Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Journal of Pediatric Surgery (2012) 47, 2279–2284
Transabdominal electrical stimulation increases colonicpropagating pressure waves in paediatric slowtransit constipation☆,☆☆,★
Melanie C.C. Clarke a, Anthony G. Catto-Smith a,b,c, Sebastian K. King a,c,Phil G. Dinning d, Ian J. Cook d, Janet W. Chase a, Susan M. Gibb a,b,Val J. Robertson e, Di Simpson b, John M. Hutson b,c, Bridget R. Southwell a,c,⁎
aMurdoch Childrens Research Institute, Melbourne, AustraliabRoyal Children's Hospital, Melbourne, AustraliacDepartment of Paediatrics, University of Melbourne, AustraliadSt George Hospital, and Department of Medicine, University of New South Wales, Sydney, NSWeUniversity of Newcastle, Australia
Received 31 August 2012; accepted 1 September 2012
Background and aims: In slow-transit constipation (STC) pancolonic manometry shows significantly
reduced antegrade propagating sequences (PS) and no response to physiological stimuli. This study
aimed to determine whether transcutaneous electrical stimulation using interferential current (IFC)
applied to the abdomen increased colonic PS in STC children. Methods: Eight children (8–18 years) with confirmed STC had 24-h colonic manometry using awater-perfused, 8-channel catheter with 7.5 cm sidehole distance introduced via appendix stomas. They then received 12 sessions (20 min/3× per week) of IFC stimulation (2 paraspinal and 2abdominal electrodes), applied at a comfortable intensity (b40 mA, carrier frequency 4 kHz,varying beat frequency 80–150 Hz). Colonic manometry was repeated 2 (n=6) and 7 (n=2) monthsafter IFC. Results: IFC significantly increased frequency of total PS/24 h (mean ±SEM, pre 78±34 vs post210± 62, p=0.008, n=7), antegrade PS/24 h (43± 16 vs 112± 20, p=0.01) and high amplitude PS(HAPS/24 h, 5± 2:10± 3, p=0.04), with amplitude, velocity, or propagating distance unchanged. Therewas increased activity on waking and 4/8 ceased using antegrade continence enemas.
☆ Authors have no financial conflict of interest to disclose.
☆☆ Funding source: National Health and Medical Research Council, Australia (Project Grants 384434, 546432, Senior Research Fellowship 436916-BRS),
Murdoch Childrens Research Institute Theme Investment Grants, and supported by the Victorian Government's Operational Infrastructure Support Program.
★ Ethics approval: Royal Children's Hospital Ethics Committee (HRC 23040 C), Clinical Trial Registration ANZCTR: ACTRN12610000418077.
⁎ Corresponding author. Gut Motility Laboratory, Surgical Research Group, Murdoch Childrens Research Institute, Royal Children's Hospital, Parkville,
Victoria, Australia, 3052. Tel.: +61 3 9345 5069.
0022-3468/$ – see front matter 2012 Elsevier Inc. All rights reserved.
Conclusions and inferences: Transcutaneous IFC increased colonic PS frequency in STC children witheffects lasting 2–7 months. IFC may provide a treatment for children with treatment-resistant STC. 2012 Elsevier Inc. All rights reserved.
Many children with chronic constipation respond to
medical therapy and behavioural modification programmes,but 1/3 remain constipated into adulthood . Constipation
Briefly, physiotherapists were provided with IFC
may be caused by slow colon transit (slow-transit constipa-
machines (Vectorsurge 5 VS470, Metron Medical, Carrum
tion, STC), diagnosed via radio-nuclear or sitz (plastic)
Downs, Victoria, Australia) that delivered two channels of
marker colon transit studies In STC, soiling and fecal
alternating current. One at a fixed frequency (4 kHz),
impaction have significant social and emotional conse-
whilst the other varied from 4080 to 4150 Hz, producing a
quences for the child and family, resulting in a low quality of
varying beat frequency of 80 to 150 Hz. The current
(b40 mA) was applied via 4 self-adhesive conducting
Children with STC can be managed by antegrade
electrodes (40 mm × 40 mm, Verity Medical Ltd, Hamp-
continence enemas (ACE) , and we have previously
shire, England),with 2 paraspinal (T9-L2), and the paired
reported the analysis of colonic motor activity performed by
electrodes positioned diagonally opposite on the anterior
inserting the manometry catheter via the appendix stoma
abdominal wall below the costal margin . Current was
. Significant abnormalities in colonic motor function
applied just at the sensory level and sub-motor intensity so
were identified, including reduced frequency of antegrade
children felt no more than low sensory stimulation and no
propagating sequences (PS) and lack of response to meals
skeletal muscle contractions occurred. IFC stimulation was
given for 20 min, ×3/week for 4 weeks.
