, Breathing and Circulation are intact
Diagnosis
1. 5HT3 antagonists e.g. Ondansetron 8mg (5mg/m2 in children) by slow i.v.
injection or i.v. infusion over 15 minutes, or
2. Phenothiazine anti-emetics e.g. prochlorperazine
• Diagnosis must be made and First Aid initiated without delay.
Dopamine antagonists such as metoclopramide should be avoided as they mayimpair therapy for renal support with dopamine.
• Diagnosis of paraquat poisoning is often made on circumstantial evidence
1. History of paraquat ingestion – from patients or other observers
activated charcoal - 100g for adults or 2 g/kg body weight in children or,
2. Evidence of paraquat ingestion (suicide note, empty container, residue,
Fuller’s Earth - 15% solution; 1 litre for adults or 15ml/kg body weight in
3. Clinical signs, especially with intractable vomiting, or inflammation or
NOTE: The use of gastric lavage without administration of an adsorbent has not
ulceration of mucous membranes (which occurs several hours following
• A purgative should also be used, e.g. mannitol or magnesium sulphate
• Ingestion under certain conditions is unlikely to be serious, including:
1. Ingestion of plants sprayed with dilute paraquat solution
• Rehydrate the patient to optimise renal clearance of paraquat, paying attention to
2. Ingestion of soil sprayed with paraquat
the possibility of fluid overload and electrolyte imbalance.
3. Accidental ingestion of a mouthful of spray-strength paraquat
NOTE: Forced diuresis is not recommended.
• Do not give supplemental oxygen unless serious hypoxia is present First Aid
• If the patient is not vomiting then administer either:
activated charcoal - 100g for adults or 2 g/kg body weight in children or,
Fuller’s Earth - 15% solution; 1 litre for adults or 15ml/kg body weight inchildren.
• A purgative should also be used, e.g. mannitol or magnesium sulphate
• If there is a suspicion of significant ingestion then arrange IMMEDIATE transfer
to hospital following the administration of first aid.
(Fuller’s Earth can be obtained via your local Syngenta office or by e-mail [email protected]). Using Laboratory Analysis for Diagnosis Clinical Features (based on Lock and Wilks 2001)
• Qualitative confirmation of significant paraquat ingestion
