Journal of Hepatology 40 (2004) 228–233
Weight gain after transjugular intrahepatic portosystemic shunt is
associated with improvement in body composition in malnourished
patients with cirrhosis and hypermetabolism
Mathias Plauth1,*, Tatjana Schu¨tz1, Deborah P. Buckendahl1, Georg Kreymann2,
Matthias Pirlich1, Sven Gru¨ngreiff1, Paul Romaniuk3, Siegfried Ertl4,
1Medizinische Klinik mit Schwerpunkt Gastroenterologie, Hepatologie und Endokrinologie, Charite´ Universita¨tsmedizin Berlin, Berlin, Germany
2Medizinische Klinik, Universita¨tsklinikum Hamburg Eppendorf, Hamburg, Germany3Institut fu¨r Ro¨ntgendiagnostik, Charite´ Univerista¨tsmedizin Berlin, Berlin, Germany
4Helios Klinikum Berlin, Klinikum Buch, Nuklearmedizinische Klinik, Berlin, Germany
Background/Aims: To search for changes in body composition and energy metabolism associated with the repeatedly
observed weight gain of cirrhotic patients after portosystemic shunting.
Methods: Twenty-one patients were studied prospectively before and 6 and 12 months after transjugular intrahepatic
portosystemic shunt (TIPS) to assess body cell mass by two independent methods (total body potassium counting: bodycell mass determined by TBP, BCMTBP, bioelectric impedance analysis: body cell mass determined by BIA, BCMBIA),muscle mass (anthropometry), resting energy expenditure (REECALO) by indirect calorimetry, and nutritional intakeby dietary recall analysis.
Results: Prior to TIPS patients were hypermetabolic in terms of measured vs. predicted REE (REECALO median 1423
(range 1164 – 1838) vs. REEPRED 1279 (1067 –1687) kcal; P < 0.05) and their body cell mass was lower (19.1 (10.9 –33.4)vs. 31.7 (16.8 – 47.1) kg; P 5 0.001). After TIPS body cell mass (BCMBIA) increased to 23.5 (12.7 –44.3) (P < 0.025) and25.7 (14.2 – 39.7) kg (P 5 0.05) at 6 and 12 months after TIPS and this was confirmed by total potassium counting(BCMTBP before TIPS: 18.8 (10.6 –26.7) vs. 22.4 (12.9 – 28.5) kg at 6 months; P < 0.01). Hypermetabolism persistedthroughout the study period. Energy and protein intake increased significantly by 26 and 33%.
Conclusions: An increase of prognostically relevant variables body cell and muscle mass contributes to the weight
gain after TIPS in malnourished patients with cirrhosis and hypermetabolism.
q 2003 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Keywords: Body cell mass; Nutritional state; Encephalopathy; Protein intake; Bioelectrical impedance analysis
Received 13 February 2003; received in revised form 3 October 2003;
* Corresponding author. Klinik fu¨r Innere Medizin, Staedtisches
Klinikum, Auenweg 38, D-06847 Dessau, Germany. Tel.: þ 49-430-501-
Protein energy malnutrition is a frequent consequence of
hepatic cirrhosis which puts patients at a higher risk of
E-mail address: [email protected] (M. Plauth).
complications , death and a complicated course
Abbreviations: TIPS, transjugular intrahepatic portosystemic shunt; BCM,
after liver transplantation including death After
body cell mass; BCMTBP, body cell mass determined by TBP; TBP, total
successful treatment of portal hypertension by surgical or
body potassium; BCMBIA, body cell mass determined by BIA; BIA,bioelectrical impedance analysis; REE, resting energy expenditure; BMI,
interventional shunt procedures weight gain and improve-
body mass index; MAMA, mid-arm muscle area; MAFA, mid-arm fat area;
ment in the nutritional status have been reported repeatedly
R, resistance; Xc, reactance; FFM, fat-free mass; TBW, total body water;
. In cirrhosis, however, the precise assessment of
TBPMEAS, total body potassium measured values; TBPPRED, total body
nutritional state is complicated by water retention .
potassium content predicted normal values; REECALO, resting energy
Recently, Selberg and coworkers found that the
expenditure measured by indirect calorimetry; REEPRED, resting energyexpenditure predicted from regression equations of healthy controls.
reduction in preoperative body cell mass was a relevant
0168-8278/$30.00 q 2003 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.jhep.2003.10.011
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
predictor of a less favourable outcome of liver
Body weight was measured to the nearest 0.1 kg on a hospital scale and
In a prospective study we therefore assessed the
body mass index (BMI) was calculated.
