Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Doi:10.1016/j.pnpbp.2006.06.025
Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx – xxx
Psychological traits and platelet monoamine oxidase activity in eating
disorder patients: Their relationship and stability
Iris Podar a,⁎, Maiken Jaanisk a,b, Jüri Allik a, Jaanus Harro a,b
a Department of Psychology, University of Tartu, Tiigi 78, Tartu 50410, Estonia
b The Estonian Centre of Behavioral and Health Sciences, University of Tartu, Tartu 50410, Estonia
Self-reported behavior and attitudes towards eating [Eating Disorder Invetory-2; Garner DM (1991). Eating Disorder Inventory-2: Professional
Manual. Odessa, Fl.: Psychological Assessment Resources; Estonian version Podar I, Hannus A, Allik J (1999). Personality and AffectivityCharacteristics Associated With Eating Disorders: a Comparison of Eating Disordered, Weight-Preoccupied, and Normal Samples. J Pers Assess;73(1), 133–147] and the activity of platelet monoamine oxidase (MAO) was studied in 11 patients with anorexia nervosa (AN), 43 patients withbulimia nervosa (BN) and a healthy control group (n = 138). Nineteen patients filled in the EDI-2 questionnaire and donated blood samples threetimes with three month intervals in order to determine platelet MAO activity. Eating disordered (ED) patients scored higher on all EDI-2 subscalesand had lower MAO activity compared to the control group. They also scored higher than the control group on the Neuroticism domain but loweron the Extraversion, Openness, and Conscientiousness domains of the NEO-PI-R questionnaire. The average stability of MAO on differentoccasions (r = .56) was slightly smaller than the stability of the EDI-2 scores (r = .70). The lack of correlations between personality dispositions andMAO activity indicates that they have independent influence on eating disorders. A possible relationship between neurochemical mechanisms andpsychological symptoms of eating disordered behavior is discussed. 2006 Elsevier Inc. All rights reserved.
Keywords: Anorexia nervosa; Bulimia; Eating disorders; EDI-2; NEO-PI-R; Platelet MAO; Stability
syndromes are far more common among females than males andthey have become more common among younger females
Since eating disordered behavior is more prevalent in
during the latter half of the twentieth century it is believed that
industrialized and Western societies, culture has been identified
they are reflecting current cultural beauty ideals for women
as one of the major etiological factors leading to the
development of anorexia nervosa (AN) and bulimia nervosa
eating disorders have socio-cultural (e.g., family influences and
cultural pressures for thinness) risk factors there are also psycho-logical (e.g., personality dispositions)
Abbreviations: 5-HT, 5-hydroxytryptamine; A, agreeableness; A, asceti-
cism; AN, anorexia nervosa; B, bulimia; BD, body dissatisfaction; BMI, body
involved in the development of eating disordered behavior
mass index; BN, bulimia nervosa; C, conscientiousness; DT, drive for thinness;
E, extraversion; EDI-2, Eating Disorder Inventory 2; F 50.0, anorexia nervosa
Like many other obsessive compulsive behaviors, eating
(International Classification of Diseases-10); F 50.2, bulimia nervosa (Interna-
disorders demonstrate a high degree of stability over time (
tional Classification of Diseases-10); I, ineffectiveness; IA, interoceptiveawareness; ID, interpersonal distrust; IR, impulse regulation; MAO, monoamine
oxidase; MAO-B, monoamine oxidase B isoenzyme; MF, maturity fears; N,
neuroticism; NEO-PI-R, Revised NEO Personality Inventory; O, openness to
is associated with a 9-fold increase in risk for late adolescent
experience; P, perfectionism; SI, social insecurity.
bulimia nervosa and a 20-fold increase in risk for adult bulimia
nervosa. Late adolescent bulimia nervosa is associated with a 35-
(M. Jaanisk), (J. Allik), (J. Harro).
fold increase in risk for adult bulimia nervosa. Presence of eating
0278-5846/$ - see front matter 2006 Elsevier Inc. All rights reserved.
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
problems in early childhood or an eating disorder in adolescence
confers a strong risk for an eating disorder over a 17-year interval
The role of serotonin dysregulation in the devel-
Disorder Inventory (EDI-2; administered 10 years
opment of eating disorders is also demonstrated by a significant
improvement of AN and BN patients who have been treated with
the serotonin reuptake inhibitor citalopram
that disturbed eating attitudes decline with age, the mean scores
on eating disorder attitude scales tended to increase with age
Although both, personality dispositions and serotonin sys-
(). Therefore it is not surprising that different
tem dysfunction, contribute to the eating disorders, there are
instruments like Eating Disorder Inventory (EDI,
relatively few studies in which these two groups of factors are
also demonstrate a good test–retest stability. For example, in a
jointly studied in the clinical and normal samples. Existing data,
non-clinical sample EDI demonstrated a substantial stability
however, demonstrate that there may be a covariation between
over a 1 year period ). Although developed
personality traits and neurochemical activity in the brain. For
for adults, EDI-2 scales demonstrated considerable test–retest
stability also in a sample of adolescents over a 3 year period
tween personality traits and 5-HT indices in bulimic patients.
