Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Bsp15
SCAR FORMATION KEY FIGURES:
This chapter gives background information about the scarring process. Treatment options for problematic scars are also discussed. Normal Course of Scar Maturation
Scar tissue is never as strong as normal, uninjured skin. For the first3–4 weeks after injury, the wound can easily be reopened by minimaltrauma. By 6 weeks, the scar has attained approximately 50% of itsfinal strength. During the next 12 months, the scar gradually increasesits ability to withstand injury, but it never attains normal strength.
The period of maximal collagen production (the primary component ofskin and scar tissue) is the first 4–6 weeks after a wound has closed. During this period the scar may appear red and be slightly firm andraised.
Over the next several months, changes in the rate of collagen produc-tion and degradation occur. Normal healing results in normal typesand amounts of collagen in the area. On the surface, normal healing isillustrated by the fading of redness and softening of the scar.
I usually tell patients that it will take at least 1 year for the scar toachieve its final appearance. Scars in children may continue to changeand improve for several years.
Practical Plastic Surgery for Nonsurgeons
Abnormal Scarring
For various reasons, such as genetics, nature of initial injury, or badluck, some scars become exceptionally red, thick, and tight. Such scarscan be problematic on the hand or other flexor surfaces, because theymay lead to limitation of movement and loss of function. Hypertrophic scars are a bit thicker and redder than the fine scar that usually results after primary healing. At the extreme, scars may become keloids—that is, they may enlarge beyond their initial area. Keloids can become large and unsightly. They also can cause annoying symptoms, such as itching and pain.
Typical hypertrophic scar. Note that the scar is thick and raised but still withinthe confines of a normal scar.
In addition, the scar may be unstable. An unstable scar is easily rein- jured with minimal trauma; it heals but is easily injured again. This cycle can go on for years and ultimately result in the development of an aggressive form of skin cancer.
Abnormal scarring is usually the result of abnormal collagen produc-tion and degradation. Although we do not know the exact cause ofthese abnormal processes, the manner in which a wound is closed mayplay a role. In addition, there are interventions that can improve an ab-normal scar. Method of Wound Closure
Usually, the best (i.e., least noticeable) scar results when a wound isclosed by suturing the skin edges together. Usually the sutures are re-moved before the 14th day after repair. As explained above, at this pointthe scar is not very strong; in fact, it has < 15% of its final strength. Normal everyday movements will pull on the scar and may result inwidening of the scar.
For this reason, most plastic surgeons place buried dermal sutures aswell as the usual skin sutures when they close a wound (see figurebelow). Buried dermal sutures are not difficult to place, but this extrastep is time-consuming. The dermal sutures add strength to the repairsite during the weeks to months required for their absorption. Theanticipated result is less widening and an improved appearance ofthe scar.
Buried dermal sutures are used to hold together the skin edges and thereby de-crease tension on the external sutures. In theory, placement of a few burieddermal sutures decreases the risk for hypertrophic scarring and keloid formation.
When dermal sutures are not used, be sure that the skin sutures pro-vide good dermis-to-dermis approximation. It also is important toremove the sutures at the appropriate time (see chapter 1, “Suturing:The Basics”). Sutures that are left in place too long cause an inflamma-tory response that worsens scar appearance.
If Steristrips are available, put them across the suture line when the su-tures are removed. This simple step gives the scar a bit of extra strengthduring the period when it is vulnerable to injury.
Wounds that are allowed to heal secondarily often have larger, morenoticeable scars than ones closed primarily. Secondary wound closure
Practical Plastic Surgery for Nonsurgeons
also is associated with a higher incidence of hypertrophic scarring andkeloid formation. How the Patient Can Help
Once the sutures have been removed and the wound looks well healed, rubbing or gently massaging the scar with a mild moisturizing cream (e.g., Vaseline, aloe, cocoa butter) a few times each day promotes softening and lightening of scar tissue, especially on the face and hands. A cream with vitamin E may be helpful. Patients should not spend a large sum of money on fancy creams because no conclusive evidence indicates that ex- pensive formulations improve the scar’s final appearance. Gentle massage should be continued for at least 4–6 weeks.
Patients should stay out of the sun as much as possible, and always use a sunscreen (SPF > 20). Scars exposed to the sun (especially if sunburn dvelops) not only stay red longer but also may not fade as much as normally expected.
All patients should maintain good nutrition, and diabetics should maintain good glucose control.
Providers must counsel patients aggressively about the ill effects of tobacco products on wound healing. Some of the components in ciga- rettes cause a decrease in blood circulation to the skin, which results in poor wound healing and may even lead to tissue loss. Dramatic ad- verse reactions due to the effects of smoking have been reported. Interventions for Problematic Scars
These treatments can be tried individually or in some combination.
Instruct the patient in the massage techniques described above.