Anthropometric measurements were made at the non-dominant arm
evolution of body composition, energy expenditure, nutrient
using a skinfold caliper (Holtain, Crymych, UK) and a flexible tape
intake, as well as mental state over periods of 6 and 12
measure to calculate mid-arm muscle area (MAMA), mid-arm fat area
months after a transjugular intrahepatic portosystemic stent-
shunt (TIPS) had been inserted As a reference body
Bioelectrical impedance analysis was performed as described else-
where using a BIA 2000-M analyzer (Data Input, Frankfurt/Main,
cell mass estimated by bioelectrical impedance analysis and
Germany) at 50 kHz to measure resistance (R), reactance (Xc) and phase
resting energy expenditure were determined in healthy
angle a. The coefficients of variation for R and Xc were 1.1 and 2.7% in
controls, too. Specifically, we were interested to see: (1)
patients without ascites and 2.1 and 3.9% in patients with ascites. BCM
whether the weight gain following TIPS was associated with
the formulae for fat-free mass (FFM) as TBW/0.732 and total body water
an increase in the metabolically relevant compartments
muscle mass or body cell mass as assessed by two
Total body potassium content (TBP) is being considered a valid
measure of BCM and due to limited access was determined only prior
independent methods; and (2) whether patients with TIPS
to TIPS and after 6 months by measuring the amount of the naturally
do tolerate a diet according to the European Society for
occurring radioisotope 40K using a shielded-room whole-body counter
Clinical Nutrition and Metabolism (ESPEN) guidelines
(Nuclear Enterprises Ltd., Edinburgh, UK) working with four NaI(T1)detectors (Berthold, Wildbad, Germany), as described elsewhere . The
without adverse effects on mental state.
coefficient of variation for repeated measurements was # 2%. BCM wascalculated from TBP as BCM
TBP measurement was not available for the cohort of 310 healthyindividuals. Therefore, measured TBP (TBPMEAS) in cirrhotic patients was
compared with predicted normal values (TBPPRED) calculated from theequations given by McMillan for males as TBP
height) 2 (4.51 £ age) 2 2483 and for females as TBP
Twenty-one patients (13 men, eight women; age: 60.0 (38.7 – 71.6)
years) with liver cirrhosis of alcoholic (n ¼ 19) or non-alcoholic (oneautoimmune hepatitis, one primary biliary cirrhosis) origin were studied
Respiratory gas exchange was measured by indirect calorimetry
prospectively before and 6.0 (5.0 – 7.4) months as well as 12.5 (11.8 – 14.9)
(Deltatrac II, Datex, Bremen, Germany). The intraindividual coefficient
months after TIPS insertion. The indications for TIPS insertion were
of variation of repeated measurements was 3.4% for oxygen consumption
recurrent esophageal variceal bleeding in 14 patients (nine without ascites
and 5.1% for carbon dioxide production. Resting energy expenditure
and five with ascites) and refractory ascites in seven patients. The Child-
(REECALO) was calculated according to Consolazio To search for
Pugh Score was calculated to classify severity of cirrhosis. Of the 21
hypermetabolism in each patient the REECALO was compared to REEPRED
patients included in the study five dropped out after month 6 due to
calculated as a function of measured BCM. REEPRED was calculated from
transplantation (n ¼ 1), death (n ¼ 1), TIPS occlusion (n ¼ 2) and loss to
gender specific regression equations derived from our cohort of healthy
During the initial and follow-up hospitalizations all patients received
dietary counselling according to the ESPEN guidelines Nutritional andmental state were assessed on the occasion of the scheduled visits at months
6 and 12 as part of routine admissions (months 1, 3, 6 and 12 after TIPS
Energy and protein intake of the preceding 2 weeks were assessed prior
insertion) to check for TIPS patency. All patients gave written informed
to TIPS and after 6 months by a standardized diet history (EBISe,
consent for the metabolic study after the indication for the TIPS procedure
Forschungszentrum fu¨r Erna¨hrung, Stuttgart, Germany) Portion sizes
had been established independently and the patients’ consent for the TIPS
of the amount of ingested legumes, potatoes, chips, rice and noodles were
procedure had been obtained. The study protocol conformed to the 1975
estimated by using photographs of four to six portion sizes between 50 and
Helsinki declaration and was approved by the local ethics committee.
A cohort of 310 healthy volunteers consented to have indirect
calorimetry and body composition analysis done by means of bioelectricalimpedance analysis (BIA). From this cohort gender specific regression
equations were derived to calculate expected resting energy expenditure
A battery of six validated psychometric tests (number connection tests
(REE) values for each patient. For the comparison of body cell mass
A and B, digit symbol test, pointing test, line tracing test time and line
determined by BIA (BCMBIA) one healthy individual was matched to each
tracing test mistakes) were performed prior to TIPS insertion as well as 6
patient according to gender and age within ^ 2 years
and 12 months thereafter. In addition to the time needed to execute or thenumber of mistakes the results of each test were classified on a five mark
scale: (þ 1) better than mean þ 1 SD, (0) between mean and mean ^ 1 SD,(2 1) between mean 2 1 SD and mean 2 2 SD, (2 2) between mean 2 2 SDand mean 2 3 SD, and (2 3) less than mean 2 3 SD using age matched
reference values . The global performance of each patient at one testsession was expressed as the average of marks scored in each of the six
TIPS insertion was performed according to the method described by
tests. For follow-up visits four different test arrangements were available to
Ro¨ssle et al. using Memotherme (Angiomed, Karlsruhe, Germany)
devices. There were no intervention associated complications during thefirst 4 weeks. In all patients the TIPS angiography was done 6 months after
TIPS insertion as scheduled, while in seven patients additional angio-graphic interventions were necessary prior to the scheduled one at 6
Results are given as median and range. Statistical analysis was
months. In the whole group reinterventions with dilatation (n ¼ 5) or
performed using the computer software program SPSS (Version 9.0). The
dilatation and insertion of additional stents (n ¼ 10) were required to
Wilcoxon signed rank-sum test was used to compare the values before and
maintain TIPS patency until 6 months and eight reinterventions were
after TIPS insertion as well as between patients before TIPS and controls.
