Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Overcoming radiation resistance in inflammatory breast cancer
Overcoming Radiation Resistance inInflammatory Breast Cancer*
Wendy A. Woodward, MD, PhD; Bisrat G. Debeb, PhD; Wei Xu, PhD; and Thomas A. Buchholz, MD
The clinical-pathological features of inflammatory breast cancer include enrichment of factors that have been previ-
ously associated with radioresistant disease, including negative hormone receptor status and a phenotype enriched
for relatively radioresistant breast cancer stem/progenitor cells. The risks and benefits of accelerated postmastec-
tomy radiation treatment regimens in the multimodality management of inflammatory breast cancer were reviewed
at the first International Inflammatory Breast Cancer Conference at The University of Texas M. D. Anderson Cancer
Center. The biological basis for radiation resistance and strategies to radiosensitize these tumors were also presented.
The prevalent basal phenotype of inflammatory breast cancer makes it an ideal clinical model to examine stem cell
hypotheses, which the authors believe can help guide future trials to continue making incremental progress against
this aggressive disease. Cancer 2010;116(11 suppl):2840–5. V
KEYWORDS: cell lines, inflammatory breast cancer, radiation, surgery, chemotherapy, history, stem cells,mammospheres.
Currently, the most widely referenced definition of inflammatory breast cancer (IBC) is that of the American JointCommittee on Cancer,1 which states in part that inflammatory carcinoma is a clinicopathologic entity characterized bydiffuse erythema and edema (peau d’orange) of the breast, often without an underlying mass. These clinical findingsshould involve the majority of the breast. It is important to remember that inflammatory carcinoma is primarily a clinicaldiagnosis. Involvement of the dermal lymphatics alone does not indicate inflammatory carcinoma in the absence of clini-cal findings.
The unique features of the primary disease in IBC make optimal local/regional management a critical component of
the multidisciplinary care of IBC. The current standard or care in the management of IBC includes neoadjuvantchemotherapy Æ trastuzumab for appropriate patients, modified radical mastectomy, and high-dose postmastectomy radi-ation targeting the chest wall skin and soft tissue as well as the draining lymphatics. Clearly the skin is a target in IBC, andcare must be taken to ensure adequate dose and skin reaction. Importantly, ‘‘despite the rapid progressive nature of IBC,70% of patients present with local/regional disease without distant metastases at diagnosis,’’2 highlighting the potentialfor improved cure rates with adequate local/regional disease control.
Before the introduction of effective chemotherapy in the management of solid tumors, the 5-year actuarial overall
survival for IBC was <5%, with a median survival of only 15 months. Modified radical mastectomy was not technicallypossible for many patients with IBC because of the extent of disease on the chest wall at presentation. It was often difficultto achieve negative margins, and there was little or no benefit to a positive margin surgery. This led to the use of primaryradiotherapy as the sole treatment modality yielding excellent symptom palliation, with modest short-term local controlrates of 50%.
In this era, The University of Texas M. D. Anderson Cancer Center initiated a pilot study of altered-fractionation
radiation therapy with the intent of intensifying the radiation dose and improving local control. Among 80 patients stud-ied, 69 patients received standard fractionation of 2 gray (Gy) per day to the chest wall and draining lymphatics. With this
Corresponding author: Wendy A. Woodward, MD, Assistant Professor of Radiation Oncology, The University of Texas M. D. Anderson Cancer Center, Box 1202,1515 Holcombe Blvd, Houston, TX 77030; Fax: (713) 563-6940; [email protected]
Division of Radiation Oncology, The University of Texas M. D. Anderson Cancer Center, Houston, Texas
The articles in this supplement were presented at the First International Inflammatory Breast Cancer Conference, Houston, Texas, December 5-7, 2008.
*Proceedings of the First International Inflammatory Breast Cancer Conference, Supplement to Cancer.