• Mild or subacute poisoning: <20 – 30 mg paraquat ion/kg body weight.
urine spot test (alkali and sodium dithionite) as soon as possible (test kits
Asymptomatic or vomiting and diarrhoea.
can be obtained via your local Syngenta office or by e-mail to
Renal and hepatic lesions are minimal or absent.
An initial decrease of the pulmonary diffusion capacity may be present.
a negative urine test should be repeated at 6 hours post-ingestion and if this
Complete recovery would be expected.
is still negative then serious sequelae are unlikely.
• Moderate to severe acute poisoning: >20 – 30 but <40 – 50 mg paraquat
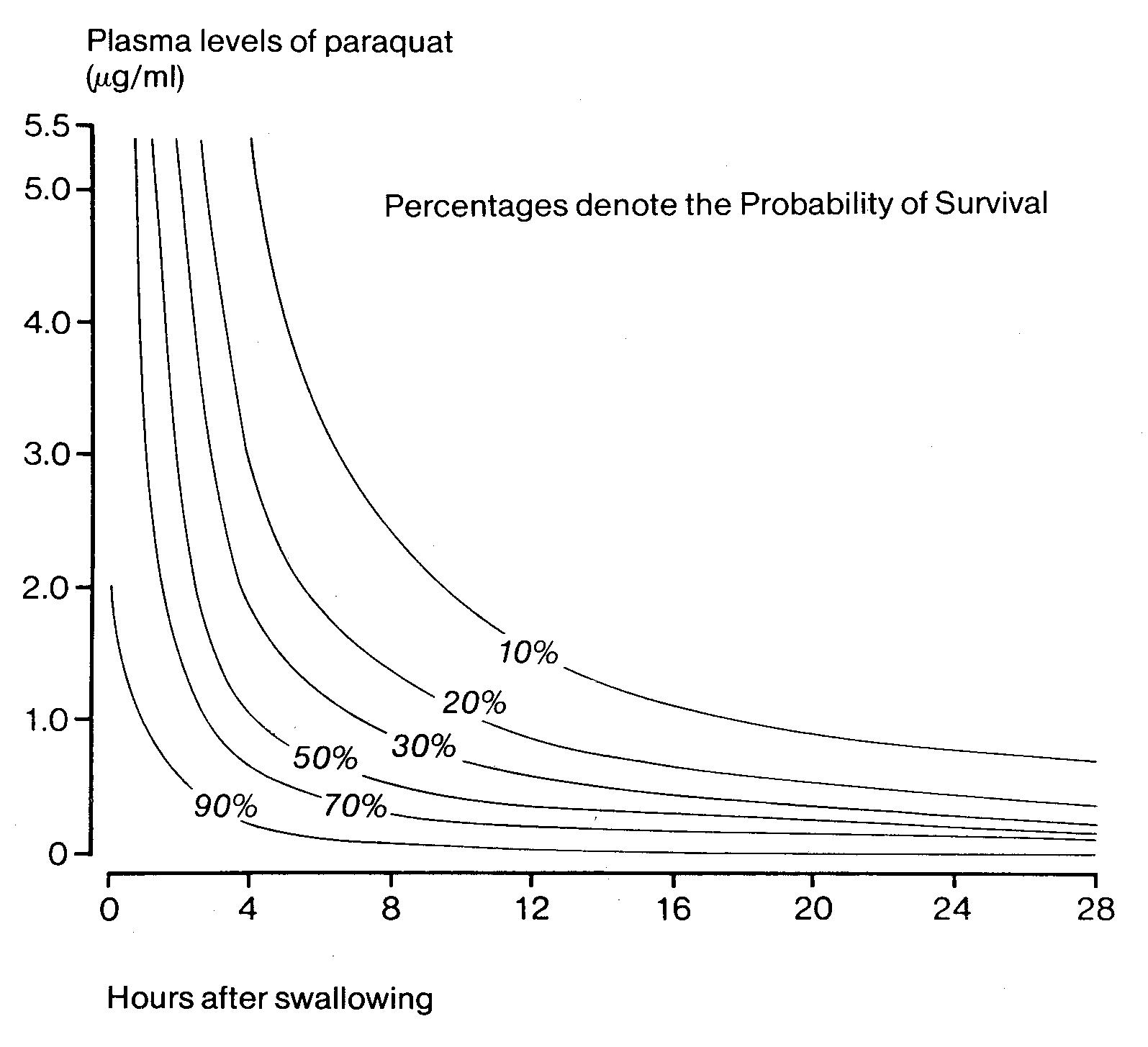
• Quantitative measurement in plasma gives a measure of severity and prognosis
(the sample must be taken at least 4 hours post-ingestion, and should be stored
hours: diarrhoea, abdominal pain, mouth and throat ulceration.
one to four days: renal failure, hepatic impairment, hypotension and
• Plasma should be analysed rather than serum, because serum paraquat
concentrations are approximately 3 fold lower than those in plasma prepared
one to two weeks: cough, haemoptysis, pleural effusion, pulmonary fibrosis
from the same blood sample. If only serum is available results should be
interpreted with caution in relation to survival curves.
Survival is possible, but in the majority of cases death occurs within 2 – 3 weeksfrom pulmonary failure.
• See section on ‘Analytical Techniques’ for details
• Fulminant: >40 – 55 mg/kg mg paraquat ion/kg body weight.
hours to days: diarrhoea, abdominal pain, renal and hepatic failure,gastrointestinal ulceration, pancreatitis, toxic myocarditis, refractoryhypotension, coma, convulsions.
Death from cardiogenic shock and multi-organ failure occurs within 1-4 days
General Supportive Measures (see flowchart)
i.v. fluids – the kidney is the major route of excretion of paraquat and renalfunction must therefore be closely monitored and optimum function
Significant paraquat ingestion suspected on history and / or
analgesics – aggressive analgesia (e.g. opiates) may be required sincepatients can have severe pain from oral, oesophageal or abdominalcorrosive injury. Control of vomiting
mouth care for ulceration and inflammation. Vomiting?