Predicted and measured values were analysed by Mann – Whitney U-test.
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
Linear regression analysis based on the control group was used to calculatepredicted values for REE in the study population. Frequencies wereevaluated by the x2-test. Correction for multiple comparisons (6 and12 months after TIPS vs. before TIPS) was performed according toBonferroni with a probability level of less than 0.025 accepted asstatistically significant. Otherwise P , 0:05 was considered statisticallysignificant.
TIPS was well tolerated by all patients. Among the
14 patients in whom TIPS was performed for treatment ofvariceal hemorrhage, there was one episode of varicealbleeding within the first 6 months and one at month 9 due toTIPS occlusion which required a surgical shunt procedure ascompared to 4 (0 – 10) episodes in the year prior to TIPS(P , 0:001) and ascites was absent (n ¼ 4) or moderate(n ¼ 1) in the five patients who also had ascites prior toTIPS. Ascites improved significantly in all seven patients in
Fig. 1. Reduction in body cell mass measured by bioelectricalimpedance analysis (BCM
whom TIPS was performed for treatment of refractory
BIA) in patients (before TIPS) as compared
to age and sex matched controls (C). Gain in BCMBIA of patients at 6
ascites so that ascites grade decreased from a median grade
(TIPS-6) and 12 months (TIPS-12) after TIPS. Box plots with
of 2 (moderate ascites) to a median grade of 1 (no ascites).
horizontal bars indicating median values, boxes indicating the 25th
In fact, none of the patients required further paracenteses.
centiles, error bars indicating the 95% confidence interval and o
TIPS insertion resulted in a persistent reduction of
indicating values outside the 95th centile. ***P < 0.001. [This figureappears in colour on the web.]
portocaval pressure gradient from 23.0 (12 – 29) mmHgprior to TIPS to 15.5 (8 – 21) mm Hg at 6 months(P ¼ 0:002) and 11.5 mmHg at 12 months
Six months after TIPS insertion the patients as a
(P ¼ 0:001) determined on control angiography prior to
group had gained body weight (77.0 (49.0 – 138.5) vs.
any TIPS reintervention. Endogenous creatinine clearance
69.5 (52.0 – 115.0) kg; P ¼ 0:001; weight change 8.0
increased from 94.9 (34.4 – 184.3) ml/min prior to TIPS to
(2 3.7 – 23.5); increase n ¼ 16, stable n ¼ 3, loss n ¼ 2)
98.1 (33.4 – 205.7) ml/min at 6 months and 126.7
reflected by a significant increase in BMI by 11% from
(51.1 – 286.6) ml/min at 12 months (n.s.). Prior to TIPS
22.3 (18.0 – 35.1) to 26.2 (18.3 – 40.0) kg/m2 (P , 0:001).
insertion 67% (14/21) of patients were on diuretics with a
This increase was due to a gain in muscle mass by 18%
median daily dose of oral spironolactone (141.4
in terms of MAMA (48.0 (27.6 – 95.9) vs. 42.6
(21.7 – 88.3) cm2; P ¼ 0:001) or muscle mass as deter-
(5.7 – 80.0) mg, n ¼ 10). At 6 and 12 months, 67 and 44%
mined by the Heymsfield method (23.3 (14.2 – 45.7) vs.
of patients were on diuretics, but at a significantly lower
20.6 (11.4 – 42.7) kg; P ¼ 0:002), while fat mass
daily dose (spironolactone 6 months: 100.0 (42.9 – 142.9)
remained unaltered (MAFA 21.3 (6.7 – 64.9) vs. 23.3
mg, n ¼ 13, P , 0:01; 12 months: 75.0 (50.0– 100.0)
(6.1 – 51.3) cm2). Accordingly, a gain in the metabolically
mg, n ¼ 6, P , 0:01; furosemide 6 months: 40.0
active compartment body cell mass could be demon-
(2.9 – 80.0) mg, n ¼ 11, P , 0:025; 12 months: 30.0
strated by two independent methods: bioelectrical impe-
(20.0 – 80.0) mg, n ¼ 6, P , 0:01).