Transcutaneous electrical stimulation using interferential
current (IFC) has been used for pain management and
urinary incontinence, with diarrhoea reported as a sideeffect . IFC increased defecation frequency inchildren with chronic constipation and reduced
Eight children had 24-h colonic manometry immediately
colonic transit times in STC . Symptom improve-
before electrical stimulation and 2 months (n=6, 5 male, 9–
ment lasted 3–6 months in 1/3 and more than 2 years in 1/3
19 years) or 7 months (n=2, 1 male, 16–18years) after
of patients . The aim of this study was to determine
completing stimulation. Patients ceased washouts 5 days
the effects of IFC upon colonic PSs. Specifically, we
before and during the manometry. Manometry was performed
hypothesised that IFC increases the frequency of PS in
as previously described Briefly, an 8-channel multi-lumen
catheter with 7.5 cm sidehole spacing, was inserted via theappendix stoma and advanced anally with bisacodyl infusion(2.5 ml of 0.5 mg/ml solution). The catheter position wasestablished by fluoroscopy. Water was perfused at 0.25 ml/
min. Polygram software (Medtronic Australasia, Gladesville,NSW, Australia) was used for recording, commencing 24 h
Children (n = 62) with STC were recruited during a larger
after bisacodyl with children remaining in bed for 24 h.
randomised control trial (Ethics: HEC 23040C) .
They drank water and ate a meal of 17% protein, 34%
Thirteen of these children had appendix stomas, and 8/13
carbohydrate and 48% fat, with 1255 kJ for breakfast, 4184 kJ
volunteered for colonic manometry forming the cohort of
for lunch and 4184 kJ for dinner. They completed an event
diary recording eating, postural changes, sleep/waking, urine
All 8 children had N2 years chronic constipation that had
and defecation, abdominal sensation and flatus. After 24 h, 20
not responded to medical therapies (diet, laxatives, behaviour
min of electrical stimulation was applied.
modification). STC was diagnosed by radionuclear transit
Colonic motility studies were examined and analysed
studies (defined by retention of radioisotope in the
visually, as previously described to identify antegrade
ascending/transverse colon) performed within the previous
PS, retrograde PS and high amplitude PS, the latter defined
year . Patients had existing appendix stomas placed more
as N116 mmHg in 3 adjacent channels (shown as ‘extent’
than 6 months before the study. All had long-standing
in Frequency, amplitude and velocity of PS and
constipation (6–19 years of symptoms). Half had symptoms
distance travelled were compared before and after
since birth. Most had soiling but only 2 had daily soiling. For
stimulation for each patient (paired t-test). Linked PSs
management, they performed antegrade continence enemas
were identified. Sequential PSs were defined as being
to wash out their colons every second day and recorded 3–4
‘regionally-linked’ if they started at different side-holes,
were in the same direction and had overlapping side-hole
Frequency, extent and velocity of propagating sequences.
D. Frequency of total colonic propagating sequences
activity If 3 or more regionally-linked PSs occurred
sequentially, this was defined as a ‘colonic complex’. Waking and postprandial responses were analysed using
Samples were tested for normality and then compared pre
and post TES using students t-test. P b0.05 was considered
statistically significant. For one patient, recording stopped
initiation moved from the splenic flexure before stimulation,
during the 2nd session and this patient was not included
to the rectosigmoid after stimulation. Pre-treatment 4/5
patients had antegrade and 2/5 had retrograde coloniccomplexes, whilst post-treatment all 5 had antegrade and 3/5 had retrograde colonic complexes. There was no change in
percent of antegrade linked-sequences (pre-treatment 65% ±8%, mean ± SEM, post-treatment 56% ± 4.5%), but unexpect-edly, there was a significant decrease in retrograde linked-
Children had colonic manometry before and 2 months
sequences (61% ± 4.5%, 33% ± 9.8%, p = 0.04 t-test).
(n = 6) or 7 months (n = 2) after 1 month of IFC stimulation.