patients should be kept nil by mouth if there is a suspicion of oropharyngeal
avoidsupplemental oxygen unless significant hypoxia exists (oxygen enhances paraquat toxicity). Charcoal 100g or 2 g/kg Fullers Earth 1 litre of
supporting renal function with haemodialysis or haemofiltration may berequired
General Early Management
palliative care is paramount for those with a poor prognosis
other specific treatments could be considered depending on the clinical
context (see section on Other Potential Treatment and obtain advice from a
Paraquat Spot Test - urine or Repeat at 6 hours gastric aspirate Discharge Plasma paraquat level Supportive Management Survival probability curve (for
palliative care for those with poorprognosis
Eyes Skin
• If the product is used as recommended and normal hygiene practices are
may cause a transient stinging sensation but no damage is expected.
observed, effects on the skin are unlikely. Intact skin is an effective barrier toparaquat absorption under normal circumstances.
may cause severe inflammation of the cornea and conjunctiva which may
concentrated formulations (e.g. ‘Gramoxone 100’) may result in irritation,
loss of corneal and conjunctival epithelium and even mild iritis can occur with
blistering and potentially full thickness burns which usually develop 1 to 3
the risk of secondary infection and consequent residual corneal scarring.
corneal oedema may persist for up to 3-4 weeks with temporary blurring of
brief contact with products diluted for use may cause erythema.
nail damage, discoloration (e.g. white spots) or total loss of the nail mayoccur upon direct contact with the concentrated formulation. Normal nail re-
Treatment
• The eye should be irrigated immediately for at least fifteen minutes with water or
Systemic toxicity is rare but can occur if there is:
saline and a fluorescein stain performed.
prolonged contact e.g. not washing after being splashed with concentrate;carrying of leaking knapsack sprayers; wearing of clothes soaked in spray.
• Local antibiotics may be needed to prevent secondary infection.
Extensive scrotal or perineal contamination.
skin is broken and there is significant exposure.
• If splashed with the concentrate, patients should be reviewed after 24 hours.
large areas of skin contaminated with concentrate, even if washed.
• Referral to an ophthalmologist should be considered. Prevention and treatment
• Decontaminate as soon as possible by removing contaminated clothes and
washing skin thoroughly with soap and copious amounts of water, taking care toavoid abrasion.
• Treat any skin irritation/damage symptomatically with daily review if
contaminated with concentrate (as blistering and chemical burns may developover 1 to 3 days).
• If systemic toxicity is suspected, test urine for paraquat. There is little data for
time to peak plasma levels by skin absorption, but if the urine is negative for 24hours, systemic toxicity can probably be discounted. If the urine test is positive orif there is any doubt about potential systemic toxicity, obtain a blood level andtreat for systemic toxicity as above
Inhalation
Paraquat’s herbicidal effects were discovered in the late 1950s and the product wasfirst sold in 1962. It is today the world’s second largest selling weedkiller and isregistered and used in well over 100 countries.
• Paraquat is not volatile but all liquid Syngenta paraquat formulations contain an
unpleasant ‘stenching agent’ which may occasionally cause feelings of nausea or
It is a fast-acting contact herbicide which is rainfast shortly after application and is
rapidly deactivated on contact with soil, having no residual effects in the soil. Itsnormal use causes no adverse effects on wildlife or the environment. When properly
used it has no adverse effects on the health of spray operators.
when applied as recommended the spray droplets are too large to beinhaled into the lungs.
Its many uses in a wide variety of crops have helped to increase the productivity of
application as a fine mist may cause some irritation of the upper respiratory
agriculture in both the developed and developing world. By reducing the need for
tract but there are no reports of serious systemic toxicity from inhalation.
cultivation it has helped to prevent erosion of soil and assisted in the conservation of
Local irritation of nose and throat may occasionally cause epistaxis. Contact
soil moisture. It has facilitated the introduction of ‘no-till farming’ or direct drilling’ in
of nasal mucosa with fingers contaminated with paraquat may also cause
which time and energy-consuming soil cultivation have been eliminated. Treatment
No specific treatment is required other than symptomatic for epistaxis. There is noneed to perform a urine test as the lungs are not a major route of absorption.
Paraquat concentrates in (pulmonary) alveolar type I and II cells via an energy
dependant transport system (due to structural similarity of paraquat with naturallyoccurring polyamines taken up by alveolar cells). Paraquat ion (PQ2+)
• High concentration of paraquat once accumulated into lung or renal cells results
in redox cycling and generation of toxic reactive oxygen species (see diagram). This can overwhelm cellular defence mechanisms and lead to lung damage(acute and subchronic) and renal tubular necrosis.