DOI: 10.1002/cncr.25173, Received: December 1, 2009; Accepted: January 14, 2010, Published online May 19, 2010 in Wiley InterScience (www.interscience.wiley. com)
Radiation and Inflammatory Breast Cancer/Woodward et al
regimen, patients received a total of 50 Gy þ a 10- to 16-
before radiation therapy commenced. For the entire
Gy boost to gross disease. Eleven patients received twice-
cohort of 256 patients, the 5-year actuarial distant metas-
daily fractionation treatment of 1.5 Gy per treatment to a
tasis-free survival, local control, and overall survival were
total of 51 Gy þ a 15- to 20-Gy boost to gross disease.
40%, 76%, and 44%, respectively.8 Not unexpectedly,
Although this was a small study, the local control was
5-year overall survival was significantly improved for
54% in the once-a-day arm versus 73% in the altered frac-
patients who completed all therapy, 51% versus 24%
tionation arm.3 In 1974, the introduction of doxorubicin
(P ¼ .0001), and the local/regional control rate was 84%
chemotherapy yielded another significant gain in IBC
for patients who completed all therapy. This rate of local/
outcome. Although the addition of chemotherapy had no
regional control was higher than historical rates. Examina-
effect on local control (73% vs 74%3), the 5-year survival
tion of the factors that predicted for local recurrence after
improved from <5% to 30%-50% because of the reduc-
radiation among patients in Group 1 revealed that age
tion in distant metastasis. Importantly, the addition of
<45 years, less than partial response to chemotherapy, !4
chemotherapy rendered more patients operable, and
positive lymph nodes, lack of taxane use, and positive or
modified radical mastectomy was reintroduced. Several
unknown surgical margins were all associated with
series subsequently reported the local control benefit of
increased risk of local/regional recurrence. Patients with
mastectomy in the setting of systemic chemotherapy,
any 1 of these factors had higher rates of local/regional re-
demonstrating an absolute increase in local control of
currence, ranging from 21% to 52%. Dose escalation
24% to 45%.4-6 In the postmastectomy setting, however,
(60 vs 66 Gy) appeared to have the most significant bene-
total radiation dose was lowered from a gross disease dose
fit in these high-risk groups, with age <45, positive/
of 66 to 70 Gy to a microscopic disease dose of a standard
unknown margins, and disease unresponsive to chemo-
60 Gy. Although this lowered the complication rates
therapy. Given the higher rate of grade 3 toxicity at 5 years
related to radiotherapy, local failure remained a challenge,
with dose escalation (29% vs 15%, P ¼ .08), we now
with local failure rates exceeding 20%.7 Demonstrating
reserve dose escalation for patients with high-risk features
that this was a problem of radiation resistance to this low-
ered dose, the majority of these local failures were centeredin the radiation field on the chest wall. This provided therationale for dose escalation in the setting of postmastec-tomy radiation, and in 1987, a dose escalation regimen
was introduced for IBC patients at The University of
Texas M. D. Anderson Cancer Center consisting of 51
The clinical-pathological features of IBC include enrich-
Gy to the chest wall and draining lymphatics, and a 15-
ment of factors that have been previously associated with
Gy boost to the chest wall (to 66 Gy total) delivered at 1.5
radioresistant disease, including negative receptor status
Gy/fraction twice daily. Treating twice a day reduced the
(estrogen and progesterone9,10) and a phenotype enriched
overall treatment time from 6 to 41=2 weeks, an example of
for relatively radioresistant breast cancer stem/progenitor
the early dose-dense strategy in radiation therapy.
cells.11-13 In general, it is clear that although treatment
In 2008, a retrospective analysis was performed of
advances have been made, clinical experience demon-
all patients with nonmetastatic IBC cancer treated at The
strates a relative radioresistance of IBC tumors compared
University of Texas M. D. Anderson Cancer Center over
with non-IBC breast tumors, where local failure rates after
the progression of these treatment strategies from 1977 to
contemporary postmastectomy radiation are <10%.14
2004.8 Patients who were initially intended to receive
Although improved local control can be achieved in IBC
neoadjuvant chemotherapy, modified radical mastec-
with dose escalation, the cost in terms of toxicity can be
tomy, and postmastectomy radiation were included
high, and alternative approaches to radiosensitize these tu-
regardless of whether they were able to complete all ther-
apy and grouped by those who completed all therapy or
Laboratory investigations of available IBC cell lines
those who did not, often because of progressive disease.
