Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Ftd.med.upenn.edu
of specific diagnostic criteria based on an independent
RESEARCH LETTER
review of the semistructured history, detailed mental sta-tus examination, and complete neurological examina-tion. These patients and their legal representatives par-
Longitudinal Cortical Atrophy
ticipated in an informed consent procedure approved bythe institutional review board at the University of Penn-
in Amyotrophic Lateral Sclerosis
sylvania. The age-matched (PϽ.61) patients (mean [SD]
With Frontotemporal Dementia
age, 61.3 [6.1] years) were right-handed, high school-
F rontotemporaldementia(FTD)withamyotro- educated(mean[SD]education,17.5[1.9]years),na-
phic lateral sclerosis (ALS) presents with im-
tive English speakers with a mean (SD) Mini-Mental State
paired language or behavior and declining mo-
Examination score at the first examination of 27.0 (3.2).
tor function. Frontotemporal lobar degeneration with
The second evaluation was conducted a mean (SD) of 5.3
ubiquinated transactivating responsive sequence DNA-
(0.5) months after the first evaluation, and the mean (SD)
binding protein (TDP-43) inclusions is found postmor-
score at the second evaluation was 21.3 (8.5).
tem in the affected brain areas of patients with ALS, FTD/
Imaging. Baseline and follow-up image acquisitions
ALS, and many patients with FTD.1 Prior magnetic
(Trio 3.0T MRI scanner; Siemens, Munich, Germany) be-
resonance imaging (MRI) observations revealed cross-
gan with a sagittal T1-weighted localizer. A T1 struc-
sectional atrophy in the motor and/or premotor cortices
tural axial image was acquired with a repetition time of
of patients with FTD/ALS,2 while a longitudinal study
1620 milliseconds; TE echo time, 3 seconds; slice thick-
using diffusion tensor imaging revealed corticospinal tract
ness, 1 mm; in-plane resolution, 0.9766 mmϫ0.9766 mm;
changes.3 We used high-resolution diffeomorphic im-
and field of view, 256 ϫ256ϫ192 voxels.
age normalization4,5 and serial MRI to provide the first
Imaging Normalization and Longitudinal Atrophy
assessment of longitudinal cortical atrophy in patients
Assessment. We use a longitudinal extension4 of large de-
formation tensor-based morphometry (LDTBM)5 in thisstudy. This framework first generates an unbiased intra-
Methods. Subjects. We contrasted 4 elderly controls with
subject measurement of atrophy from each subject’s base-
4 patients with FTD/ALS, performed by an experienced
line and follow-up image.4 One high-resolution voxel-
neurologist (M.G.) at the University of Pennsylvania De-
wise map of annual atrophy for each individual is
partment of Neurology. Two trained reviewers (M.G. and
transferred to a local template space that allows statistical
L.M.) of a consensus committee confirmed the presence
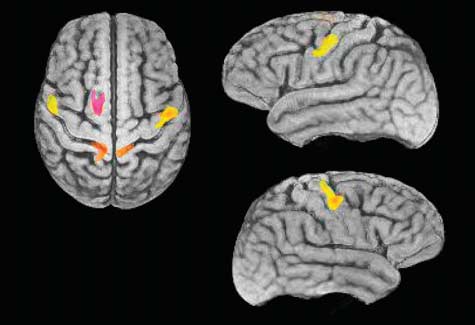
contrast of subject and control longitudinal change via thet test, computed within an explicit gray matter mask. Results. We rendered cortical regions with significant an- nual atrophy due to FTD/ALS on the local template in the Figure. Significant effects occur in the premotor cor- tex, primary motor cortex, and parietal lobe bilaterally in Brodmann areas (BA) 4, 6, and 7. The average annual cortical atrophy over significant voxels in FTD/ALS on the right and left is 8.5% and 7.6%, respectively, in BA4; 8.1% and 5.9% in BA6; and 3.6% and 2.2% in BA7. For all cortices in FTD/ALS, the atrophy rate was 1.0% per
year; in elderly controls, 0.25% per year. The local atro-
phy rate did not correlate with global brain atrophy; the
age and global brain atrophy rates did not correlate. Comment. We found significant differences in longitu- Figure. The significant areas of annual atrophy in our amyotrophic lateral
dinal cortical atrophy in motor and premotor areas in pa-
sclerosis (ALS) population are highlighted and color-coded by
tients with clinical features of both ALS and FTD. Amyo-
neuroanatomical area on the cortex of a population-specific template. Atrophy was measured by a fine-grained quantitative structural analysis
trophic lateral sclerosis cooccurs with FTD in 5% to 10%
based on diffeomorphic image normalization. Such methods quantify
of cases. This is owing, in part, to the presence of ubiq-
structure in the spirit of voxel-based morphometry, but with higher anatomic
uitinated TDP-43 underlying both FTD and ALS.6 Pre-
fidelity and sensitivity.4,5 Significance is defined as a voxelwise falsediscovery rate–corrected P value of .05 with contiguous gray matter voxel
sumably, regional motor and premotor cortical atrophy
clusters larger than 500 voxels. These areas indicate regions of cortical gray
reflect the motor and cognitive changes, respectively, that
matter undergoing annual atrophy that are consistently greater in ALS than
are characteristic of this condition. Additional study is
in the age- and education-matched elderly control population. In contrast, across-sectional morphometric comparison of the elderly and motor neuron
needed to establish whether there are clinically observ-
degeneration cortical volumes in this cohort produced no significant effects.
