Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Guerbet.com
A 59-year-old woman was admitted for rapid health degradation, with abdominal pain, icterus and ascites. She was known for a two years long-standing breast cancer aggra-vated progressively by multi-organ metastases. The patient was treated by hormonal therapy (Tamoxifen followed by Exemestane) and chemotherapy (5-Fluorouracil – Epirubucin – Cyclophosphamide then Cisplatine – 5-Fluorouracil). Contrast-enhanced CT scan of the thorax and the abdomen were performed (Fig. 2) and compared to previous CT scans (Fig. 1).
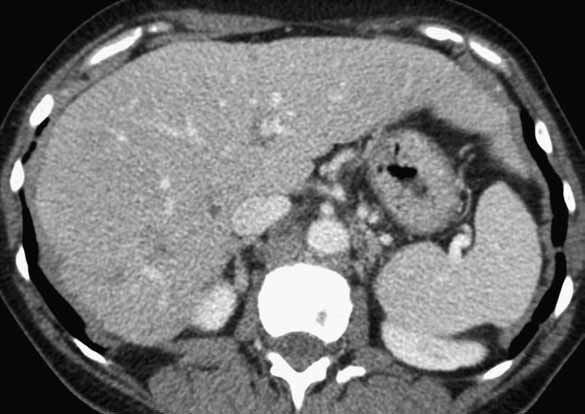
Figure 1: Axial contrast-enhanced CT scan. Section at the level of the liver (January 2011). In January 2011, CT showed a normal sized and smooth liver. Small metastases are already observed in the right hepatic lobe. No ascites or portal hypertension is present.
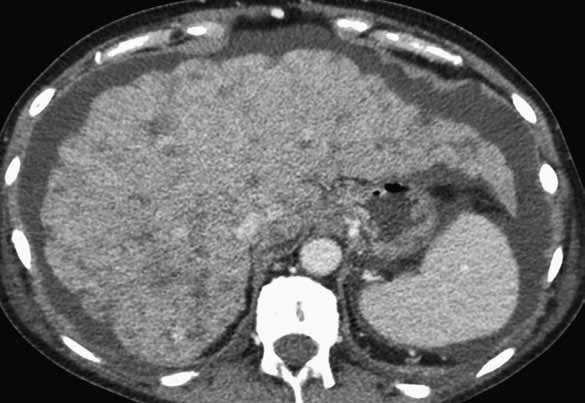
Figure 2: Axial contrast-enhanced CT scan of upper abdomen (August 2011).
Fig. 2a: Section at the level of the liver. Highly dysmorphic and heterogeneous liver with capsular retractions, lobulated pattern and multiples hypodense lesions, complicated by ascites.
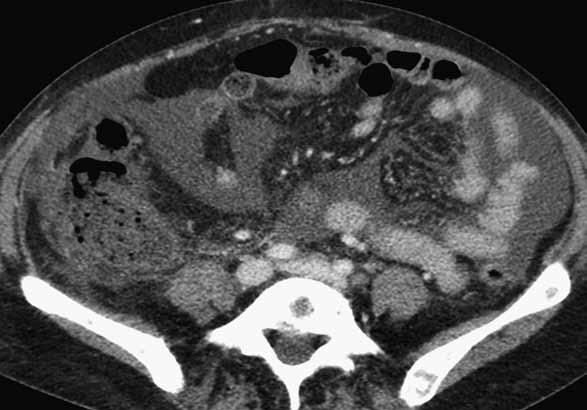
Fig. 2b: Section at mid-abdominal level. Features of portal hypertension are demonstrated with ascites, enlarged mesenteric veins and congested wall of the right colon. Notice also the presence of multiple bone metastases.
Cliniques Universitaires St-Luc, Catholic University of Louvain, Brussels, Belgium
e-mail address for correspondence: [email protected]
Based on the radiological findings and the clinical history, the diagnosis of hepar loba-tum carcinomatosum was made.
Hepar lobatum carcinomatosum (HLC) is an acquired non-cirrhotic liver dysmorphy associated with liver
metastases of carcinoma, most often breast carcinoma.
Hepar lobatum, characterized by a coarsely nodular lobulated liver parenchyma by deeply grooved scars,
was first described in association with tertiary syphilis. Since 1924, this entity was occasionally reported
in association with carcinomatous liver metastases and thus renamed hepar lobatum carcinomatosum.