SUM-149 and SUM-190 demonstrate relative radiore-
Among 256 patients analyzed, 192 completed all therapy
sistance of these lines (data not shown), making them
(Group 1), whereas 64 did not and received either preop-
good models for investigation of radioresistance mecha-
erative radiation (n ¼ 21) or definitive radiation (n ¼ 21).
nisms. Radiation resistance is classically assessed by clono-
An additional 22 patients developed a local recurrence
genic cell survival curves, which are generated by counting
Figure 1. Flow cytometric analysis of expression of CD24 and CD44 in SUM149 inflammatory breast cancer (IBC) cells is shown. SUM149 IBC cells were cultured under adherent (2-dimentional [2D]) or tumor-initiating cells enrichment condition (3D). Cellswere stained with CD24 and CD44 antibodies conjugated with different dyes and subjected to cytometric analysis. (A) The distri-bution of CD24 and CD44 expression in 1 representative experiment is shown: (A1) cells cultured in 2D condition stained withCD24 only; (A2) cells cultured in 3D condition stained with CD44 only; (A3) cells grown in 2D condition stained with both CD24and CD44; (A4) cells grown in 3D condition stained with both CD24 and CD44. (B) The relative increase of CD44 þ CD24lowpopulation in cells cultured in 3D condition compared with that in 2D condition is shown. The result is a summary of 5 independ-ent experiments. *P < .05.
colonies produced from cells that survive radiation and
factors in the search for selective cancer stem cell radiosen-
are capable of dividing clonally. The primary mechanism
of radiation cell killing in solid tumors is mitotic cell deathrather than apoptosis, and as such, this long-term assess-
ment of replicative potential eliminates cells that may per-
Although novel targeted cancer stem cell radiosensitizers
sist briefly after radiation but are destined to die after a
are desirable, they are still in early in clinical development,
few cell divisions and thus are not likely to be capable of
and it will be some time before optimal strategies are
defined. In the meantime, building on published and
Clonogenicity has been commonly assessed in
institutional experience with the oral prodrug of 5-fluo-
monolayer culture in serum containing media that may
ruracil, capecitabine,19 we have activated a new protocol
diminish the stem or progenitor cells’ potential in the cul-
for patients with progressive primary IBC to radiosensitize
ture system.15,16 Because normal and cancer stem/progen-
the primary tumors during radiation using capecitabine.
itor cells from mammary gland have been shown to be
On the basis of the long history of 5-fluorouracil
resistant to radiation compared with bulk, differentiated
chemotherapy for breast cancer and the encouraging
cells,11,12,17 we have compared clonogenicity of IBC cell
safety and efficacy results for preoperative concurrent
lines assessed in 2-dimensional (2D) monolayer clono-
capecitabine and radiation in rectal cancer,20,21 this
genic assays as well as in 3-dimensional serum-free growth
approach was advocated for carefully selected breast can-
factor-enriched clonogenic assays designed to support
cer patients with inoperable breast cancer who had no
stem/progenitor cells in in vitro culture.15 Exposure to
better treatment options at The University of Texas
stem cell-promoting media increases the percentage of tu-
M. D. Anderson Cancer Center. In a retrospective review
mor-initiating cells that have been prospectively identified
of 55 patients treated with concurrent radiation and
as CD44high/CD24low18 (Fig. 1) from human breast
capecitabine at The University of Texas M. D. Anderson
cancers. These tumor-initiating cell populations are more
Cancer Center for inoperable breast cancer (IBC and
resistant to radiation in clonogenic assays compared with
non-IBC), concurrent chemoradiation with capecitabine
the adherent population (Fig. 2). This assay system pro-
demonstrated 91% of these patients converted to having
vides an effective model to test pharmacologic and genetic
operable disease after treatment.22 The clinical complete
approaches to inhibit putative cancer stem cell survival
response rate was 33%; moreover, the overall pathological
Radiation and Inflammatory Breast Cancer/Woodward et al
Figure 2. Tumor-initiating cells from inflammatory breast cancer (IBC) cell lines are more resistant to radiation than monolayer(2-dimensional [2D]) cells. Clonogenic survival assay of IBC cells derived from (A) SUM149 and (B) SUM190 cultured under 2D ormammosphere (3D) cultures is shown. Cells in 3D are more resistant to radiation than cells grown in 2D. Cells were grown in 2Dor 3D culture conditions and irradiated with single, increasing doses (0, 2, 4, 6 gray [Gy]) of radiation.