• Renal failure may occur as a result of direct tubular toxicity and haemodynamic
changes. It is an early, but often reversible, feature of paraquat poisoning.
Maintenance of renal function is important to reduce plasma paraquat levels and
thereby minimise accumulation in lung cells.
After large doses multi-organ failure can lead to rapid death. At more intermediate
doses, the initial lung injury may appear to repair, but then develop into fibrosis.
This is characterised by rapid, excessive proliferation and differentiation of
fibroblasts, resulting in a loss of pulmonary architecture and interference with gasexchange. Depletion of surfactant and the inflammatory response may alsocontribute to further toxicity
O X Y G E N F R E E R A D I C A L S G L U T A T H I O N E O X I D A T I O N L I P I D F R E E R A D I C A L S
Formed by fatty acids reacting with oxygen
CELL DEATH AND MULTI-ORGAN DYSFUNCTION / FAILURE
the six patients with the lowest plasma concentration survived. Lin et al., (1999)reported results of a prospective, randomised study of pulse therapy with
cyclophosphamide (1g/day over 2 days) and methylprednisolone (1g/day over 3days) in 142 patients. Seventy-one patients died from fulminant poisoning within oneweek, and cyclophosphamide did not make any difference. In the group ofmoderately to severely poisoned patients, only 4/22 patients treated with
Enhanced elimination of paraquat
cyclophosphamide died, compared to 16/28 in the control group. Plasma paraquatconcentrations were not available, but the authors stated that there was no difference
Peritoneal dialysis or haemodialysis may be required in patients with acute renal
in severity of poisoning between the two groups based on the urine dithionite test.
failure, but they are ineffective in enhancing the elimination of paraquat from the
However, the beneficial effects of the cyclophosphamide-dexamethasone regime
have been disputed and in a prospective study Perriens et al., (1992) did not find anydifference in mortality between 14 patients who had received standard treatment and
Haemoperfusion has been postulated as a treatment for a number of years but its
the 33 patients who had received high-dose cyclophosphamide and dexamethasone.
efficacy remains controversial. While charcoal columns are very efficient at removing
A final answer regarding the usefulness of this therapy can therefore not been given
paraquat from the blood, paraquat is rapidly distributed to other tissues and re-
distributes back to the blood relatively slowly. i.e. toxic levels in tissues occur early inthe course of the poisoning.
When considering the use of haemoperfusion in paraquat poisoning, note that:
Radiotherapy has been suggested to decrease the number of fibroblasts (veryradiosensitive) in the lung, and hence decrease fibrosis. However, there is no
1. Patients who have ingested borderline lethal quantities of paraquat, or have
conclusive evidence that it improves survival.
survival probabilities between 20 and 70 percent, and present within a few hours (probably < 6-10 hours) post ingestion may benefit from haemoperfusion (since the paraquat may not have distributed to the tissues / lungs in toxic quantities
and even small differences in the paraquat level may affect survival probability).
Although lung transplantation has been tried in several cases, success has been
2. Patients who have taken many times the lethal dose of paraquat, or have very
reported in only one (Walder et al., 1997). This was performed 5 weeks after the
poor prognosis on survival probability curves, are not helped by haemoperfusion
initial presentation (the patient was supported with mechanical ventilation during this
time until a donor was found). Supportive treatment also consisted of haemodialysisuntil no paraquat was detected in the plasma or dialysate.
3. The use of ‘continuous’ haemoperfusion is probably not life-saving but may
prolong survival. This may allow the use of other treatment modalities to be
Other agents
considered (e.g. lung transplantation, see below) (Suzuki et al., 1993).
A wide range of therapeutic substances have been studied experimentally. Some
Prevention and treatment of pulmonary fibrosis
have been used in humans, but most of the published work is based on single or asmall number of cases (for a detailed review see Lock and Wilks, 2001).
Patients with moderate intoxication who do not die from early, multiorgan failure oftendevelop progressive pulmonary fibrosis. This leads to respiratory failure and death
Agents which have been used clinically include:
within a few weeks. Several treatment modalities have attempted to prevent this.
• antioxidants (vitamins C and E) and superoxide dismutase to reduce free radical
Cyclophosphamide and steroid therapy
• N-acetyl cysteine to increase intracellular glutathione
• desferrioxamine to chelate iron which acts as catalyst in the production of
Several studies have looked at the use of cyclophosphamide and steroid therapy.