dance analysis (BCMBIA: 23.5 (12.7 – 44.3) vs. 19.1(10.9 – 33.4) kg; þ 15%; P , 0:025) and total body
potassium counting (BCMTBP 22.2 (12.9 – 28.5) vs. 18.8(10.6 – 26.7) kg; þ 15%; P , 0:01; BCMTBP even
Weight 69.5 (52.0 – 115.0) vs. 74.0 (45.0 – 115.0) kg,
increased to the level of predicted normal values
height 170 (158 – 185) vs. 171 (152 – 185) cm) and body
(87 ^ 5%; ns) at 6 months, as opposed to 77 ^ 5%
mass index 22.3 (18.0 – 35.1) vs. 25.6 (16.9 – 37.4) kg/m2)
prior to TIPS (P , 0:01), again showing a significant
were not different between patients and controls. However,
improvement (P , 0:01) after TIPS insertion ().
patients with cirrhosis showed a significant reduction in
In the subgroup of 16 patients also studied 12 months
metabolically relevant lean tissue, both in terms of body cell
after TIPS insertion, a persistent gain in weight of 0.9
mass (BCMBIA 19.1 (10.9 – 33.4) vs. 31.7 (16.8 –47.1) kg;
(2 9.1 – 8.0) to (72.7 (54.0 – 142.6) kg; P , 0:01), body
P ¼ 0:001, calculated from impedance measure-
mass index (25.8 (20.6 – 42.6) kg/m2; P , 0:025), arm
ments and in terms of the directly measured variable phase
muscle area (16.8 (9.7 – 69.8) cm2; P , 0:001) and body cell
angle a (4.5 (2.9 – 6.2)8 vs. 6.5 (5.8 – 7.5)8; P , 0:001) when
mass (BCMBIA 25.7 (14.2 – 40.0) kg, n.s., ; phase
compared to age and gender matched controls.
angle a 5.2 (3.8 – 6.0)8, n.s.) could be demonstrated.
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
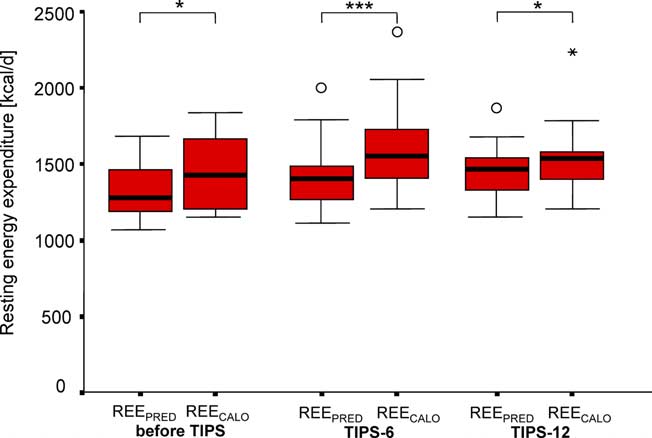
(P , 0:025). Measured REECALO remained higher thanpredicted values REEPRED at 6 months (1550 (1203 – 2364)vs. 1402 (1112 – 2000) kcal/d; P ¼ 0:001) and 12 months(1532 (1208 – 2232) vs. 1465 (1152 – 1868) kcal/d;P , 0:05) after TIPS, but the initial difference decreasedduring follow-up.
Total energy intake before TIPS was 1842 (1334 – 3687)
kcal/d and increased by 6 months after TIPS by 26% to 2533(1014 – 4062) kcal/d (P , 0:05). This was due to an increasein protein (1.2 (0.7 – 1.7) g kg21 d21 vs. 0.9 (0.5 – 1.2) gkg21 d21; P ¼ 0:05) and carbohydrate intake (3.7 (2.0–5.4)g kg21 d21 vs. 2.9 (1.7 – 4.9) g kg21 d21; P ¼ 0:05), while
Fig. 2. Reduction in body cell mass (BCMTBP) assessed by total body
fat intake remained unchanged (1.4 (0.6 – 2.0) g kg21 d21
potassium counting in patients before TIPS. Patient values are
compared to predicted normal values calculated according toMcMillan Six months after TIPS BCMTBP has increased
significantly and is no longer different from predicted values. Legendsand box plot as explained in **P < 0.01. [This figure appears incolour on the web.]
The majority of patients (63 – 95% before TIPS and
47 – 95% after TIPS) performed below the limit (age
adjusted mean minus two standard deviations) in individualpsychometric tests with the exception of line tracing errors,
Before TIPS patients had a measured total body
but not time. After TIPS, there were significant improve-
ments in the number connection test B (P ¼ 0:001) at month
CALO of 1449 (1164 – 1838) kcal/d which was lower
than in matched controls (1644 (1117 – 2181) kcal/d;
6 and the pointing test at months 6 and 12 (P , 0:01 and
P , 0:05). However, when the patients’ energy expenditure
P , 0:025) In terms of global performance,
was calculated using the regression equations, their
however, there was no improvement after TIPS (n.s.).