At pathology, diffuse metastatic involvement of the liver is observed in HLC, characterized by the pres-
ence of fibrous septa originating from the organ surface and running deep into the parenchyma. These
septa contain scattered metastatic cells. HLC can be observed independently of neoplasic progression
or apparent regression, and independently of chemotherapy of the metastatic carcinoma.
On imaging, HLC must be suggested in case of rapid (months) dysmorphic transformation of a previously
smooth and normal sized liver into a liver with capsular retractions and lobulated pattern, in the absence
of etiologic factor for cirrhosis (hepatitis B or C, alcohol or drug consumption, hemochromatosis,.).
Metastatic liver lesions can be observed or not. MRI demonstrates scarring and progressive fibrosis of
the liver, demonstrated by late parenchymal enhancement after IV Gadolinium injection.
The oncologic history is usually already known, but HLC can occasionally be the initial manifestation of
The physiopathology of HLC remains controversial. First authors hypothesized a desmoplastic stromal
response in reaction of metastatic cells invasion. Later, it has been proposed that HCL could be a certain
form of healing and scarring after tumor regression, since several cases have been reported following
chemotherapy. More recently, it has been suggested that vascular injuries could play a major role in HCL
development: firstly, direct diffuse invasion and obstruction of intra-hepatic portal and/or hepatic
venous branches has been reported in most of cases. This peripheral vascular invasion can be respon-
sible for a congestive effect on liver, leading to its gradual shrinkage with typical veinocentric distribu-
tion of fibrosis and development of portal hypertension. Secondly, chemotherapy could be an additional
In summary, HLC could result from the combination between an important stromal reaction to carcino-
matous cells associated to intrahepatic vascular tumoral obstruction, potentially aggravated by chemo-
HLC has a poor prognosis, even in case of apparent tumoral regression after chemotherapy.
Liver, metastases – hepar lobatum carcinomatosum – liver, CT scan
1. Cervoni JP, Dobrin A, Sailley N, et al. Hepar lobatum carcinomatosum: A rare cause of portal hyper-
tension complicating hepatic metastases in breast cancer. Gastroenterol Clin Biol. 2008; 32: 740-744.
2. Honma K. Hepar lobatum carcinomatosum due to metastatic breast carcinoma. Virchows Arch A
Pathol Anat Histopathol 1987; 410: 465-469. PMID: 3105165
3. Graber I, Dumortier J, Poncet G, et al. Hepar lobatum carcinomatosum revealing an occult metastatic
lobular carcinoma of the breast. Ann Diagn Pathol 2010; 14: 438-442. PMID: 21074693
4. Teke Z, Nessar G, Kiremitci S, et al. Hepar lobatum carcinomatosum associated with metastatic rectal
carcinoma: an unusual cause of liver dysmorphy. Med Princ Pract. 2011; 20: 93-96. PMID: 21160223
Cliniques Universitaires St-Luc, Catholic University of Louvain, Brussels, Belgium
e-mail address for correspondence: [email protected]
You can make the most of your pharmacy benefit plan and control your prescription medication costs by using this Preferred Medication List. Be sure to share this list with your doctor to select cost-effective medications that are clinical y appropriate to treat your condition or maintain your health. This Preferred Medication List (PML) was developed by • Therapeutic categories are listed alp
The Medicalization of Society Over the past century an increasing number of human problems have come into the jurisdiction of the medical profession. This process has been termed the medicalization of society. We will examine core theoretical and empirical texts that examine this issue, especially the origins and consequences of medicalization. While we will read books and articles from sever
 A 59-year-old woman was admitted for rapid health degradation, with abdominal pain, icterus and ascites. She was known for a two years long-standing breast cancer aggra-vated progressively by multi-organ metastases. The patient was treated by hormonal therapy (Tamoxifen followed by Exemestane) and chemotherapy (5-Fluorouracil – Epirubucin – Cyclophosphamide then Cisplatine – 5-Fluorouracil).
A 59-year-old woman was admitted for rapid health degradation, with abdominal pain, icterus and ascites. She was known for a two years long-standing breast cancer aggra-vated progressively by multi-organ metastases. The patient was treated by hormonal therapy (Tamoxifen followed by Exemestane) and chemotherapy (5-Fluorouracil – Epirubucin – Cyclophosphamide then Cisplatine – 5-Fluorouracil). Based on the radiological findings and the clinical history, the diagnosis of hepar loba-tum carcinomatosum was made.
Based on the radiological findings and the clinical history, the diagnosis of hepar loba-tum carcinomatosum was made.