Addo and Poon-King (1986) claimed a 72% survival rate in 72 patients treated with
• propranolol to block paraquat uptake into the lung
cyclophosphamide (5 mg/kg/day to a maximum total of 4 g) and dexamethasone (8
• inhaled nitric oxide to improve pulmonary gas exchange
mg eight-hourly over two weeks). However, the plasma paraquat data of 25 patientsshowed that 7 survivors had no measurable paraquat levels, and of the other 18 only
Plasma can block the cartridges so if possible it should be filtered, for example
through a 0.45µm syringe filter ( PVDF or nitrocellulose ) before performing the test. Serum does not require this pre-treatment unless it is cloudy. • Mix approximately 1g portions of sodium bicarbonate and sodium dithionite with
1. Qualitative confirmation of diagnosis
• Urine is made alkaline by addition of approximately 0.5g of sodium bicarbonate
• Transfer 2 mL plasma, serum or alkalinised urine to a 1 mL/100mg silica SPE
cartridge, and allow the sample to percolate through into the bed (the preferred
Urine or gastric aspirate can be tested for paraquat using the method
cartridge is Bakerbond Cat No 7086-01, an alternative is Varian Bond-Elut
based on reduction of paraquat cation to a blue radical ion in the presence
• Using a syringe fitted on to the top of the cartridge with an adapter, apply gentle
pressure to force the rest of the sample through the cartridge.
Add alkali, such as sodium hydroxide, to 10 ml or urine or gastric aspirate
• Wash the cartridge with an equal volume of water, keeping the flow rate low.
until the pH is above 9 (approximately half to one teaspoon of sodium
• Add approximately 0.2 mL of the dithionite solution to the cartridge and apply
bicarbonate can be used as an alternative).
very slight pressure to ensure that the liquid penetrates to just below the top frit. Do not allow the cartridge to dry out
Add a spatula blade full of sodium dithionite to the alkaline urine or gastric
• A blue band immediately below the top frit of the cartridge indicates the presence
of paraquat and confirms the diagnosis. NB. Once opened and exposed to air/moisture sodium dithionite can
• This test will detect paraquat down to a level of around 0.1 µg/ml with a 2 mL
deteriorate on storage so users should ensure that the reagent works
sample. Ideally a positive control should be carried out, at a level of around 0.5
effectively preferably by testing a sample known to contain paraquat.Sodium dithionite packed in foil sachets supplied in test kits has ashelf-life of at least 10 years if undamaged.2. Quantitative determination of paraquat
View the tube from above against a white background. A blue or greencolour in the solution denotes the presence of paraquat and confirms thediagnosis. In the presence of high paraquat concentrations, the solution
Quantitative measurement in plasma gives a measure of severity and prognosis
may turn black, and the test should be repeated with a diluted sample.
(the sample must be taken at least four hours post-ingestion, and should becentrifuged and stored in plastic, not glass tubes.)
This method can detect concentrations of paraquat in urine down to 2
2.1. SPECTROPHOTOMETRY FOLLOWING SOLID-PHASE EXTRACTION AND
g/ml and may be made semi-quantitative if a range of standards are
prepared in control urine samples. (Widdop 1976; Berry and Grove, 1971).
• Plasma or serum samples are first filtered as described in section 1.2. Bond-Elut
cyanopropyl cartridges (100mg 1 mL reservoir, Varian) are pre-conditioned
successively with two column volumes of methanol, 0.1M HCl and 0.1Mammonia solution. The cartridges are fitted with 15 mL reservoirs and the patient
Urine, serum or plasma can be tested for paraquat using a method based on in situ
plasma, serum, blank or spiked plasma ( 5 mL) is applied and drawn through by
reduction on a solid phase extraction cartridge ( Woollen and Mahler 1987).
attaching the cartridges to a vacuum manifold until the cartridges are dry. The
A more sensitive version of this test using the reagents provided in the test kits is
cartridges are rinsed with 1 mL 0.1M ammonia until they are dry and then
paraquat is eluted with 0.8 mL 0.1M HCl into a test tube. Concentrated ammonia(0.025 mL) and sodium dithionite (0.1 mL 0.23M in 4M NaOH) are added. Aftervortexing the solutions are poured into disposable semi-microcuvettes (1 mL) andthe absorbance scanned from 490 to 385 nm. The absorbance difference (A395-
A460) is used to determine the paraquat concentration.