Data on responses to meal and waking were available for
Data from one time period (9 am to 5 pm) from one child
4/6 patients given the second manometry 2 months after IFC
2 months after stimulation were lost, and this child is not
and 2/2 patients 7 months after IFC. None of these 6 patients
had an increase in high amplitude PS activity on waking
Following stimulation 5 patients had an increase in
before stimulation. Two months post-stimulation, there was
antegrade, high amplitude and retrograde PS, with the
an increase in the number of subjects showing a waking
antegrade:retrograde PS ratio becoming greater than 1.0 (1.4
response (0/4 and 0/2 pre, 3/4 and 1/2 post). At 2 months
to 4.6, One patient (#5) had no change in antegrade
post-stimulation, there was also a small increase in patients
or high amplitude PS, a doubling in retrograde PS and
with an increase in high amplitude PS after a meal (3 meals, 4
reduction in antegrade:retrograde PS ratio. Another patient
subjects, 3/12 pre, 6/12 post). There was an increase in total
(#6) had a three-fold increase in antegrade and retrograde PS
motility index but no greater response after a meal in the 2
but a reduction (halving) in high amplitude PS. Results were
patients at 7 months post-treatment.
similar for patients at 2 or 7 months post-stimulation.
All patients were using ACE to washout the colon every
shows the change in frequency of PS in 7 children, 2 months
2–3 days for management. There was no difference in the
after stimulation (n = 5) and 7 months after stimulation (n = 2).
number of defecations/week in the pre-treatment (mean±
In the combined group (n = 7), there was a significant
SEM, 3.6±0.6), treatment (3.1±0.4), 1st month post treatment
increase in frequency of antegrade, high amplitude and total
(4.6±0.5) or 2nd month post treatment (3.3±0.4). However,
PS, with a non-significant increase in frequency of retrograde
2/6 patients were able to defecate without the use of antegrade
PS (). Increases were into the normal range
enemas 2 months after stimulation as were the 2 patients with
If data for two months after stimulation were assessed
7 month follow up. Continuing to defecate without needing
separately, there was still a significant increase in the
washouts suggests their constipation symptoms were gone.
frequency of total PS (/24 h mean ± SEM, pre 89 ± 47: post221 ± 80, p = 0.03, n = 5), antegrade PS (/24 h, 49 ± 22:115 ±18, p = 0.03) and high amplitude PS (/24 h, 5 ± 3:11 ± 3, p =0.06), compared with activity before stimulation (paired
t-test). There was a non-significant increase in retrograde PS(/24 h, 40 ± 25 pre, 107 ± 70, p = 0.22). There was no apparent
In a long-term follow-up of patients in an RCT of IFC to
change in velocity or propagating distance.
treat paediatric STC, 1/3 of patients had no improvement, 1/3
The most common site of initiation of propagation of
of the patients had improvement that lasted more than 2 years
antegrade PS was the cecum, both before and after
and 1/3 had improvement lasting 3–6 months . In this
stimulation. For retrograde PS, the most common site of
study we examined a subset of these patients and demon-
Frequency of propagating sequences (PS). (A) Total, antegrade (Ant), high amplitude (HAPS) and retrograde (Ret) PS. Mean (SEM)
values of all 7 patients. (B) HAPS values of all 7 patients.
strated that transcutaneous electrical stimulation using IFC
patients with daily stimulation for more than 2 months
increased frequency of colonic PS in 5/7 STC children. There
support that symptoms continue to improve with more
was also a 3-fold increase in high amplitude PS frequency.
stimulation Patients are accustomed to using laxatives or
Four of 8 patients stopped using ACE, as soiling stopped. The
ACE, and graded removal of these treatments may need to be
increased activity persisted for 7 months in the 2 patients who
planned and measured as specific outcomes.
were followed for the longer period.
Unfortunately the numbers studied are small, as each
Colonic PS and high amplitude PS are temporally
study requires the family and child to spend 3 days in the
associated with both defecation and luminal transit in
hospital and few are able to do this twice. Because of the
healthy controls. More frequent high amplitude PS after
difficulties of doing this assessment, we did not attempt an
morning waking or a high calorie meal can also be used as a
RCT. We cannot discount that these changes in bowel
measure of a “normal’ colonic response to physiological
activity could occur as a placebo or due to time. As we think
stimuli Adults and children with STC have an absent or
it would be very difficult to perform an RCT, large animal
diminished response to such stimuli An absent colonic
studies may be necessary to perform an RCT.
response has been reported by some to be an indicator of an
Children with STC have reduced antegrade PS. Transcu-
intrinsic neuropathy/mesenchymopathy Therefore as
taneous IFC 3-times a week for 1 month increased the
the majority of our patients demonstrated an increased
frequency of colonic PS 3–5 fold in most of the children and
frequency of PS and high amplitude PS after treatment with
increased colonic motor activity on waking and after meals.