complete response rate was 20%. Only 1 patient had pro-
To assess the efficacy and toxicity prospectively, to
gressive disease. The 5-year overall survival, local recur-
set the bar for upcoming novel radiosensitizers, and to
rence-free survival, and distant metastasis-free survival
permit the correlation of breast cancer stem cells in the
rates were 48%, 85%, and 37%. Sixteen (29%) patients
primary tumor pre- and post-radiation therapy to out-
had a grade 3 or higher complication (acute yet resolving
come, we have recently activated a single-arm phase 2
study to quantify response, conversion to operable among
In a phase 2 study of radiation and capecitabine in
nonoperable patients, local control of gross disease not
women with locally advanced breast cancer who had failed
resected at the time of surgery, and toxicity. Patients con-
first-line anthracycline-based neoadjuvant therapy, Gaui
senting to optional procedures will have a core biopsy per-
et al. studied the concomitant use of radiation therapy
formed before and at the conclusion of radiotherapy to be
and capecitabine, to determine the toxicity and efficacy of
assessed for cancer stem cells before and after radiother-
this regimen as a second-line neoadjuvant treatment.19
apy. We believe that advances in technology for radiation
Twenty-eight patients with inoperable locally advanced
therapy targeting and delivery make this the right time for
breast cancer refractory to first-line anthracycline-based
strategies exploring aggressive local/regional management
treatment were enrolled between January 2003 and May
in patients with progressive IBC. Although we anticipate
2004. Patients received radiation therapy (total dose 5000
preoperative radiation with capecitabine will provide
cGy) and concomitant capecitabine (850 mg/m2) twice
disease control and conversion to operability in some
daily for 14 days every 3 weeks. This treatment rendered
patients, patient selection and consent are critical before
23 (82%) of the 28 patients operable. The 5 remaining
embarking on any new therapy with significant potential
patients did not undergo surgery because of disease pro-
toxicity. These data will provide a baseline against which
gression. The median clinical tumor size decreased from
to compare new pipeline IBC targets. The prevalent basal
80 to 49 cm2. Microscopic residual disease was observed
phenotype of IBC makes it an ideal clinical model to
in 3 (13%) patients, and another patient achieved a com-
examine stem cell hypotheses, which we believe can help
plete pathologic response. The median number of
guide future trials to continue making incremental pro-
involved lymph nodes was 2, and treatment was well toler-
gress against this profoundly aggressive disease.
ated, with no grade 3 or 4 events. These results indicatethat second-line neoadjuvant treatment with radiation
therapy and capecitabine is feasible, well tolerated, and
Acceleration of radiotherapy regimens, giving increased
effective in patients with locally advanced breast cancer re-
dose in less time, has been an effective strategy against the
fractory to primary anthracycline-based treatment.
aggressive biology of IBC. Higher-risk patient subsets
have been identified that gain the greatest benefit from
Program and Clinic; the State of Texas Grant for Rare and
these aggressive strategies, but local control has not yet
Aggressive Cancers; and The University of Texas InstitutionalResearch Grants; KL2 RR024149 and R01CA138239-01.
been maximized for all patients, and safer, less toxicapproaches are needed. Greater understanding of the biol-ogy of radiation resistance in IBC is providing new
insights to guide the design of new trials with novel radio-
1. Singletary SE, Allred C, Ashley P, et al. Staging system for
breast cancer: revisions for the 6th edition of the AJCC
sensitizers to improve tumor control in IBC.
Cancer Staging Manual. Surg Clin North Am. 2003;83:803-819.
