Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Microsoft word - 006 - alisa jan 12.doc
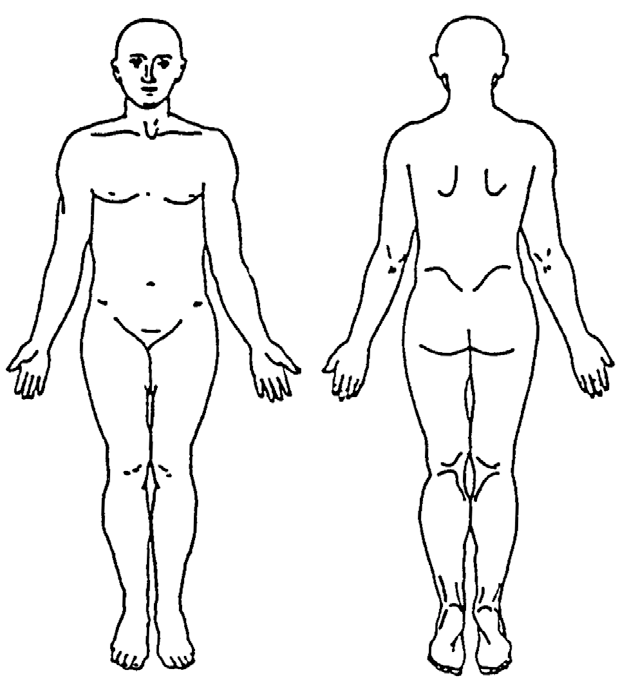
PATIENT PAIN ASSESSMENT Part A: Body and Pain Scale Please mark, on the drawings below, the areas where you feel pain.
Write “E” if external or “I” if internal. Write “EI” if both external and internal. Please use numbered pain scores and additional descriptive words like: neuropathic, intense (deep or
surface), sharp, hot, dull, cold, sensitive, tender, itchy, shooting, numb, electrical, tingling, cramping, radiating, throbbing, aching, heavy, or unpleasant.
If you are unable to annotate the illustration, please see Part E. PATIENT PAIN ASSESSMENT Part B: Initial Assessment & History:
Chief complaint/Current Medical History: Crohn’s Disease Past Medical/Surgical History: 2005 and 2012 colonoscopy
Pain Management History/Regimen: Immunosuppressants (Imuran) and steroids. Also
tried once to switch to Humira, but decided the shots were too painful to continue. Present Pain Management Regimen: Immunosuppressants (Imuran) and medical marijuana.
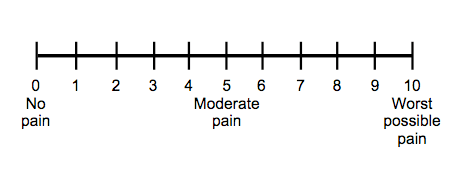
Acceptable level of pain: Pain score: (Choose between 0 - 10) __4___ Patient’s pain goal: _X_ Decreased Pain __ No pain __ Resume Activities of Daily Life
Part C: Questions
What are the aggravating factors? Is there an activity or an inactivity that causes pain? Is there a certain time of day when the pain is worse?
Mainly stress and menstruation. When there is a flare happening, the pain is worse in the
morning and evenings. The pain seems to subside during the afternoon. What are the relieving factors? Does repositioning help? Common pain relief like tylenol? Does cold/warm application, massage, distraction, reposition, art therapy or music help? Laying down and eating a very bland diet. Sometimes curling up into the fetal position
helps. Also, the use of warm compresses can help. How is your physical activity and mobility? How does your daily physical activity compare today to before your illness? How does your pain affect your day and your productivity?
My physical activity is even less than compared to before my illness. Doctors always recommend exercising more, but I don’t usually have the motivation to do it, especially
during a flare. Depending on the level of pain determines how much I can get done in a day. Sometimes there are days where all I can do is just lay in bed and rest.
Do you participate in fewer activities because of pain or fear of onset of pain? Yes. I do not participate in physical activities like I used to. I also fear that certain
symptoms that come along with Crohn’s will arise.
PATIENT PAIN ASSESSMENT How do you feel emotionally—now or when you had or have pain? Does your pain provide you with a positive outlook? Are you happier on days without pain? It took a while to cope with the pain but now that it has been a few years, I think that it has
helped become stronger emotionally. I am happier on days without pain. Part D: Additional Questions (Optional)
Do you view your pain as something temporary or permanent? How has successful or unsuccessful pain management contributed to this belief? My pain will be permanent since my condition is chronic, but I have found some very
successful pain management that I think will help me live a fulfilled life.
Do you feel this experience has prevented personal growth? Encouraged it? Yes, of course. This particular experience helped me understand that it’s way more
common than I thought and it has encouraged my curiosity of the human body. How has pain affected your personal relationships or social life? Are you more withdrawn? Feel isolated? See friends more or less often? I did lose some personal relationships from my pain and it has caused me to be more
withdrawn. I can no longer drink alcohol so social events can be more of a drag than
anything. But my really good friends have always stayed by my side and continue to be extremely supportive.
Do you share with those around you about your experience? How do the people you share with respond—empathy, love, pity, disregard, etc.?
Some people don’t always know what Crohn’s Disease is but everyone is always very empathetic and loving. My family and friends have been incredible during my years of
coping and finding pain management that works for me.
How has/have others’ reaction to your experience effected you? Do you feel comforted, supported, alienated, ignored?
Everyone’s reactions have made me proud of my disease. Yes, there are some gross symptoms that come along with this disease, but that doesn’t make me a gross person.
Besides, everyone has had one of the symptoms at least once in their lifetime so there is nothing to be ashamed of. I am completely supported by the people who matter.
PATIENT PAIN ASSESSMENT Part E: Describing Pain (if unable to mark body scale). Repeat as necessary.
Location of Pain: Lower abdomen X_Shooting
_X_Sharp _X_Pressure
__Radiating _X_Other: Cramping
2. Type: _X_Acute
3. Intensity: 0 – 10 (10 being the worst pain you’ve ever felt): __10___
__Radiating __Other: ___________________
6. Intensity: 0 – 10 (10 being the worst pain you’ve ever felt): _____
A Guide to Computing with Statistics with SPSS Release 10 for Windows: With Supplements for Releases 8and 9, Dennis Howitt, Duncan Cramer, Prentice Hall PTR, 2000, 0130326852, 9780130326850, . This text isdesigned for statistics courses taught in departments of Psychology. SPSS Guide to Computing for Windows10.0 walks students through the process of data analysis in straightforward, intuitive st
HEALTH PROFILE and PARENT CONSENT FORM All sections of this form must be completed as part of the enrollment application for Caronport High School. Although a medical exam is not required, it is advised that all students have medical, dental and eye exams as well as all routine immunizations up to date prior to their arrival on campus. Students competing in Cougar Athletics may be req
 PATIENT PAIN ASSESSMENT
PATIENT PAIN ASSESSMENT