predicted metabolic rate REEPRED (1279 (1067 – 1687)kcal/d was significantly lower than the measured REECALO1423 (1164 – 1837) kcal/d; P , 0:05; indicating
In this prospective study we demonstrated that body cell
mass in patients with liver cirrhosis is severely reduced andthis condition does not inevitably run a downhill course butcan be ameliorated as demonstrated in a patient cohorttreated with TIPS. Using three independent methods(anthropometry, bioelectrical impedance analysis, totalbody potassium counting) to analyse body composition wecould not only confirm the repeatedly claimed improvementin nutritional state after successful portosystemic shuntingbut also show that this improvement is associated with again in the metabolically relevant compartments musclemass (anthropometry) and body cell mass (bioelectricimpedance analysis and total body potassium counting). As would be expected, this gain in lean body mass was notcorrelated with weight change since improvement of ascites
Fig. 3. Hypermetabolism in liver cirrhosis before TIPS and at 6
was observed after TIPS as well. BCM is the sub-
(TIPS-6) and 12 (TIPS-12) months after TIPS. Resting energy
compartment of lean body mass, in which 99% of the
expenditure was measured by indirect calorimetry (REECALO) and
body’s metabolic processes take place , and significant
values are compared with predicted REEPRED from actual BCM using
losses of which are tightly linked to mortality . The
regression equations of healthy volunteers (for details see text).
fact that the improvement in nutritional state was more
Legends and box plot as explained in . *P < 0.05, ***P 5 0.01. [This figure appears in colour on the web.]
readily observed in our patient population but only less so in
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
Table 1Overview of psychometric tests results before and 6 and 12 months after TIPS
Values are median (range). Results were available for statistical analysis in 19/21 or 15/16 patients due to test termination prior to maximum time (# one
another study may be related to the degree of
counselling, unless supplemental artificial feeding provides
malnutrition prior to TIPS insertion as reflected by
additional energy and protein . We were pleased to
the severe reduction in BCM in our patients. As shown
see that, after TIPS insertion patients managed to increase
recently there is reasonable agreement between BIA
total energy (þ 26%) and protein intake (þ 33%) and
and TBP counting regarding the determination of BCM
reached a stable anabolic state without any nutritional
even in cirrhotic patients with massive ascites. Body cell
intervention apart from dietary counselling. This obser-
mass calculation from TBP or BIA data is based on
vation shows that in a group of patients with predominantly
assumptions which may not be fully adequate in cirrhosis
repeated variceal hemorrhage receiving TIPS as salvage
and, therefore, it is important to see the major result of the
therapy the loss of BCM does not inevitably progress but
study confirmed by independent methodology, such as an
can actually be stopped and reverted to increase. Whether
increase in muscle mass and the recent findings of
this favourable change was causally related to TIPS cannot
be answered from the present data. One may speculate,however, that the treatment of portal hypertension may have
improved intestinal nutrient absorption, food intake due torelief from abdominal fullness, or protein anabolism after a
Searching for changes in energy metabolism as a
prolonged period without catabolic insults from hemorrhage
potential cause for the improvement of nutritional status,
or paracenteses. It is conceivable that the absence of a
we observed an increase in total resting energy expenditure
worsening in mental state in our cohort of patients with
REECALO following TIPS and this occurred irrespective of
psychometrically diagnosed subclinical encephalopathy is a
the presence of ascites prior to TIPS To correct for the
result of pro-encephalopathic interventions like TIPS on the
effects of changes in BCM we related REECALO to
one hand and anti-encephalopathic interventions like
REEPRED predicted from the measured BCM of each patient
adequate nutrition with a 33% percent increase in protein
using regression equations derived in the group of 310
consumption on the other hand. This would not be
healthy controls. We chose this approach to allow for the
surprising since controlled trials feeding high protein diets
curvilinear relationship between REE and BCM instead
to patients with liver cirrhosis have generated
of expressing this relationship as the ratio of REE/BCM
sound data to dismiss protein intolerance as a dangerous
which may erroneously overestimate REE in individuals
myth rather than a clinically relevant pathogenic principle
with low BCM. This analysis revealed hypermetabolism in
patients prior to TIPS which persisted throughout the
We conclude that even malnourished patients with liver
observation period of 12 months but showed a tendency to
cirrhosis and hypermetabolism are capable to improve their
decrease. This observation may reflect the ongoing chronic
lean body mass and this increase of prognostically relevant
liver disease and the TIPS associated augmentation of
variables body cell and muscle mass contributes to the
portalsystemic shunting on the one hand and the improved
nutrient balance on the other hand which requires long-termrather than short-term follow-up to detect an improvementof body composition.
[1] Plauth M, Merli M, Kondrup J, Ferenci P, Weimann A, Mu¨ller MJ.
ESPEN guidelines for nutrition in liver disease and transplantation.