2. Wingo PA, Jamison PM, Young JL, Gargiullo P. Popula-
tion-based statistics for women diagnosed with inflammatory
breast cancer (United States). Cancer Causes Control. 2004;15:321-328.
To evaluate radiosensitivity, specified numbers of
3. Barker JL, Montague ED, Peters LJ. Clinical experience
cells derived from monolayer cultures were seeded into
with irradiation of inflammatory carcinoma of the breast
individual wells of a 6-well tissue culture plate (for 2D) or
with and without elective chemotherapy. Cancer. 1980;45:625-629.
ultralow attachment plates (for 3D). Cells from both
4. Fleming RY, Asmar L, Buzdar AU, et al. Effectiveness of
2D and 3D were exposed to increasing doses of radia-
mastectomy by response to induction chemotherapy for con-
tion (2, 4, or 6 Gy) 4 hours after plating. 2D plates
trol in inflammatory breast carcinoma. Ann Surg Oncol. 1997;4:452-461.
were incubated for 10 to 14 days, and colonies were stained
5. Panades M, Olivotto IA, Speers CH, et al. Evolving treat-
with crystal violet. For 3D, cells were incubated in mammo-
ment strategies for inflammatory breast cancer: a popula-
sphere media for 7 days, and spheres were stained with
tion-based survival analysis. J Clin Oncol. 2005;23:1941-1950.
3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bro-
6. Perez CA, Fields JN, Fracasso PM, et al. Management of
mide to improve visualization and counted using a
locally advanced carcinoma of the breast. II. Inflammatory
Gelcount colony counter (Oxford Optronix, Oxford,
carcinoma. Cancer. 1994;74(1 suppl):466-476.
7. Thoms WW Jr, McNeese MD, Fletcher GH, Buzdar AU,
UK). Clonogenic survival curves were generated using
Singletary SE, Oswald MJ. Multimodal treatment for
inflammatory breast cancer. Int J Radiat Oncol Biol Phys. 1989;17:739-745.
8. Bristol IJ, Woodward WA, Strom EA, et al. Locoregional
treatment outcomes after multimodality management of
SUM149 and SUM190 cells cultured under mammo-
inflammatory breast cancer. Int J Radiat Oncol Biol Phys.
sphere and adherent conditions were harvested with
10 mM ethylenediaminetetraacetic acid, centrifuged,
9. Kyndi M, Sorensen FB, Knudsen H, Overgaard M, Nielsen
HM, Overgaard J. Estrogen receptor, progesterone receptor,
and resuspended in phosphate-buffered saline (PBS)
HER-2, and response to postmastectomy radiotherapy in
(105 cells/mL). They were then incubated with fluorescein
high-risk breast cancer: the Danish Breast Cancer Coopera-
isothiocyanate (FITC)-conjugated CD44 and phycoery-
tive Group. J Clin Oncol. 2008;26:1419-1426.
10. Woodward WA, Buchholz TA. The role of locoregional
thrin (PE)-conjugated CD24 antibodies (BD Biosciences,
therapy in inflammatory breast cancer. Semin Oncol.
San Diego, Calif) for 30 minutes at concentrations recom-
mended by the manufacturer. Cells incubated in PBS,
11. Phillips TM, McBride WH, Pajonk F. The response of
CD24(-/low)/CD44þ breast cancer-initiating cells to radia-
FITC, or PE alone served as controls. Cell analysis for the
tion. J Natl Cancer Inst. 2006;98:1777-1785.
expression of CD44 and CD24 was performed using a
12. Woodward WA, Chen MS, Behbod F, Alfaro MP, Buch-
Beckman Coulter (Fullerton, Calif) machine, and the
holz TA, Rosen JM. WNT/beta-catenin mediates radiationresistance of mouse mammary progenitor cells. Proc Natl
data files were analyzed using FlowJo software (Treestar,
13. Xiao Y, Ye Y, Yearsley K, Jones S, Barsky SH. The lympho-
vascular embolus of inflammatory breast cancer expresses astem cell-like phenotype. Am J Pathol. 2008;173:561-574.