IFC, these data are likely to be of clinical significance.
The effects persisted 2–7 months after stimulation. Further
The mechanism of action of IFC remains unclear. With
studies on larger numbers of patients are warranted to
the electrode positions used, the current could affect local
determine if IFC can provide a treatment for children with
sensory and motor nerves in the skin, spinal nerves
(sensory and motor, T9 to L2), sympathetic (thoraco-lumbar) and parasympathetic nerves, enteric nerves,pacemaker cells (interstitial cells of Cajal) or smooth
muscle cells in the intestinal wall. The stimulation was justat the sensory threshold and did not produce striated muscle
[1] van Ginkel R, Reitsma JB, Buller HA, et al. Childhood constipation:
contraction or pain, so was not stimulating A-δ or C
longitudinal follow-up beyond puberty. Gastroenterology 2003;125:
(nociceptor/pain) fibres. The effects took months to develop
[2] Benninga MA, Buller HA, Tytgat GN, et al. Colonic transit time in
and lasted for months, suggesting it was changing nerve
constipated children: does pediatric slow-transit constipation exist?
circuits or overall neuronal health, rather than causing
J Pediatr Gastroenterol Nutr 1996;23:241-51.
[3] Hutson JM, Catto-Smith T, Gibb S, et al. Chronic constipation: no
We have previously reported on the use of IFC to treat
longer stuck! Characterization of colonic dysmotility as a new disorder
chronic constipation and STC in children
in children. J Pediatr Surg 2004;39:795-9.
[4] Gutierrez C, Marco A, Nogales A, et al. Total and segmental
Other groups have demonstrated that IFC increased
colonic transit time and anorectal manometry in children with
gastrointestinal motility producing diarrhoea im-
chronic idiopathic constipation. J Pediatr Gastroenterol Nutr 2002;
proved gastric emptying , improved functional dyspepsia
symptoms and increased rate of swallowing
[5] Clarke MC, Chow CS, Chase JW, et al. Quality of life in children with
Dinning et al. performed 24-h colonic manometry in 8 adults
slow transit constipation. J Pediatr Surg 2008;43:320-4.
[6] King SK, Sutcliffe JR, Southwell BR, et al. The antegrade continence
with STC during direct stimulation of sacral nerve S3 and
enema successfully treats idiopathic slow-transit constipation. J Pediatr
showed there was increased pancolonic PS .
The electrical parameters used in this study were those
[7] King SK, Catto-Smith AG, Stanton MP, et al. 24-Hour colonic
previously used for bladder stimulation. Stimulation was
manometry in pediatric slow transit constipation shows significant
performed by physiotherapists with patients visiting clinics 3
reductions in antegrade propagation. Am J Gastroenterol 2008;103:2083-91.
times a week. Following 1 month of IFC, symptoms
[8] Stanton MP, Hutson JM, Simpson D, et al. Colonic manometry via
improved over the following 2 months after stimulation,
appendicostomy shows reduced frequency, amplitude, and length of
with more improvement at 7 months (both patients had
propagating sequences in children with slow-transit constipation. J
stopped using their appendix stomas and doing washouts, and
were defecating regularly with no impaction). We have
[9] Robertson VJ, Low J, Reed A, et al. Electrotherapy explained:
principles and practice4th ed. ; 2006.
previously reported the long-term follow-up of the rando-
[10] Emmerson CA. A preliminary study of the effect of interferential
mised control trial and crossover treatment and this
therapy on detrusor instability in patients with multiple sclerosis. Aust
showed that symptom improvement lasted 3–6 months or
more than 2 years and that 2 months' stimulation produced
[11] Kajbafzadeh AM, Sharifi-Rad L, Baradaran N, et al. Effect of pelvic
greater improvement than 1 month. Following the release of
floor interferential electrostimulation on urodynamic parameters andincontinency of children with myelomeningocele and detrusor
battery-operated machines, daily stimulation at home was
overactivity. Urology 2009;74:324-9.
tested and this produced increased defecation suggest-
[12] Chase J, Robertson VJ, Southwell B, et al. Pilot study using
ing a dose response. Further studies on larger numbers of
transcutaneous electrical stimulation (interferential current) to treat
chronic treatment-resistant constipation and soiling in children.
colonic propagating pressure waves in severe constipation. Neurogas-
J Gastroenterol Hepatol 2005;20:1054-61.
troenterol Motil 2010;22(12):e340-9.