(An acceptable test–retest stability was
These findings suggest a multidimensional model of eating
also observed in samples of eating disordered patients
disorders according to which biological and personality dispo-
sitions jointly interact in the development of eating disorders
“drive for thinness” were found to change significantly over
of attempts to study in parallel the influence of personality
Although the stability of eating disordered behaviors and
dispositions and the activity of the serotonin system on the
attitudes suggests the enduring role of personality dispositions in
eating behavior and attitudes. Another novelty of this study is a
the development of eating disorders, it is not entirely clear what
longitudinal observation of self-reported behavior and attitudes
combination of personality traits contribute as a risk factor (
towards eating in parallel with MAO activity three times with
The best documented link exists betweenneuroticism and eating disorders
). However, the role of other personality dispositions in theetiology of eating disorders is less clear. Increasing evidence
Altogether one hundred and ninety two subjects from two
indicates that normal and abnormal personality can be treated
different groups participated in this study.
within a single hierarchical structure in which the level of fivefactors is the most comprehensive Unfor-
tunately, the number of studies of eating disorders in the frame-
Fifty four patients with eating disorders who were consec-
work of the Big Five personality factors is limited
utively admitted to the Psychiatric Clinic of Tartu University
Hospitals between March 2000 and March 2003 took part in this
study, among them 11 cases met the criteria for anorexia nervosa
). Nevertheless, findings seem to suggest that
(F 50.0) and 43 cases for bulimia nervosa (F 50.2). The patients
eating disorder symptomatology is correlated with high neurot-
were diagnosed based on the criteria of the Classification of
icism and openness to experience and low conscientiousness and
Mental and Behavioural Disorders (International Classification
of Diseases-10; World Health Organization, 1992). The patients
were diagnosed by experienced psychiatrists. Twenty one
complete agreement between different studies. For example,
patients were diagnosed having co-morbidity symptoms, most
frequently depression (F 32) in 15 cases. However, only in
domly selected from the general population a high level of open-
2 cases depressive episodes were severe (F 32.2). Two patients
ness, not closeness, was significantly associated with self-
were diagnosed with recurrent depressive disorder (F 33.1). In
reported lifetime history of eating disorder.
2 cases, both bulimics, a harmful use or dependence on alcohol
Besides phenotypical personality traits, that can be conceptu-
was recorded (F 10). In one case social phobias (F 40.1) were
alized as biologically rooted endogenous dispositions (
reported. Forty patients (74%) received antidepressant treat-
the disturbances in the underlying neuro-
ment. In most cases (30 patients) Fluoxetin (20 mg/day) or some
chemical systems may be another risk factor for eating disorders.
other antidepressants like Paroxetin or Citalopram (9 cases) were
In particular, patients with eating disorders exhibit serotonin (5-
prescribed from one to twelve months. In 1 case anxiolytic
Xanax was prescribed. All patients received at least once psy-
). Several studies have confirmed that patients with
chiatric consultation concerning eating disorders, dieting, and
AN or BN demonstrate reduced activity of platelet monoamine
nutrition and were encouraged to start treatment. Three patients
oxidase (MAO) activity which is a reliable peripheral indicator of
attended sessions of cognitive-behavioral therapy (at least 10
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
sessions). All participants were females aged 16–37 years
activity was measured as previously described (
(Mean = 20.1; S.D. = 4.5) and their mean body mass index (BMI;
) and expressed as nanomoles of β-phenylethylamine
the body weight in kilograms divided by the squared height in
oxidized per 1010 platelets/min. On the first time all the patients
meters) was 19.77 (S.D. = 2.8). Eleven patients were smokers.
participating in the research were tested for MAO activity(n = 54), blood samples from 34 and 26 patients, respectively,
were available at follow-up three months or six months later.