14. Greenbaum MP, Strom EA, Allen PK, et al. Low locore-
This supplement was sponsored by the Houston Affiliate of
gional recurrence rates in patients treated after 2000 with
Susan G. Komen for the Cure, the National Cancer Institute,
doxorubicin based chemotherapy, modified radical mastec-
and the State of Texas Rare and Aggressive Breast Cancer
tomy, and post-mastectomy radiation. Radiother Oncol. In
Research Program. The First International Inflammatory Breast
Cancer Conference was supported in part by GlaxoSmithKline,
15. Dontu G, Abdallah WM, Foley JM, et al. In vitro propaga-
Pfizer, Eli Lilly and Company, and Cardinal Health. Supported
tion and transcriptional profiling of human mammary stem/
by the Morgan Welch Inflammatory Breast Cancer Research
progenitor cells. Genes Dev. 2003;17:1253-1270.
Radiation and Inflammatory Breast Cancer/Woodward et al
16. Woodward WA, Bristow RG. Radiosensitivity of cancer-ini-
20. Dunst J, Debus J, Rudat V, et al. Neoadjuvant capecitabine
tiating cells and normal stem cells (or what the Heisenberg
combined with standard radiotherapy in patients with
uncertainly principle has to do with biology). Semin Radiat
locally advanced rectal cancer: mature results of a phase II
trial. Strahlenther Onkol. 2008;184:450-456.
17. Zhang M, Behbod F, Atkinson RL, et al. Identification of
21. Krishnan S, Janjan NA, Skibber JM, et al. Phase II study of
tumor-initiating cells in a p53-null mouse model of breast
capecitabine (Xeloda) and concomitant boost radiotherapy
cancer. Cancer Res. 2008;68:4674-4682.
in patients with locally advanced rectal cancer. Int J Radiat
18. Al-Hajj M, Wicha MS, Benito-Hernandez A, Morrison SJ,
Clarke MF. Prospective identification of tumorigenic breast
22. Perkins GH, Middleton LP, Tran R, et al. Concurrent che-
cancer cells. Proc Natl Acad Sci U S A. 2003;100:3983-3988.
moradiation with capecitabine achieves meritable response
19. Gaui MF, Amorim G, Arcuri RA, et al. A phase II study of
and local control for inoperable and recurrent neoadjuvant
second-line neoadjuvant chemotherapy with capecitabine
chemotherapy refractory breast cancer. Paper presented at:
and radiation therapy for anthracycline-resistant locally
San Antonio Breast Cancer Symposium; December 13-16,
advanced breast cancer. Am J Clin Oncol. 2007;30:78-81.
Prayer before drinking wine on Purim – Say before every cup! I hereby connect myself through drinking this wine, on this Purim day to all the true Tzaddikimin our generation, and to all the true Tzaddikim of previous generations, and to Mordechai andEsther, and in particular to our holy Rebbe, Tzaddik, a flowing brook of wisdom, Rebbe Nach-man ben Faige of Breslev, he should be a merit for us
Use of genomic technologies and isotonic dose• response modeling in the development of a biochemical marker of effect for pyrethroid insecticides University of North Carolina at Chapel Hill Pyrethroids are pesticides that disrupt nervous system function in both target (insects) and non• target species. These compounds exert their neurotoxic effect through prolongation of sodium curre
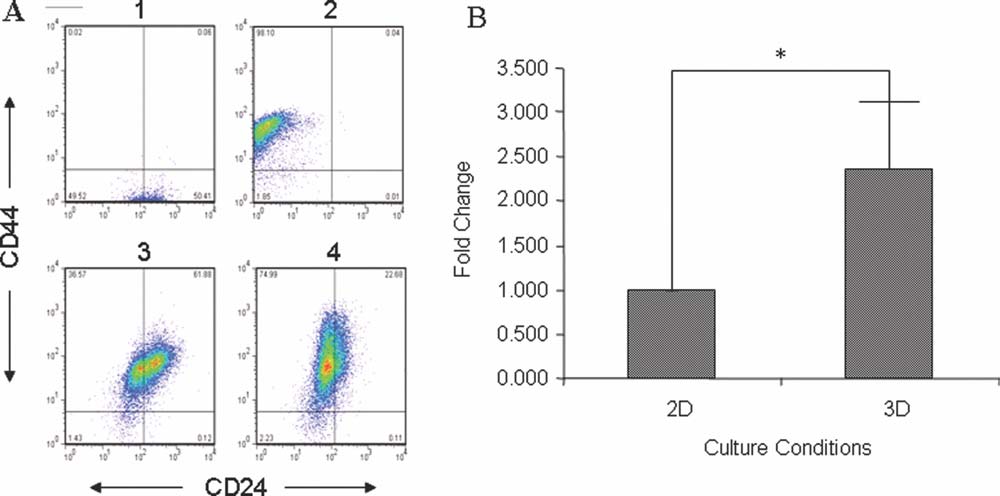 Figure 1. Flow cytometric analysis of expression of CD24 and CD44 in SUM149 inflammatory breast cancer (IBC) cells is shown.