able changes corresponding to these parietal changes.
(REPRINTED) ARCH NEUROL / VOL 66 (NO. 1), JAN 2009
2009 American Medical Association. All rights reserved. Downloaded From: http://archneur.jamanetwork.com/ by a University of Pennsylvania User on 03/14/2013
Cortical atrophy is thought to be difficult to detect in
ease (MJD). We would like to raise some concerns re-
ALS because the relatively rapid rate of clinical progres-
garding the authors’ interpretation of the findings.
sion minimizes the opportunity for noticeable cortical at-
First, Franc¸a and colleagues proposed that altered ex-
rophy to emerge and motor disease limits the practical
citatory inputs from the corticospinal fibers rather than
limitation of follow-up assessments. This may be the first
the peripheral motor axonal changes might be respon-
demonstration of longitudinal cortical atrophy in FTD/
sible for muscle cramps in MJD. Muscle cramps and fas-
ALS because normalization with LDTBM reduces re-
ciculations arise from spontaneous motor unit activities
sidual intersubject variance in neuroanatomy while re-
frequently associated with lower motor neuron disor-
taining sensitivity to intrasubject effects, augmenting
ders, and ectopic firing usually originates from the dis-
detection power in neuromorphometry.
tal motor axons, especially the intramuscular nerve ter-minals.3 We have shown that muscle cramp severity
correlates with an increased index of peripheral axonal
excitability, suggesting that cramps in MJD are associ-
ated with underlying peripheral axonal loss and result-
ing collateral sprouting by the surviving neurons. We con-
sider muscle cramp a symptom of motor nerve sproutingbut not of neuronal degeneration. In our experience, dis-
Correspondence: Dr Avants, 3600 Market St, Ste 360,
abling muscle cramps in patients with MJD are most
Philadelphia, PA 19104 ([email protected]).
prominent during the early stages of the disease and then
Author Contributions: Dr Grossman had full access to
gradually disappear with the progression of amyotro-
all of the data in the study and takes responsibility for
phy.2 This phenomenon would possibly be associated with
the integrity of the data and the accuracy of the data analy-
the high ability of sprouting in the early stages of dis-
sis. Study concept and design: Avants and Grossman. Ac-
ease. Therefore, the subgroup of patients without cramps
quisition of data: Khan, McCluskey, and Elman. Analysis
might include patients in the early and advanced stages
and interpretation of data: Avants, Khan, and Grossman.
of MJD. We believe that this fact accounts for the seem-
Drafting of the manuscript: Avants, Khan, and Grossman.
ingly insignificant difference in the neurophysiological
Critical revision of the manuscript for important intellec-
parameters between groups with and without cramps. tual content: Avants, McCluskey, Elman, and Grossman.