[13] Ismail KA, Chase J, Gibb S, et al. Daily transabdominal electrical
[20] van den Berg MM, Hogan M, Caniano DA, et al. Colonic manometry
stimulation at home increased defecation in children with slow-
as predictor of cecostomy success in children with defecation
transit constipation: a pilot study. J Pediatr Surg 2009;44:
disorders. J Pediatr Surg 2006;41:730-6 [discussion 730–736].
[21] Clarke MC, Chase JW, Gibb S, et al. Improvement of quality of life in
[14] Clarke MC, Chase JW, Gibb S, et al. Decreased colonic transit time
children with slow transit constipation after treatment with transcutaneous
after transcutaneous interferential electrical stimulation in children
electrical stimulation. J Pediatr Surg 2009;44:1268-72 [discussion 1272].
with slow transit constipation. J Pediatr Surg 2009;44:408-12.
[22] Weinkauf JG, Yiannopoulos A, Faul JL. Transcutaneous electrical
[15] Leong LC, Yik YI, Catto-Smith AG, et al. Long-term effects of
nerve stimulation for severe gastroparesis after lung transplantation.
transabdominal electrical stimulation in treating children with slow-
J Heart Lung Transplant 2005;24:1444.
transit constipation. J Pediatr Surg 2011;46:2309-12.
[23] Koklu S, Koklu G, Ozguclu E, et al. Clinical trial: interferential electric
[16] Yik YI, Ismail KA, Hutson JM, et al. Home transcutaneous electrical
stimulation in functional dyspepsia patients — a prospective
stimulation to treat children with slow-transit constipation. J Pediatr
randomized study. Aliment Pharmacol Ther. 31:961-8.
[24] Furuta T, Takemura M, Tsujita J, et al. Interferential electric stimulation
[17] Sutcliffe JR, King S, Hutson JM, et al. What is new in radiology and
applied to the neck increases swallowing frequency. Dysphagia
pathology of motility disorders in children? Semin Pediatr Surg
[25] Dinning PG, Fuentealba SE, Kennedy ML, et al. Sacral nerve
[18] Dinning PG, Szczesniak MM, Cook IJ. Spatio-temporal analysis
stimulation induces pan-colonic propagating pressure waves and
reveals aberrant linkage among sequential propagating pressure wave
increases defecation frequency in patients with slow-transit constipa-
sequences in patients with symptomatically defined obstructed
defecation. Neurogastroenterol Motil 2009;21:945-e975.
[26] Leong LC, Yik YI, Catto-Smith AG, et al. Long-term effects of
[19] Dinning PG, Zarate N, Hunt LM, et al. Pancolonic spatiotemporal
transabdominal electrical stimulation in treating children with slow-
mapping reveals regional deficiencies in, and disorganization of
transit constipation. J Ped Surg 2011;46(12):2309-12.
Dr. med. habil. Rüdiger Schellenberg Talstraße 29 35625 Hüttenberg Stand: Januar/ 2012 Literaturverzeichnis Publikationen und Buchbeiträge 1. Blume, M. und Schellenberg, R.: Screening-Test für geeignete Adsorptionsmittel zur Extraktion von biologisch wirksamen Vasopression aus Plasma. Diplomarbeit, Medizinis
This document sets out the basis on which the service is provided. Dolmens Insurance Brokers Ltd 37/44 Butterly Business Park About our insurance services 1. The Financial Services Authority (FSA) The FSA is the independent watchdog that regulates financial services. It requires us to give you this document. Use this information to decide if our services are right for you.