Before TIPS, our patients were malnourished despite a
numerically adequate nutrient intake. Many patients with
[2] Mendenhall CL, Moritz TE, Roselle GA, Morgan TR, Nemchausky
cirrhosis cannot reach a stable anabolic state despite dietary
BA, Tamburro CH, et al. A study of oral nutritional support with
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
oxandrolone in malnourished patients with alcoholic hepatitis: results
health: effects of age, sex, height, and fat. Am J Physiol 1974;226:
of a department of veterans affairs cooperative study. Hepatology
[21] Ertl S, Tautz M, Deckart H, Mischke W. Physikalische Charakter-
[3] Caregaro L, Alberino F, Amodio P, Merkel C, Bolognesi M, Angeli P,
isierung und klinischer Einsatz des rekonstruierten Ganzko¨rperza¨hlers
et al. Malnutrition in alcoholic and virus-related cirrhosis. Am J Clin
in der Nuklearmedizinischen Klinik Berlin-Buch. Radiobiol Radio-
[4] Merli M, Riggio O, Dally L, and PINC. Does malnutrition affect
[22] Cohn SH, Vasvani AN, Yasumura S, Yuen K, Ellis KJ. Assessment of
survival in cirrhosis? Hepatology 1996;23:1041– 1046.
cellular mass and lean body mass by non-invasive nuclear techniques.
[5] Pikul J, Sharpe MD, Lowndes R, Ghent CN. Degree of preoperative
malnutrition is predictive of postoperative morbidity and mortality in
[23] McMillan DC, Preston T, Watson WS, Simpson JM, Fearon KCH,
liver transplant recipients. Transplantation 1994;57:469 – 472.
Shenkin A, et al. Relationship between weight loss, reduction of body
[6] Selberg O, Bo¨ttcher J, Tusch G, Pichlmayr R, Henkel E, Mu¨ller MJ.
cell mass and inflammatory response in patients with cancer. Br J Surg
Identification of high- and low risk patients before liver transplan-
tation: a prospective cohort study of nutritional and metabolic
[24] Consolazio CF, Johnson RE, Pecora LJ. Physiological measurements
parameters in 150 patients. Hepatology 1997;25:652 – 657.
of metabolic functions in man. New York: McGraw Hill; 1963. p.
[7] Orloff MJ. Pathogenesis and surgical treatment of intractable ascites
associated with alcoholic cirrhosis. Ann N Y Acad Sci 1970;170:
[25] Landig J, Erhardt JG, Bode JC, Bode C. Validation and comparison of
two computerized methods of obtaining a diet history. Clin Nutr 1998;
[8] Ochs A, Ro¨ssle M, Haag K, Hauenstein K, Deibert P, Siegerstetter
V, et al. The transjugular intrahepatic portosystemic stent-shunt
[26] Schomerus H, Weissenborn K, Hecker H, Hamster W, Ru¨ckert N.
procedure for refractory ascites. N Engl J Med 1995;332:
PSE Syndrome Test. Psychodiagnostisches Verfahren zur quantitati-
ven Erfassung der (minimalen) portosystemischen Encephalopathie(PSE). Frankfurt: Swets & Zeitlinger B.V., Swets Test Services; 1999.
[9] Sanyal AJ, Freedman AM, Luketic VA, Purdum iii PP, Shiffman ML,
[27] Moore FD. Energy and the maintenance of the body cell mass. J Parent
DeMeo J, et al. The natural history of portal hypertension after
transjugular intrahepatic portosystemic shunts. Gastroenterology
¨ ber die Atrophie der menschlichen Organe bei Inanition.
Z Angew Anat Konstitutionslehre 1921;7:87 – 134.
[10] Trotter JF, Suhocki PV, Rockey DC. Transjugular intrahepatic
[29] Kotler DP, Tierney AR, Pierson RN. Magnitude of body cell mass
portosystemic shunt (TIPS) in patients with refractory ascites: effect
depletion and the timing of death from wasting in AIDS. Am J Clin
on body weight and Child-Pugh score. Am J Gastroenterol 1998;93:
[30] Selberg O, Bo¨ttcher J, Pirlich M, Henkel E, Manns MP, Mu¨ller MJ.
[11] Prijatmoko D, Strauss BJG, Lambert JR, Sievert W, Stroud DB,
Clinical significance and correlates of whole body potassium status in
Wahlqvist ML, et al. Early detection of protein depletion in alcoholic
patients with liver cirrhosis. Hepatol Res 1999;16:36– 48.
cirrhosis: role of body composition analysis. Gastroenterology 1993;
[31] Allard JP, Chau J, Sandokji K, Blendis LM, Wong F. Effects of ascites
resolution after successful TIPS on nutrition in cirrhotic patients with
[12] Schu¨tz T, Zillich DP, Jurczyk S, Ertel S, Lochs H, Plauth M.
refractory ascites. Am J Gastroenterol 2001;96:2442 – 2447.
Improvement in body composition after transjugular intrahepatic
[32] Dolz C, Raurich JM, Ibanez J, Obrador A, Marse P, Gaya J. Ascites
portosystemic stent-shunt (TIPS) in patients with liver cirrhosis
increases the resting energy expenditure in liver cirrhosis. Gastro-
[abstract]. Gastroenterology 1999;116:A1274.