The control group (n = 138) was also entirely comprised of
females aged 16–37 years (Mean = 20.14; S.D. = 3.33) and their
BMI was 20.47 (S.D. = 2.45). The control group was selected fromthe students of Tartu University and other schools, employees of
Patients who volunteered to participate were asked to fill in
the Psychiatric Clinic and others, who volunteered to participate in
the EDI-2 Estonian version and have their blood tested for the
the research project. The control group was selected to match the
activity of monoamine oxidase three times with an interval of
eating disordered patients by their sex, age, and education.
three months. Forty eight filled EDI-2 questionnaires were
Thirteen participants from the control group were smokers.
returned on the first time, 26 on the second and 19 on the third. Nineteen patients returned the filled questionnaires and had
MAO activity tested all three times.
The Estonian version (of the Eating Disorder
Inventory- 2 (EDI-2; ) consists of 91 items and 11
Internal consistency of the EDI-2, both in clinical and control
subscales measuring psychological characteristics and behaviors
samples, was similar and in the range of reliabilities reported in
associated with eating disorders. The items are evaluated on a 6-
the EDI-2 manual ). In the control group (n = 138)
point scale (from “never” to “always”) which for the analysis is
alpha was .84 and in the patient group (n = 54) alpha was .88.
transformed into a 4-point scale. Like its predecessor, EDI-2
shows the mean values on EDI-2 scales for the three
consists of 8 primary scales: DT — Drive for Thinness, B —
categories of participants: AN and BN patients and the control
Bulimia, BD — Body Dissatisfaction, I — Ineffectiveness, P —
group. When treated as a single category, ED patients scored
Perfectionism, ID — Interpersonal Distrust, IA — Interoceptive
significantly higher on all EDI-2 scales compared to the control
Awareness, and MF — Maturity Fears. In the second revision
group (F values in ANOVA varied from F(1,182) = 8.08 to 79.90
EDI-2 consisted of 3 additional scales were developed: A —
for the Perfectionism and Ineffectiveness subscales respectively,
Asceticism, IR — Impulse Regulation, and SI — Social
p always higher than .003). In comparison with each other, ano-
Insecurity. The first 3 subscales are concerning eating, weight
rexia and bulimia patients differed significantly only on the B
and body shape (DT, B, BD), and eight subscales concerning
subscale (F(1,44) = 11.64, p b .001) where bulimia patients scored
psychological traits thought to be clinically relevant to eatingdisorders (I, P, ID, IA, MF, A, IR, SI). The diagnostic validity ofthe Estonian EDI-2 has been previously demonstrated
NEO Personality Inventory (NEO-PI-R) is a 240-item measureof the Five Factor Model of personality (It contains 30 8-item facet scales, six for each of the fivebasic personality factors, Neuroticism (N), Extraversion (E),Openness to Experience (O), Agreeableness (A), and Consci-entiousness (C). The factors can be estimated by domain scores,which sum the relevant six facets. The original NEO-PI-R wastranslated and adapted into Estonian with all psychometricallysignificant parameters similar to the original instrument ). In the previous report of Estonian EDI-2() an older version of the NEO-PI was used(Estonian NEO-PI-R data have repeatedlybeen reported in different publications and demonstrate anacceptable validity ).
Fig. 1. The mean scores of EDI-2 subscales for controls (n = 138), anorexiapatients (AN) (n = 11) and bulimia patients (BN) (n = 37). EDI-2 subscales: DT =Drive for Thinness; B = Bulimia; BD = Body Dissatisfaction; IE =
Ineffectiveness; P = Perfectionism; ID = Interpersonal Distrust; IA =
One hundred and six individuals from the control group gave
Interoceptive Awareness; MF = Maturity Fears; A = Asceticism; IR = Impulse
blood samples for determining their MAO-B activity. MAO
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
higher than anorexia patients. The difference on the BD subscale
EDI-2 stability proved to be statistically significant on all the
was only marginally significant (F(1,45) = 4.08; p = .049).
subscales as well as in the total score. The average stability of
The average profile of ED patients was very similar to what
MAO on different occasions (r = .56) was slightly smaller than the
was obtained in other countries. When the correlations were
stability of self-reported eating disorders (r = .70).