• A standard curve is prepared in the range 0.05 - 1µg/mL paraquat ion. Higher
concentrations in unknown samples may be determined by taking a smalleramount of plasma sample. The lower limit of quantitation of the assay is 0.045
• The method is also applicable to urine which must be alkalinised (0.025 mL
concentrated ammonia to 5 mL urine) and centrifuged prior to addition to thecartridge.
• Paraquat can be measured in plasma or urine down to 0.001µg/mL by
fluorescence HPLC after conversion to the dipyridone derivative (Blake, et al2002). 3. Advice on paraquat analysis
Syngenta CTL can provide advice on analysis of paraquat in biological samples viathe e-mail address [email protected]
Addo, E. and Poon-King, T. (1986). Leucocyte suppression in treatment of 72 patients with paraquat poisoning. TheLancet1, 1117-1120
Blake D.K., Gallagher R.T. and Woollen B.H. (2002). Improved methods for the analysis of paraquat in biological fluids. Chromatographia 55, s183-185
Berry, D.J. and Grove, J. (1971). The determination of paraquat in urine. Clinica Chimica Acta 34, 5-11
Hampson, E. C., and Pond, S. M. (1988). Failure of hemoperfusion and hemodialysis to prevent death in paraquat poisoning - a retrospective review of 42 patients. Med. Toxicol. Adverse Drug Experience3, 64-71.
Hart, T.B. et al., (1984). A New Statistical Approach to the Prognostic Significance of Plasma Paraquat Concentrations. The Lancet, 2, 1222-3
Lin, J.L., Leu, M.L., Liu, Y.C., and Chen, G.H. (1999) A prospective clinical trial ofpulse
therapy with glucocorticoid and cyclophosphamide in moderate to severe
paraquat-poisoned patients. Am. J Resp. Crit. Care Med. 159, 357-360.
Lock, E.A., Wilks, M.F. (2001) Paraquat. In: Krieger, R.I. (ed.), Handbook ofPesticide Toxicology (2.ed.), pp. 1559 – 1603, Academic Press, San Diego.
Perriens, J.H. et al., (1992). High-dose cyclophosphamide and dexamethasone in paraquat poisoning: a prospective study. Human & Experimental Toxicology, 11, 129-134
Smith, N.B., Mathialagen, S. and Brooks, K.E. (1993). Simple and Sensitive Solid- Phase Extraction of Paraquat from Plasma Using Cyanopropyl Columns. J Analytical Toxicol17, 143-145
Suzuki, K. et al. (1993), Effect of Aggressive Haemoperfusion on the Clinical Course of
Patients with Paraquat Poisoning, Human & Experimental Toxicology12, 323-327
Walder, B. et al. (1997). Successful single lung transplantation after paraquat intoxication, Transplantation, 64, 789-791
Widdop, B. (1976). Detection of paraquat in urine. Br. Med. J. Part IV, 1135
Woollen, B.H. and Mahler, J.D. (1987). An improved spot test for the detection of paraquat and diquat in biological samples , Clin Chim Acta167, 225-229
Amoxycillin Market Research Report Overseas Market of Amoxicillin Based on Official Trade Data Contents Introduction Market Characteristics Market Segments a. Generics vs. Branded b. Dosage Forms Largest Markets Brand Tracking Country Analysis a. South Africa b. Nigeria c. Myanmar d. Sri Lanka e. Netherlands f. Yemen g. Madagascar h. Uganda i. UAE 7.
The American Journal of Medicine (2005) 118, 612– 617 CLINICAL RESEARCH STUDY Incidence of intracranial hemorrhage in patients with atrial fibrillation who are prone to fall Brian F. Gage, MD, MSc,a Elena Birman–Deych, MS,a Roger Kerzner, MD,b Martha J. Radford, MD,c David S. Nilasena, MD, MSPH, MS,d Michael W. Rich, MDb aDivision of General Medical Sciences, Washington University
 Addo, E. and Poon-King, T. (1986). Leucocyte suppression in treatment of 72
Addo, E. and Poon-King, T. (1986). Leucocyte suppression in treatment of 72