 Journal of Pediatric Surgery (2012) 47, 2279–2284
Transabdominal electrical stimulation increases colonicpropagating pressure waves in paediatric slowtransit constipation☆,☆☆,★
Melanie C.C. Clarke a, Anthony G. Catto-Smith a,b,c, Sebastian K. King a,c,Phil G. Dinning d, Ian J. Cook d, Janet W. Chase a, Susan M. Gibb a,b,Val J. Robertson e, Di Simpson b, John M. Hutson b,c, Bridget R. Southwell a,c,⁎
aMurdoch Childrens Research Institute, Melbourne, AustraliabRoyal Children's Hospital, Melbourne, AustraliacDepartment of Paediatrics, University of Melbourne, AustraliadSt George Hospital, and Department of Medicine, University of New South Wales, Sydney, NSWeUniversity of Newcastle, Australia
Received 31 August 2012; accepted 1 September 2012
Background and aims: In slow-transit constipation (STC) pancolonic manometry shows significantly
reduced antegrade propagating sequences (PS) and no response to physiological stimuli. This study
aimed to determine whether transcutaneous electrical stimulation using interferential current (IFC)
applied to the abdomen increased colonic PS in STC children.
Journal of Pediatric Surgery (2012) 47, 2279–2284
Transabdominal electrical stimulation increases colonicpropagating pressure waves in paediatric slowtransit constipation☆,☆☆,★
Melanie C.C. Clarke a, Anthony G. Catto-Smith a,b,c, Sebastian K. King a,c,Phil G. Dinning d, Ian J. Cook d, Janet W. Chase a, Susan M. Gibb a,b,Val J. Robertson e, Di Simpson b, John M. Hutson b,c, Bridget R. Southwell a,c,⁎
aMurdoch Childrens Research Institute, Melbourne, AustraliabRoyal Children's Hospital, Melbourne, AustraliacDepartment of Paediatrics, University of Melbourne, AustraliadSt George Hospital, and Department of Medicine, University of New South Wales, Sydney, NSWeUniversity of Newcastle, Australia
Received 31 August 2012; accepted 1 September 2012
Background and aims: In slow-transit constipation (STC) pancolonic manometry shows significantly
reduced antegrade propagating sequences (PS) and no response to physiological stimuli. This study
aimed to determine whether transcutaneous electrical stimulation using interferential current (IFC)
applied to the abdomen increased colonic PS in STC children.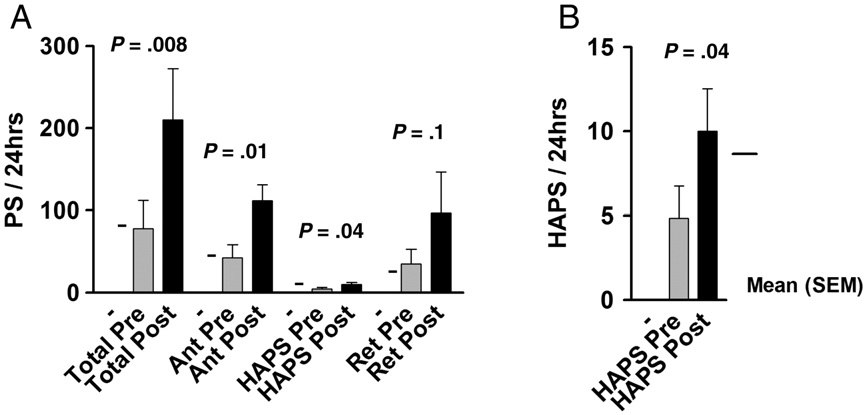 statistically significant. For one patient, recording stopped
initiation moved from the splenic flexure before stimulation,
during the 2nd session and this patient was not included
to the rectosigmoid after stimulation. Pre-treatment 4/5
patients had antegrade and 2/5 had retrograde coloniccomplexes, whilst post-treatment all 5 had antegrade and 3/5 had retrograde colonic complexes. There was no change in
percent of antegrade linked-sequences (pre-treatment 65% ±8%, mean ± SEM, post-treatment 56% ± 4.5%), but unexpect-edly, there was a significant decrease in retrograde linked-
Children had colonic manometry before and 2 months
sequences (61% ± 4.5%, 33% ± 9.8%, p = 0.04 t-test).
statistically significant. For one patient, recording stopped
initiation moved from the splenic flexure before stimulation,
during the 2nd session and this patient was not included
to the rectosigmoid after stimulation. Pre-treatment 4/5
patients had antegrade and 2/5 had retrograde coloniccomplexes, whilst post-treatment all 5 had antegrade and 3/5 had retrograde colonic complexes. There was no change in
percent of antegrade linked-sequences (pre-treatment 65% ±8%, mean ± SEM, post-treatment 56% ± 4.5%), but unexpect-edly, there was a significant decrease in retrograde linked-
Children had colonic manometry before and 2 months
sequences (61% ± 4.5%, 33% ± 9.8%, p = 0.04 t-test).