computed between the EDI-2 subscale profile obtained in thisstudy and profiles of ED patients reported in the literature, they
were typically in the range from .90 to .98 compared with Canada(Germany Italy
The results of this study clearly indicate that self-reported
behaviors and attitudes distinguish clinical samples from a
healthy control group. Both AN and BN patients scored signi-
When ED patients completed EDI-2 the second and the third
ficantly higher than normal individuals on all 11 EDI-2 sub-
time after three months and six months, respectively, only Ma-
scales. The obtained profiles of eating disordered patients are
turity Fears had decreased significantly, F(2,36) = 5.02. These
very similar to those that were obtained previously in Estonian
changes were not related to the treatment outcome. The same
samples (and various other countries such as
tendency of decrease can be seen in B, BD, IE, ID, IA and IR
Japan, Sweden and Italy. This seems to indicate that symptoms
subscales as well as the EDI-2 total score, but the difference did
and behaviors characterizing ED are rather universal and tran-
not reach a level of significance. These results are both quali-
scend from one culture to another. Although EDI-2 differenti-
tatively and quantitatively similar to previous Estonian data
ated ED samples from norm rather well, it was rather insensitive
to discriminate AN patients from BN patients. Like in previous
As expected, ED patients scored higher than the control
group on the Neuroticism domain [F(1,153) = 42.8, p b .0001]
subscale the BN group did not score higher than the AN group
but lower on the Extraversion [F(1,152) = 14.7, p = .0002],
Openness [F(1,153) = 6.27, p = .013], and Conscientiousness
The current study supports previous studies that have revealed a
[F(1,151) = 9.57, p = .002] domains.
considerable personality disposition towards ED. As expected,
In the patient group, the activity of MAO was slightly lower
neuroticism was the strongest predictor of ED. Many previous
9.76 (n = 54, S.D. = 2.91) than in the control group 10.79 (n = 106,
studies have demonstrated that individuals who are not able to
SD = 3.28). ANOVA revealed that this difference was marginally
control their emotional reactions are more inclined towards ED
significant F(1,158) = 3.76, p = 0.054. There was a statistically
significant correlation between the activity of MAO and two EDI
subscales, DT (r = −.169, p = .036) and B (r = −.190, p = .018).
). Besides neuroticism, other personality traits also
These correlations, however, were reduced and became insignif-
join a cluster of traits that is typical to ED patients characterized
icant when the division into the patient and control group was
besides neurotic tendencies by high introversion, closeness to
taken into account. When controlled for smoking correlations
experience, and low conscientiousness. It is understandable that
between the activity of MAO and all EDI subscales became
individuals who have not learned to manage their desires (low
conscientiousness), who tend to be conventional in their behavior
The correlations or stability in time of test–retest on EDI-2
(closeness), and who are more shy (introversion) are more prone to
subscale scores in eating disordered patients are shown in
developing eating problems. It is an open question whether lowagreeableness is also an etiological risk factor for the developmentof ED or not (It seems, however, that AN
patients have somewhat higher scores than BN patients on the
Test–retest correlations of EDI-2 subscales and MAO in eating disordered
Like many previous studies, results of this study indicated
that self-reported symptoms and problems are very stable in
time despite psychological and pharmacological intervention.
The average test–retest correlation of the EDI-2 total scores was
.70 which is surprisingly higher than the MAO test–retest
correlation (r = .56). It is also remarkable that the six-month
stability indices were not significantly lower than the three-
Platelet MAO activity tended to be lower among the patients,
in line with previous findings that eating disordered patients
have described a considerably larger difference in platelet MAO
activity between patients and healthy controls. Platelet MAOactivity is considered to be individually highly stable, but indeed
Note: All correlations are significant at least p b .05. T
the second, and the third time of testing.
the studies on which this assumption is based have included
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
relatively small number of subjects. In a recent longitudinal
Cassin SE, Von Ranson KM. Personality and eating disorders: a decade in
study we have found in a sample of three hundred twenty healthy
review. Clin Psychol Rev 2005;25(7):895–916.
Claes L, Vandereycken W, Vertommen H. Personality traits in eating-disordered
participants that platelet MAO activity is stable in the large
patients with and without self-injurious behaviors. J Pers Disord 2004;18
majority of subjects, but in a significant minority considerable
changes occur in either direction, the test–retest correlation
Costa Jr PT, McCrae RR. Revised NEO Personality Inventory (NEO PI-R) and
being 0.56 (). The present study demonstrates
NEO Five-Factor Inventory (NEO-FFI) professional manual. Odessa, Fl.:
that there is a weak correlation between the central psychological
Psychological Assessment Resources; 1992.
Crowther JH, Lilly RS, Crawford PA, Shepherd KL. The stability of the eating
symptoms of eating disorders and platelet MAO activity, but
disorder inventory. Int J Eat Disord 1992;12(1):97-101.
there is no clear-cut association of any of the items of EDI-2 with
Davis C, Claridge G, Cerullo D. Personality factors and weight preoccupation: a
platelet MAO activity. The lack of correlations between
continuum approach to the association between eating disorders and
personality dispositions and the MAO activity indicates that
personality disorders. J Psychiatr Res 1997;31(4):467–80.
they have independent influence on eating disorders. A specific
Diaz-Marsa M, Carrasco JL, Hollander E, Cesar J, Saiz-Ruiz J. Decreased
platelet monoamine oxidase activity in female anorexia nervosa. Acta
linkage with some of the items could theoretically have been
Psychiatr Scand 2000a;101(3):226–30.
expected, as both low and high platelet MAO activity have been
Diaz-Marsa M, Carrasco JL, Saiz J. A study of temperament and personality in
associated with psychological deviations, the former with
anorexia and bulimia nervosa. J Personal Disord 2000b;14(4):352–9.
measures of impulsivity and the latter with anxiety symptoms
Espelage DL, Mazzeo SE, Aggen SH, Quittner AL, Sherman R, Thompson R.