Figure 1. Flow cytometric analysis of expression of CD24 and CD44 in SUM149 inflammatory breast cancer (IBC) cells is shown.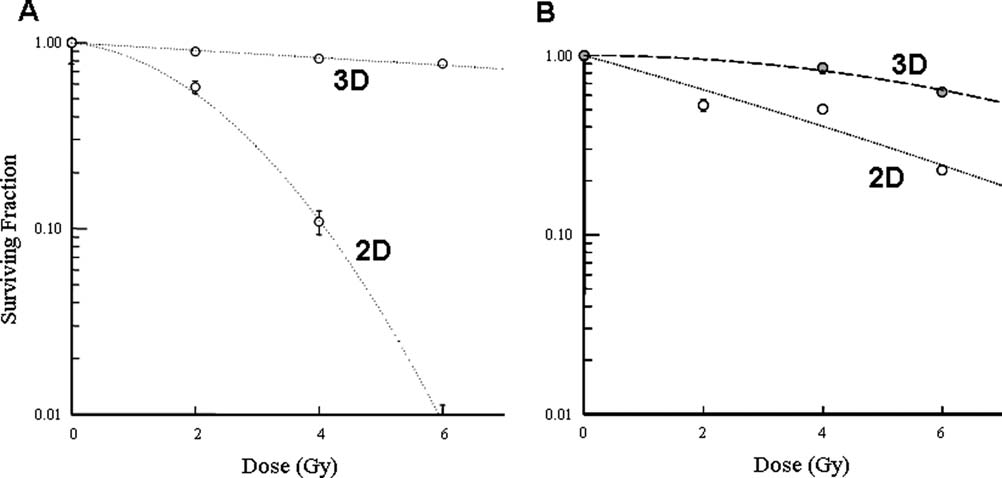 Radiation and Inflammatory Breast Cancer/Woodward et al
Figure 2. Tumor-initiating cells from inflammatory breast cancer (IBC) cell lines are more resistant to radiation than monolayer(2-dimensional [2D]) cells. Clonogenic survival assay of IBC cells derived from (A) SUM149 and (B) SUM190 cultured under 2D ormammosphere (3D) cultures is shown. Cells in 3D are more resistant to radiation than cells grown in 2D. Cells were grown in 2Dor 3D culture conditions and irradiated with single, increasing doses (0, 2, 4, 6 gray [Gy]) of radiation.
Radiation and Inflammatory Breast Cancer/Woodward et al
Figure 2. Tumor-initiating cells from inflammatory breast cancer (IBC) cell lines are more resistant to radiation than monolayer(2-dimensional [2D]) cells. Clonogenic survival assay of IBC cells derived from (A) SUM149 and (B) SUM190 cultured under 2D ormammosphere (3D) cultures is shown. Cells in 3D are more resistant to radiation than cells grown in 2D. Cells were grown in 2Dor 3D culture conditions and irradiated with single, increasing doses (0, 2, 4, 6 gray [Gy]) of radiation.