Once the sutures have been removed and the wound looks wellhealed, you can cover the wound with silicone gel sheets. Although itis not entirely understood how they work, silicone gel sheets can bequite effective. They can be obtained from pharmacies but usually re-quire a prescription (although this policy is changing in the UnitedStates). How to use the silicone gel sheet
1. Cut a piece large enough to cover the scar completely.
2. The sheet should be left in place as long as tolerated—even all day.
The longer it is in place, the better.
3. The patient should remove the sheet to wash. Deodorant soaps
should not be used to cleanse the area; they may cause a rash. Onepiece of gel sheet can be used repeatedly.
4. Sheets should be used for at least 2–3 months to make an apprecia-
The purpose of splinting is to prevent loss of function and restriction ofmovement from a tight scar. Especially on the hand and in a crease,splinting can be quite useful. The splint should be molded so that itstretches the tight scar. Case example: If a tight scar across the front of elbow prevents the pa- tient from fully extending the forearm, the following steps may help:
• Make a splint that holds the elbow in as much extension as tolerated.
Gradually the scar will become less tight because of the remodelingdue to splinting and scar massage (remember, you can add other“scar is too tight” treatments). With time the patient will be able toextend the elbow more fully.
• The splint can be made out of simple plaster of Paris (see chapter 28,
“Hand Splinting and General Aftercare”).
• If the splint interferes with the patient’s ability to work, encourage
• New splints should be made as the patient can more fully extend at
• This process may take many months, but is worth the effort to im-
Pressure garments, measured and fitted to the individual patient, canbe worn under everyday clothing. They are designed to apply continu-ous pressure over the area of concern. Theoretically, the pressure causesthe underlying scar to become ischemic and thus leads to remodeling.
Pressure garments should be worn 18–24 hours/day for a minimum of4–6 months. Medical supply stores and pharmacies can order pressuregarments, which are expensive. Prescriptions usually are required.
Practical Plastic Surgery for Nonsurgeons
Reassure the patient that scars will fade on their own, but the processtakes time. Remind the patient to avoid sun exposure whenever possi-ble and to use sunscreen when exposure cannot be avoided. Ultravioletlight injures normal skin as well as scars. A sunburned scar may notfade as well as normally expected.
Once the sutures have been removed and the wound looks well healed,the patient can apply gentle make-up until the scar fades on its own. Itis best to use make-up with a sunscreen to prevent sun injury. Make-upalone does not protect the tissues from the ill effects of the sun.
Try the treatments described under “Scars that are Too Tight.” Massage,silicone gel sheets, splinting, and pressure garments may help. In addi-tion, the treatments listed below may be useful. Each can be tried indi-vidually, but often they work better in combination with anothermethod. For example, inject the keloid with steroids and use a pressuregarment daily. Or excise the keloid, close the wound meticulously, andthen use silicone gel sheeting after the sutures have been removed.
Inject triamcinolone acetonide into the dermis of the keloid—approxi-mately 1 mg for every 1–2 cm of scar. It is best to use a tuberculin sy-ringe because you are working with small amounts of medication. Besure to check the mg/ml of the solution (different bottles may have dif-ferent drug concentrations). The total amount of injected triamcinoloneshould not exceed 30 mg. Caution: Steroid injection hurts. You can add 0.5–1.0 ml of lidocaine to the steroid solution.
It takes several weeks to see any noticeable change in the scar. Steroidinjection can be repeated after 4–6 weeks, but I do not recommend in-jecting the same area more than 2 or 3 times. The response to steroid in-jection is quite variable. The reported percentages of patients obtainingsome improvement (not necessarily resolution of the scar) after steroiduse range from 50% to 100%.
The patient should be warned of the risks associated with the injectionof steroids. Infection may develop at the injection site, and the injected
area may become lighter in color than the surrounding skin. Be espe-cially careful in treating diabetic patients. Steroids may cause an eleva-tion of blood glucose level.
Some patients develop keloids after ear piercing. Earrings designed toapply pressure to the earlobe are commercially available. They workbest on small keloids (< 1 cm). Pressure earrings are especially usefulwhen combined with excision of the keloid. Once the excision sutureshave been removed, the patient should wear the earring for at least 2or 3 months (longer is better). This approach may prevent recurrenceof the keloid. Caution: Excision of a keloid often results in formation of another keloid. The recurrence rate after excision ranges from 45% to 100%.
At times, however, it is worthwhile to excise the bothersome keloid. Forexample, patients with a keloid associated with ear piercing may have asuccessful outcome if, as previously described, after excision they wear acompression earring regularly. Another example when excision may besuccessful is if the initial injury was not closed with sutures (i.e., it wasallowed to heal secondarily). In this case, excision of the keloid followedby primary skin closure may be helpful. Even under these more favor-able circumstances, you must warn patients that the keloid may recur.
If you excise the keloid, a close dermal approximation of the skin edgesis especially important. Close approximation requires placement ofburied dermal sutures prior to skin closure. Therefore, excision of akeloid and primary closure should be undertaken only by clinicianswith excellent suturing skills.