[13] Pugh RNH, Murray-Lyon IM, Dawson JL, Pietroni MC, Williams R.
[33] Heymsfield SB, Waki M, Reinus J. Are patients with chronic liver
Transsection of the oesophagus for bleeding oesophageal varices. Br J
disease hypermetabolic? Hepatology 1990;11:502 – 505.
[34] Weinsier RL, Schutz Y, Bracco D. Reexamination of the relationship
[14] Ro¨ssle M, Haag K, Ochs A, Sellinger M, No¨ldge G, Perarnau J-M,
of resting metabolic rate to fat-free mass and to the metabolically
et al. The transjugular intrahepatic portosystemic stent-shunt
active components of fat-free mass in humans. Am J Clin Nutr 1992;
procedure for variceal bleeding. N Engl J Med 1994;330:165– 171.
[15] Frisancho AR. New standards of weight and body composition by
[35] Cabre´ E, Gonzalez-Huix F, Abad-Lacruz A, Esteve M, Acero D,
frame size and height for assessment of nutritional status of adults and
Fernandez-Banares F, et al. Effect of total enteral nutrition on the
the elderly. Am J Clin Nutr 1984;40:808– 819.
short-term outcome of severely malnourished cirrhotics. A random-
[16] Heymsfield SB, McManus C, Smith J, Stevens V, Nixon DW.
ized controlled trial. Gastroenterology 1990;98:715 – 720.
Anthropometric measurement of muscle mass: revised equations for
[36] Kearns PJ, Young H, Garcia G, Blaschke T, O’Hanlon G, Rinki M.
calculating bone-free arm muscle area. Am J Clin Nutr 1982;36:
Accelerated improvement of alcoholic liver disease with enteral
nutrition. Gastroenterology 1992;102:200 – 205.
[17] Pirlich M, Spachos T, Schu¨tz T, Ertl S, Weiss M-L, Lochs H, et al.
[37] Morgan TR, Moritz TE, Mendenhall CL, Haas R, and VA
Bioelectrical impedance analysis is a useful bedside technique to
Cooperative study group. Protein consumption and hepatic encepha-
assess malnutrition in cirrhotic patients with and without ascites.
lopathy in alcoholic hepatitis. J Am Coll Nutr 1995;14:152– 158.
[38] Nielsen K, Kondrup J, Martinsen L, Dossing H, Larsson B, Stilling B,
[18] Lautz HU, Selberg O, Ko¨rber J, Bu¨rger M, Mu¨ller MJ. Protein-calorie
et al. Long-term oral refeeding of patients with cirrhosis of the liver.
malnutrition in liver cirrhosis. Clin Investig 1992;70:478 – 486.
[19] Kushner RF, Schoeller DA. Estimation of total body water by
[39] Soulsby CT, Morgan MY. Dietary management of hepatic encephalo-
bioelectrical impedance analysis. Am J Clin Nutr 1986;44:417 – 424.
pathy in cirrhotic patients: survey of current practice in United
[20] Pearson Jr RN, Lin DHY, Phillips RA. Total body potassium in
23th February, 2011 THE LONDON PMS AND MENOPAUSE February Newsletter I have decided to send my patients (or former patients) a monthly newsletter with up to date views on hormone therapy particularly if clarification of any newspaper reports are required. The following are recent articles on the benefits and risks of Th
Society for Ambulatory Anesthesia Consensus Statement on Perioperative Blood Glucose Management in Diabetic Patients Undergoing Ambulatory Surgery Girish P. Joshi, MB BS, MD, FFARCSI Anesthesia & Analgesia 2010; 111: 1378-87 A systematic review of the literature was conducted according the protocol recommended by the Cochrane Collaboration. The consensus panel used the Grading
 Journal of Hepatology 40 (2004) 228–233
Weight gain after transjugular intrahepatic portosystemic shunt is
associated with improvement in body composition in malnourished
patients with cirrhosis and hypermetabolism
Mathias Plauth1,*, Tatjana Schu¨tz1, Deborah P. Buckendahl1, Georg Kreymann2,
Matthias Pirlich1, Sven Gru¨ngreiff1, Paul Romaniuk3, Siegfried Ertl4,
1Medizinische Klinik mit Schwerpunkt Gastroenterologie, Hepatologie und Endokrinologie, Charite´ Universita¨tsmedizin Berlin, Berlin, Germany
2Medizinische Klinik, Universita¨tsklinikum Hamburg Eppendorf, Hamburg, Germany3Institut fu¨r Ro¨ntgendiagnostik, Charite´ Univerista¨tsmedizin Berlin, Berlin, Germany
4Helios Klinikum Berlin, Klinikum Buch, Nuklearmedizinische Klinik, Berlin, Germany
Background/Aims: To search for changes in body composition and energy metabolism associated with the repeatedly
observed weight gain of cirrhotic patients after portosystemic shunting.