(Nevertheless, it is possible that either does
Examining the construct validity of the eating disorder inventory. PsycholAssess 2003;15(1):71–80.
EDI-2 not define these psychological dimensions which are
Evenden JL. Varieties of impulsivity. Psychopharmacology 1999;146:348–61.
based on the neurochemical mechanisms reflected by platelet
Fairburn CG, Harrison PJ. Eating disorders. Lancet 2003;361(9355):407–16.
MAO activity, or, alternatively, that specific psychological
Fassino S, Abbate-Daga G, Piero A, Leombruni P, Rovera GG. Dropout from
symptoms of eating disorders are associated with platelet MAO
brief psychotherapy within a combination treatment in bulimia nervosa: role
activity in a non-linear manner. Such a relationship was recently
of personality and anger. Psychother Psychosom 2003;72(4):203–10.
Fetissov SO, Harro J, Jaanisk M, Järv A, Podar I, Allik J, et al. Autoantibodies
revealed in a longitudinal population-based study which
Against Neuropeptides are Associated with Psychological Traits in Eating
suggested that both low and high platelet MAO activity predict
Disorders. Proc Natl Acad Sci U S A 2005;102(41):14865–70.
regular smoking in adolescents, the risk factor being deviation
Garner DM. Eating Disorder Inventory-2: professional manual. Odessa, Fl.:
from the population average and this non-
Psychological Assessment Resources; 1991.
linear relationship may correspond to the complex role that
Garner DM, Olmsted MP, Polivy J. Eating Disorder Inventory. Psychopharma-
serotonin and its receptor subtypes play mediating the different
Ghaderi A, Scott B. The Big Five and eating disorders: a prospective study in the
facets of impulsive behaviour (). For detecting
general population. Eur J Pers 2000;14(4):311–23.
such associations, however, the sample in this study is not
Hallman J, Sakurai E, Oreland L. Blood-platelet monoamine-oxidase activity,
suitable by its size and composition.
serotonin uptake and release rates in anorexia and bulimia patients and inhealthy controls. Acta Psychiatr Scand 1990;81(1):73–7.
Harro M, Eensoo D, Kiive E, Merenäkk L, Alep J, Oreland L, et al. Platelet
monoamine oxidase in healthy 9- and 15-years old children: the effect ofgender, smoking and puberty. Prog Neuropsychopharmacol Biol Psychiatry
This study was supported by the Estonian Science Founda-
tion (grants 5450 and 5677) and the Estonian Ministry of
Harro J, Fischer K, Vansteelandt S, Harro M. Both low and high activities of
Education and Science (grants 2585 and 2643). We are grateful
platelet monoamine oxidase increase the probability of becoming a smoker. Eur Neuropsychopharmacol 2004;14(1):65–9.
to Dr. Anu Järv and Prof. Veiko Vasar for their professional help
Heatherton TF, Mahamedi F, Striepe M, Field AE, Keel P. A 10-year
and Margit Kirk for technical assistance.
longitudinal study of body weight, dieting, and eating disorder symptoms. J Abnorm Psychol 1997;106(1):117–25.
Joiner TE, Heatherton TF, Keel PK. Ten-year stability and predictive validity of
five bulimia-related indicators. Am J Psychiatry 1997;154(8):1133–8.
Allik J. Personality dimensions across cultures. J Pers Disord 2005;19(3):212–32.
Kallasmaa T, Allik J, Realo A, McCrae RR. The Estonian version of the NEO-
Allik J, McCrae RR. Towards a geography of personality traits: patterns of
PI-R: an examination of universal and culture-specific aspects of the Five-
profiles across 36 cultures. J Cross-Cult Psychol 2004;35(1):13–28.
Factor model. Eur J Pers 2000;14:265–78.
Biederman J, Rivinus TM, Herzog DB, Ferber RA, Harper GP, Orsulak PJ, et al.