If radiation therapy facilities are available, low-dose therapy helps toprevent the development of a keloid. Usually it is performed only onpatients known to develop severe keloids who are scheduled for surgi-cal procedures. The radiation is administered as early as the first post-operative day.
As with other treatment methods, the success rate is variable, rangingfrom 10% to 94% in different studies.
Practical Plastic Surgery for Nonsurgeons
When larger wounds or wounds over creases are allowed to heal sec-ondarily, the scar may be easily injured and reopen. Although usuallyit heals with local wound care measures, this cycle often repeats itselfagain and again. Excision of the entire scar may be indicated. The re-sultant skin defect requires closure with a more durable skin graft orflap (see chapters 12, 13, and 14 on “Skin Grafts,” “Local Flaps,” and“Distant Flaps” for details about these techniques). Bibliography
Niessen FB, Spauwen PHM, Schalkwijk J, Kon M: On the nature of hypertrophic scarsand keloids: A review. Plast Reconstr Surg 104:1435–1458, 1999.
PATIENT INFORMATION SHEET – METFORMIN Metformin is a medication used for treatment of the symptoms of polycystic ovaries. It has been used for 40 years in the treatment of some types of diabetes. It works by reducing the insulin resistance of the ovaries in polycystic ovary syndrome (PCOS). Metformin may improve the quality of the eggs and the pregnancy rate in women with polycystic o
The Vermont Phoenix , From the Columbian [ Lady’s and Gentleman’s ] Magazine for April [1844]. L U C Y M A Y N A R D . BY MISS MARTHA RUSSELL. “A lily fair which God did bless, And which from Nature’s heart did draw Love, wisdom, peace and heaven’s perfect law.” READER , have you ever travelled in Connecticut, over that part of New Haven county
 SCAR FORMATION
SCAR FORMATION Practical Plastic Surgery for Nonsurgeons
Abnormal Scarring
Practical Plastic Surgery for Nonsurgeons
Abnormal Scarring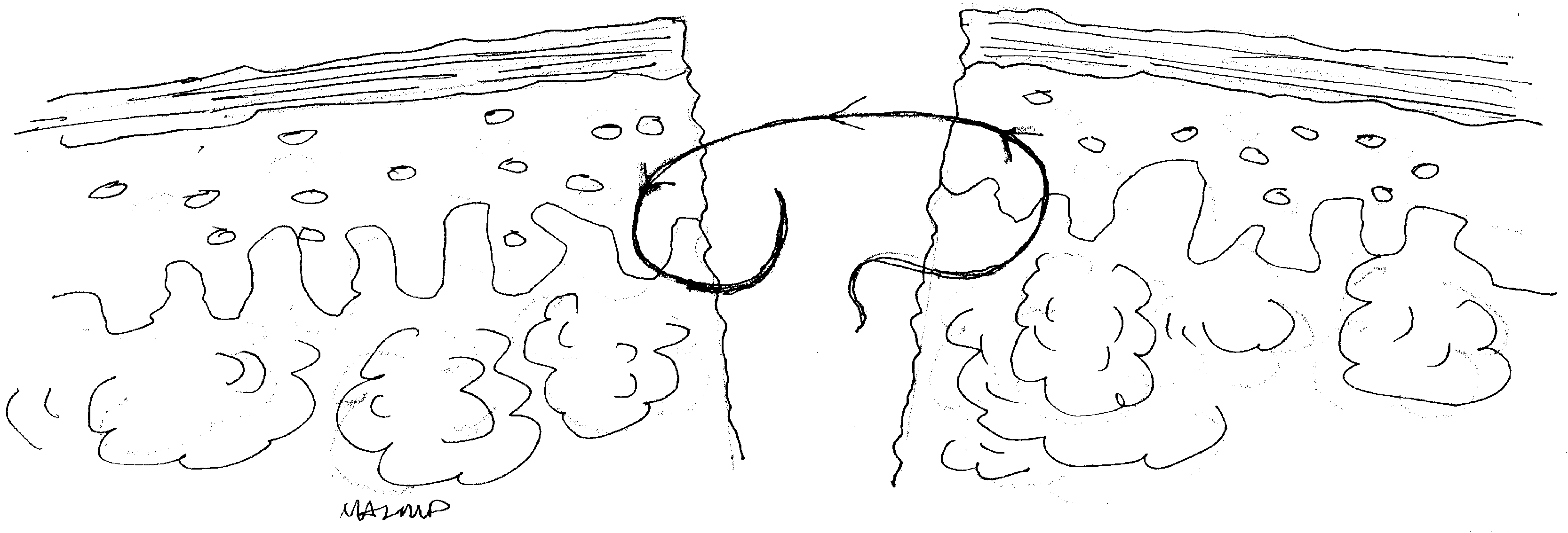 Method of Wound Closure
Method of Wound Closure