TOXBASE® an NPIS service commissioned by the Users Update: Oct 2011 www.TOXBASE.org is the online clinical toxicology database of the UK National Poisons Information Service
You have received this newsletter because your practice or unit is a registered TOXBASE® user
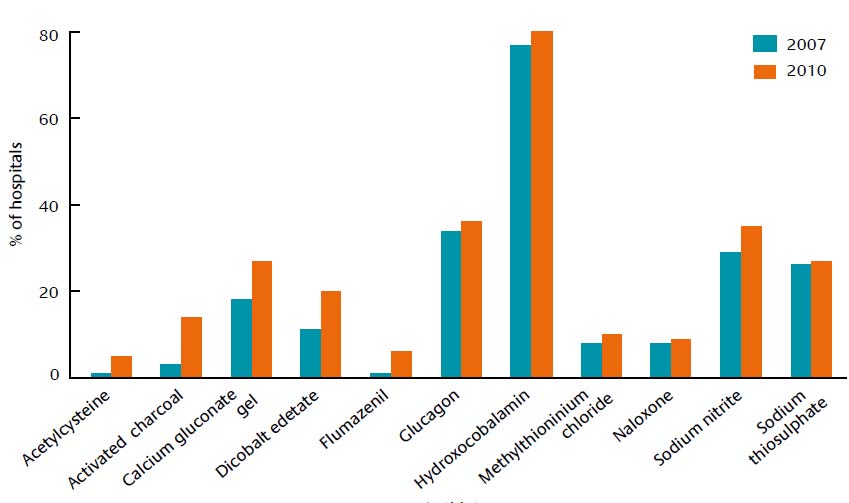
Antidote availability in UK hospitals Joint guidelines for antidote stocking by Emergency Departments in the UK were issued by the College of Emergency Medicine and NPIS in 2008. To assess compliance with this guideline a national audit was undertaken. A short questionnaire was sent to every acute hospital in the UK. 196 were completed and returned (87.5% response rate). The results showed that most commonly used antidotes are available immediately or within one hour in most acute hospitals in the UK. However a small percentage of hospitals did not hold immediately available stocks of naloxone. It is recommended that cyanide antidotes should be available for immediate use - most hospitals held at least one of the four cyanide antidotes (usually dicobalt ededate) but 9 (5%) held none. Calcium gluconate gel, which is an antidote for hydrogen fluoride exposure, is also recommended to be available for immediate use - this was not stocked by 25% of acute hospitals. Proportion of hospitals not holding recommended stocks of antidotes that are recommended to be immediately available
Of antidotes recommended to be available within one hour, pralidoxime (which should be held at selected holding centres and/or in DoH pods for major incidents) was held in 33% of acute hospitals. Viper venom antiserum and cyproheptadine and were only stocked by about 50% of acute hospitals. It is recommended that antidotes for toxic alcohol and glycol poisoning should be available for use within one hour in all acute hospitals. Most hospitals held ethanol for intravenous use. Only a minority stocked fomepizole, although it is the antidote of choice when the diagnosis is established in view of the difficulty in maintaining and monitoring ethanol infusions. It is also the preferred antidote in patients who have (or who are at risk of) depression of conscious level, those who have hepatic disease, those who have taken disulfiram or metronidazole, and in children and pregnant women. 30 (15%) acute hospitals did not have any antidote available locally for treatment of toxic alcohol and glycol poisoning, even though poisoning with these agents is not uncommon in the UK. Indications for, and appropriate methods of use of, antidotes and other medications in poisoning can be found on TOXBASE®. Information on antidotes and antivenoms, including lists of locations, can also be found on TOXBASE® - General Info tab / Antidotes and antivenoms. Further advice can be obtained from the NPIS by telephone via 0844 892 0111 (in Ireland NPIC 01 809 2566).
TOXBASE® is administered from NPIS Edinburgh, Royal Infirmary of Edinburgh tel 0131 242 1381/1383 - fax 0131 242 1387 - [email protected] 1
Update in Medical Toxicology During August & September 2011 New TOXBASE® monographs included:
University Hospital Llandough - is designed
for those interested in medical toxicology
including nurses, specialist registrars and
other physicians (particularly those working in
accident and emergency medicine) who wish
to gain expertise in the practical management
health care professionals working in the field
Updated TOXBASE® monographs included: NPIS annual report now available
includes the TOXBASE® annual report, is now
General Info tab / Newsletters and publications or from HPA http://www.hpa.org.uk/Publications/Chemical sPoisons/NationalPoisonsInformationService AnnualReports Recently published
Djokanovic N, Klieger-Grossmann C, Pupco A,
Koren G. Safety of infliximab use during pregnancy.
Hill SL, Thomas SHL. Clinical toxicology of newer
recreational drugs. Clin Toxicol 2011; 49: 705-19.
We wish to thank all our users for their assistance in providing information that
Simkin S, Hawton K, Kapur N, Gunnell D. What can
can be fed back into NPIS datasets and
be done to reduce mortality from paracetamol
improve the information NPIS provides.
overdoses? A patient interview study. QJM 2011; online early: doi: 10.1093/qjmed/hcr135
If you are no longer the TOXBASE® contact
person for your practice or unit we would be
Cassidy N, Duggan E, Williams DJP, Tracey JA.
The epidemiology and type of medication errors
reported to the National Poisons Information Centre
If you do not wish to receive this newsletter in
of Ireland. Clin Toxicol 2011; 49: 485-91.
future please send an e-mail with the word
TOXBASE® is administered from NPIS Edinburgh, Royal Infirmary of Edinburgh tel 0131 242 1381/1383 - fax 0131 242 1387 - 2
Clinica e terapia dei disturbi da uso di sostanze. Stimolanti del Sistema Nervoso Centrale Introduzione Gli stimolanti del SNC (S-SNC) agiscono da potenti simpaticomimetici periferici edesplicano, in vari gradi, effetti stimolanti sul piano psicomotorio. Gli stimolanti di piùcomune abuso sono la cocaina e le amfetamine. Anche se per tali farmaci esiste unlimitato uso terapeutico (le amf
C2 Hard™ DESCRIPTION C2 Hard™ is the advanced sealer, hardener and densifier for concrete surfaces and a much more effective alternative to conventional sodium or potassium silicate hardeners. This patented lithium silicate treatment deeply penetrates and reacts with the concrete to produce insoluble calcium silicate hydrate within the concrete pores. Conventional hardeners deposit high




 TOXBASE® an NPIS service commissioned by the
TOXBASE® an NPIS service commissioned by the 



 Update in Medical Toxicology
Update in Medical Toxicology