Keel PK, Klump KL. Are eating disorders culture-bound syndromes? Im-
Platelet mao activity in anorexia–nervosa patients with and without a major
plications for conceptualizing their etiology. Psychol Bull 2003;129
depressive disorder. Am J Psychiatry 1984;141(10):1244–7.
Bollen E, Wojciechowski FL. Anorexia nervosa subtypes and the Big Five
Kiive E, Merenäkk L, Harro M, Harro J. Changes in platelet monoamine oxidase
Personality Factors. Eur Eat Disord Rev 2004;12(2):117–21.
activity, cholesterol levels and hyperactive behaviour in adolescents over a
Brewerton TD. Toward a unified theory of serotonin dysregulation in eating and
period of three years. Neurosci Lett 2005;384(3):310–5.
related disorders. Psychoneuroendocrinology 1995;20(6):561–90.
Kotler LA, Cohen P, Davies M, Pine DS, Walsh BT. Longitudinal relationships
Brewerton TD, Hand LD, Bishop ER. The tridimensional personality ques-
between childhood, adolescent, and adult eating disorders. J Am Acad Child
tionnaire in eating disorder patients. Int J Eat Disord 1993;14(2):213–8.
Adolesc Psychiatry 2001;40(12):1434–40.
Brookings JB, Wilson JF. Personality and family—environment predictors of
Landen M, Sundblad C, Eriksson T, Bergman L, Eriksson E. Comparison of an
self-reported eating attitudes and behaviors. J Pers Assess 1994;63
androgen antagonist (flutamide) and a serotonin reuptake inhibitor (citalopram)
for the treatment of bulimia nervosa. Nord J Psychiatry 1999;53(2):96.
Carrasco JL, Diaz-Marsa M, Hollander E, Cesar J, Saiz-Ruiz J. Decreased
Markon KE, Krueger RF, Watson D. Delineating the structure of normal and
platelet monoamine oxidase activity in female bulimia nervosa. Eur Neu-
abnormal personality: an integrative hierarchical approach. J Pers Soc
ropsychopharmacol 2000;10(2):113–7.
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
Mccarthy DM, Simmons JR, Smith GT, Tomlinson KL, Hill KK. Reliability,
Rastam M, Gillberg C, Gillberg IC. A six-year follow-up study of anorexia
stability, and factor structure of the Bulimia Test-Revised and Eating
nervosa subjects with teenage onset. J Youth Adolesc 1996;25(4):439–53.
Disorder Inventory-2 scales in adolescence. Assessment 2002;9(4):382–9.
Rizvi SL, Stice E, Agras WS. Natural history of disordered eating attitudes and
McCrae RR, Costa Jr PT. Towards a new generation of personality theories:
behaviors over a 6-year period. Int J Eat Disord 1999;26(4):406–13.
theoretical context for the Five-Factor theory. In: Wiggins JS, editor. The
Steiger H. Eating disorders and the serotonin connection: state, trait and
Five-Factor Model of Personality: Theoretical Perspective. New York:
developmental effects. J Psychiatry Neurosci 2004;29(1):20–9.
Steiger H, Bruce K. Personality traits and disorders in anorexia nervosa, bulimia
McCrae RR, Costa Jr PT. A Five-Factor theory of personality. In: Pervin LA,
nervosa, and binge eating disorder. In: Brewerton TD, editor. Clinical
John OP, editors. Handbook of Personality. Theory and Research. 2 ed. New
Handbook of Eating Disorders: An Integrated Approach. New York: Marcel
York: Guilford Press; 1999. p. 139–53.
Mcelroy SL, Hudson JI, Malhotra S, Welge JA, Nelson EB, Keck PE.
Steiger H, Richardson J, Israel M, Ng Ying Kin MM, Bruce K, Mansour S, et al.
Citalopram in the treatment of binge-eating disorder: a placebo-controlled
Reduced density of platelet-binding sites for [3h] paroxetine in remitted
trial. J Clin Psychiatry 2003;64(7):807–13.
bulimic women. Neuropsychopharmacology 2005;30(5):1028–32.