Second, Franc¸a and colleagues showed that the cramp
Statistical analysis: Avants. Obtained funding: Avants. Ad-
in MJD was effectively treated with carbamazepine. In
ministrative, technical, and material support: Khan. Study
our previous study,2 patients with MJD who had dis-
abling muscle cramps benefited from mexiletine hydro-
Financial Disclosures: None reported.
chloride treatment, and nerve excitability testing sug-
Funding/Support: This study was supported in part by
gested that increases in persistent sodium currents in the
grants AG17586, AG15116, NS44266, and NS53488 from
peripheral motor axons lead to axonal hyperexcitabil-
ity. Hence, the authors’ use of sodium channel blockers
1. Forman MS, Farmer J, Johnson JK, et al. Frontotemporal dementia: clinico-
for muscle cramps in MJD appears to be a rational course.
pathological correlations. Ann Neurol. 2006;59(6):952-962.
Carbamazepine is an effective and inexpensive antiepi-
2. Chang JL, Lomen-Hoerth C, Murphy J, et al. A voxel-based morphometry study
of patterns of brain atrophy in ALS and ALS/FTLD. Neurology. 2005;65(1):
leptic drug, but serious adverse effects are not rare. There-
fore, further studies will be required to investigate which
3. Blain C, Williams V, Johnston C, et al. A longitudinal study of diffusion ten-
sodium channel blocker is the most appropriate treat-
sor MRI in ALS. Amyotrophic Lateral Sclerosis. 2007;8(6):348-355.
4. Avants B, Anderson C, Grossman M, Gee JC. Spatiotemporal normalization
ment for muscle cramps in patients with MJD.
for longitudinal analysis of gray matter atrophy in frontotemporal dementia. Med Image Comput Comput Assist Interv Int Conf Med Image Comput ComputAssist Interv. 2007;10(pt 2):303-310.
5. Kim J, Avants B, Patel S, et al. Structural consequences of diffuse traumatic
brain injury: a large deformation tensor-based morphometry study. Neuroimage. 2008;39(3):1014-1026. Correspondence: Dr Kanai, Department of Neurology,
6. Neumann M, Sampathu DM, Kwong LK, et al. Ubiquitinated TDP-43 in fron-
Graduate School of Medicine, Chiba University, 1-8-1 Ino-
totemporal lobar degeneration and amyotrophic lateral sclerosis. Science. 2006;
hana, Chuo-ku, Chiba 260-8670, Japan (VZR03355@nifty
.ne.jp). Financial Disclosure: None reported. COMMENTS AND OPINIONS
1. Franc¸a MC Jr, D’Abreu A, Nucci A, Lopes-Cendes I. Muscle excitability ab-
normalities in Machado-Joseph disease. Arch Neurol. 2008;65(4):525-529.
2. Kanai K, Kuwabara S, Arai K, Sung JY, Ogawara K, Hattori T. Muscle cramp
in Machado-Joseph disease: altered motor axonal excitability properties andmexiletine treatment. Brain. 2003;126(pt 4):965-973. Motor Nerve Hyperexcitability and
3. Miller TM, Layzer RB. Muscle cramps. Muscle Nerve. 2005;32(4):431-442. Muscle Cramps in Machado-Joseph Disease In reply W ereadthearticlebyFranc¸aetal1withgreat WeareverypleasedwiththecommentsraisedbyKanaiand
interest. We thank them for confirming our
Kuwabara regarding our study. Our findings in the seriesof Brazilian patients with MJD indeed confirm previous re-
quency of and disability associated with muscle cramps2
sults reported by Kanai et al,1 indicating that muscle cramps
in a larger sample of patients with Machado-Joseph dis-
are a frequent and disabling manifestation of the disease.
(REPRINTED) ARCH NEUROL / VOL 66 (NO. 1), JAN 2009
2009 American Medical Association. All rights reserved. Downloaded From: http://archneur.jamanetwork.com/ by a University of Pennsylvania User on 03/14/2013
LISTE DES MEMOIRES SOUTENUS PAR LES RESIDENTS ET INTERNES DE MEDECINE GENERALE Directeur de mémoire D'EPOUSE Titre du Mémoire soutenance MG dans le domaine médico-L'impact des loisirs sur l'audition préventionVisite du médecin généraliste maintien à domicileRôle du médecin dans aiguë en MGMaintien à domicile difficile des personnes âgées à partir de 2 de la m
 of specific diagnostic criteria based on an independent
RESEARCH LETTER
of specific diagnostic criteria based on an independent
RESEARCH LETTER