Journal of Hepatology 40 (2004) 228–233
Weight gain after transjugular intrahepatic portosystemic shunt is
associated with improvement in body composition in malnourished
patients with cirrhosis and hypermetabolism
Mathias Plauth1,*, Tatjana Schu¨tz1, Deborah P. Buckendahl1, Georg Kreymann2,
Matthias Pirlich1, Sven Gru¨ngreiff1, Paul Romaniuk3, Siegfried Ertl4,
1Medizinische Klinik mit Schwerpunkt Gastroenterologie, Hepatologie und Endokrinologie, Charite´ Universita¨tsmedizin Berlin, Berlin, Germany
2Medizinische Klinik, Universita¨tsklinikum Hamburg Eppendorf, Hamburg, Germany3Institut fu¨r Ro¨ntgendiagnostik, Charite´ Univerista¨tsmedizin Berlin, Berlin, Germany
4Helios Klinikum Berlin, Klinikum Buch, Nuklearmedizinische Klinik, Berlin, Germany
Background/Aims: To search for changes in body composition and energy metabolism associated with the repeatedly
observed weight gain of cirrhotic patients after portosystemic shunting.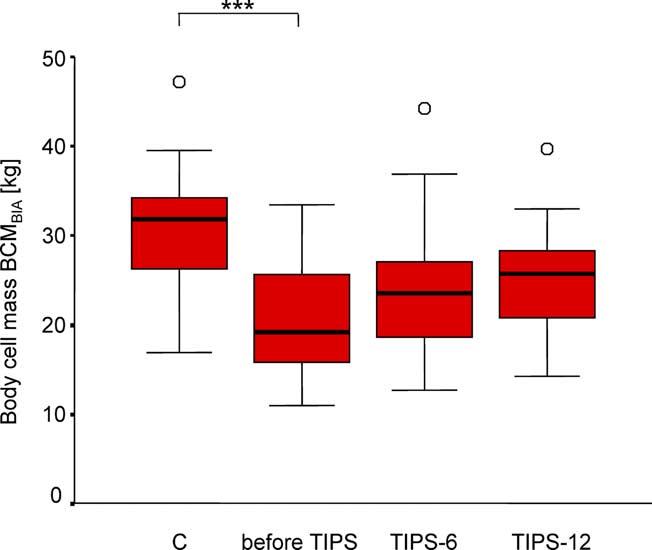 M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
Linear regression analysis based on the control group was used to calculatepredicted values for REE in the study population. Frequencies wereevaluated by the x2-test. Correction for multiple comparisons (6 and12 months after TIPS vs. before TIPS) was performed according toBonferroni with a probability level of less than 0.025 accepted asstatistically significant. Otherwise P , 0:05 was considered statisticallysignificant.
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
Linear regression analysis based on the control group was used to calculatepredicted values for REE in the study population. Frequencies wereevaluated by the x2-test. Correction for multiple comparisons (6 and12 months after TIPS vs. before TIPS) was performed according toBonferroni with a probability level of less than 0.025 accepted asstatistically significant. Otherwise P , 0:05 was considered statisticallysignificant.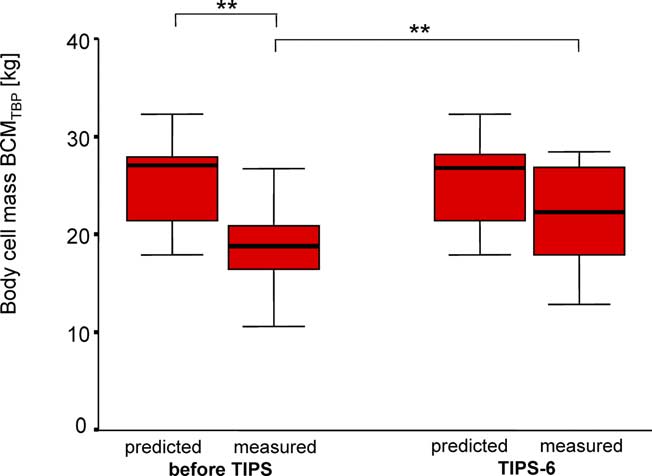
 M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
(P , 0:025). Measured REECALO remained higher thanpredicted values REEPRED at 6 months (1550 (1203 – 2364)vs. 1402 (1112 – 2000) kcal/d; P ¼ 0:001) and 12 months(1532 (1208 – 2232) vs. 1465 (1152 – 1868) kcal/d;P , 0:05) after TIPS, but the initial difference decreasedduring follow-up.
M. Plauth et al. / Journal of Hepatology 40 (2004) 228–233
(P , 0:025). Measured REECALO remained higher thanpredicted values REEPRED at 6 months (1550 (1203 – 2364)vs. 1402 (1112 – 2000) kcal/d; P ¼ 0:001) and 12 months(1532 (1208 – 2232) vs. 1465 (1152 – 1868) kcal/d;P , 0:05) after TIPS, but the initial difference decreasedduring follow-up.