Miller MN, Pumariega AJ. Culture and eating disorders: a historical and cross-
Sundblad C, Lunden M, Eriksson T, Bergman L, Eriksson E. Effects of the
cultural review. Psychiatry Interpers Biol Processes, 64(2). ; 2001. p. 93-110.
androgen antagonist flutamide and the serotonin reuptake inhibitor
Mussell MP, Binford RB, Fulkerson JA. Eating disorders: summary of risk
citalopram in bulimia nervosa—a placebo-controlled pilot study. J Clin
factors, prevention programming, and prevention research. Couns Psychol
Tachikawa H, Yamaguchi N, Hatanaka K, Kobayashi J, Sato S, Mizukami K, et
Nevonen L, Broberg AG. Validating the Eating Disorder Inventory-2 (EDI-2) in
al. The Eating Disorder Inventory-2 in Japanese clinical and non-clinical
Sweden. Eat Weight Disord 2001;6:59–67.
samples: psychometric properties and cross-cultural implications. Eat
Oreland L. Monoamine Oxidase in Neuropsychiatric Disorders. In: Yasuhara H,
Parvez SH, Oguchi K, Sandler M, Nagatsu T, editors. Monoamine Oxidase:
Tasca GA, Illing V, Lybanon-Daigle V, Bissada H, Balfour L. Psychometric
Basic and Clinical Aspects. Utrecht: VSP Press; 1993. p. 219–47.
properties of the Eating Disorders Inventory-2 among women seeking
Pallanti S, Quercioli L, Ramacciotti A. Citalopram in anorexia nervosa. Eat
treatment for binge eating disorder. Assessment 2003;10(3):228–36.
Thiel A, Jacobi C, Horstmann S, Paul T, Nutzinger DO, Schussler G. A German
Percevic R, Wolf M, Kordy H. Influence of the retest artefact on outcome
translation of the Eating Disorder Inventory EDI-2. Psychother Psychosom
measurement in psychotherapy— the Inventory of Interpersonal Problems
Med Psychol 1997;47(9–10):365–76.
and the Eating Disorder Inventory. Z Klin Psychol Psychiatr Psychother
Tylka TL, Subich LM. Exploring the construct validity of the eating disorder
continuum. J Couns Psychol 1999;46(2):268–76.
Podar I, Hannus A, Allik J. Personality and affectivity characteristics associated
Verkes RJ, Pijl H, Meinders AE, Vankempen GMJ. Borderline personality,
with eating disorders: a comparison of eating disordered, weight-pre-
impulsiveness, and platelet monoamine measures in bulimia nervosa and
occupied, and normal samples. J Pers Assess 1999;73(1):133–47.
recurrent suicidal behavior. Biol Psychiatry 1996;40(3):173–80.
Pollock-Barziv SM, Davis C. Personality factors and disordered eating in young
Wonderlich S, Mitchell JE. The role of personality in the onset of eating
women with type 1 diabetes mellitus. Psychosomatics 2005;46(1):11–8.
disorders and treatment implications. Psychiatr Clin North Am 2001;24
Pulver A, Allik J, Pulkkinen L, Hämäläinen M. A Big Five personality inventory
in two non-indo-european languages. Eur J Pers 1995;9:109–24.
• Spain has complied with its 2011/2012 interim target and the 2011 NREAP target. Spain’s revised NREAP published in 2011 sets the 2020 overall target share at 20.8%, lower than the original NREAP’s target of 22.7%, but still higher than the binding minimum of 20% set in the Directive. • Compared to the average of the previous six years, growth between 2010 and 2011 slowed down in the ele
Guidelines for Treatment of Malaria in the United States (Based on drugs currently available for use in the United States) CDC Malaria Hotline: (770) 488-7788 Monday-Friday 8 am to 4:30 pm EST 488-7100 after hours, weekends and holidays (ask to page the malaria person on-call) Clinical Diagnosis/ Region Infection Acquired Recommended Drug and Adult Dose1,8 Recommended

 Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx – xxx
Psychological traits and platelet monoamine oxidase activity in eating
disorder patients: Their relationship and stability
Iris Podar a,⁎, Maiken Jaanisk a,b, Jüri Allik a, Jaanus Harro a,b
a Department of Psychology, University of Tartu, Tiigi 78, Tartu 50410, Estonia
b The Estonian Centre of Behavioral and Health Sciences, University of Tartu, Tartu 50410, Estonia
Self-reported behavior and attitudes towards eating [Eating Disorder Invetory-2; Garner DM (1991). Eating Disorder Inventory-2: Professional
Manual. Odessa, Fl.: Psychological Assessment Resources; Estonian version Podar I, Hannus A, Allik J (1999). Personality and AffectivityCharacteristics Associated With Eating Disorders: a Comparison of Eating Disordered, Weight-Preoccupied, and Normal Samples. J Pers Assess;73(1), 133–147] and the activity of platelet monoamine oxidase (MAO) was studied in 11 patients with anorexia nervosa (AN), 43 patients withbulimia nervosa (BN) and a healthy control group (n = 138). Nineteen patients filled in the EDI-2 questionnaire and donated blood samples threetimes with three month intervals in order to determine platelet MAO activity. Eating disordered (ED) patients scored higher on all EDI-2 subscalesand had lower MAO activity compared to the control group. They also scored higher than the control group on the Neuroticism domain but loweron the Extraversion, Openness, and Conscientiousness domains of the NEO-PI-R questionnaire. The average stability of MAO on differentoccasions (r = .56) was slightly smaller than the stability of the EDI-2 scores (r = .70). The lack of correlations between personality dispositions andMAO activity indicates that they have independent influence on eating disorders. A possible relationship between neurochemical mechanisms andpsychological symptoms of eating disordered behavior is discussed.
Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx – xxx
Psychological traits and platelet monoamine oxidase activity in eating
disorder patients: Their relationship and stability
Iris Podar a,⁎, Maiken Jaanisk a,b, Jüri Allik a, Jaanus Harro a,b
a Department of Psychology, University of Tartu, Tiigi 78, Tartu 50410, Estonia
b The Estonian Centre of Behavioral and Health Sciences, University of Tartu, Tartu 50410, Estonia
Self-reported behavior and attitudes towards eating [Eating Disorder Invetory-2; Garner DM (1991). Eating Disorder Inventory-2: Professional
Manual. Odessa, Fl.: Psychological Assessment Resources; Estonian version Podar I, Hannus A, Allik J (1999). Personality and AffectivityCharacteristics Associated With Eating Disorders: a Comparison of Eating Disordered, Weight-Preoccupied, and Normal Samples. J Pers Assess;73(1), 133–147] and the activity of platelet monoamine oxidase (MAO) was studied in 11 patients with anorexia nervosa (AN), 43 patients withbulimia nervosa (BN) and a healthy control group (n = 138). Nineteen patients filled in the EDI-2 questionnaire and donated blood samples threetimes with three month intervals in order to determine platelet MAO activity. Eating disordered (ED) patients scored higher on all EDI-2 subscalesand had lower MAO activity compared to the control group. They also scored higher than the control group on the Neuroticism domain but loweron the Extraversion, Openness, and Conscientiousness domains of the NEO-PI-R questionnaire. The average stability of MAO on differentoccasions (r = .56) was slightly smaller than the stability of the EDI-2 scores (r = .70). The lack of correlations between personality dispositions andMAO activity indicates that they have independent influence on eating disorders. A possible relationship between neurochemical mechanisms andpsychological symptoms of eating disordered behavior is discussed.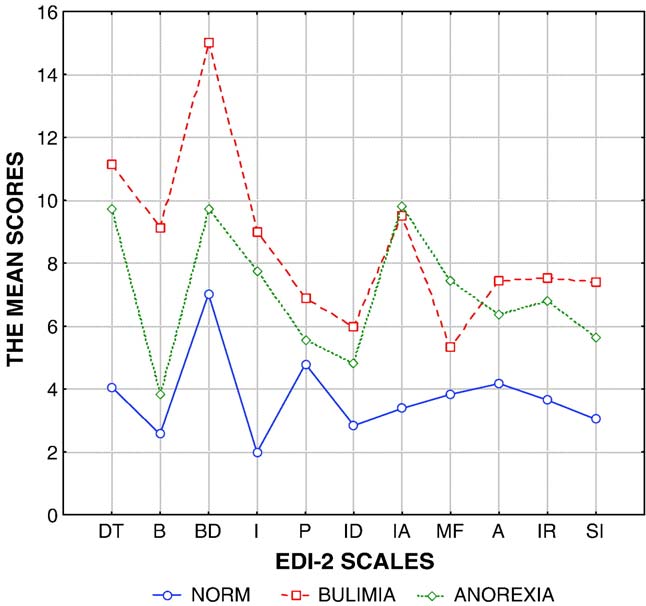 I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
sessions). All participants were females aged 16–37 years
activity was measured as previously described (
(Mean = 20.1; S.D. = 4.5) and their mean body mass index (BMI;
) and expressed as nanomoles of β-phenylethylamine
the body weight in kilograms divided by the squared height in
oxidized per 1010 platelets/min. On the first time all the patients
meters) was 19.77 (S.D. = 2.8). Eleven patients were smokers.
I. Podar et al. / Progress in Neuro-Psychopharmacology & Biological Psychiatry xx (2006) xxx–xxx
sessions). All participants were females aged 16–37 years
activity was measured as previously described (
(Mean = 20.1; S.D. = 4.5) and their mean body mass index (BMI;
) and expressed as nanomoles of β-phenylethylamine
the body weight in kilograms divided by the squared height in
oxidized per 1010 platelets/min. On the first time all the patients
meters) was 19.77 (S.D. = 2.8). Eleven patients were smokers.