Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Aeh154 865.869
British Journal of Anaesthesia 92 (6): 865±9 (2004)
DOI: 10.1093/bja/aeh154 Advance Access publication April 30, 2004
Medical aerosol propellant interference with infrared anaesthetic
The Department of Anesthesia and Critical Care Medicine, Hebrew University Hadassah School of
*Corresponding author: Department of Critical Care Medicine, Room B7 08, Sunnybrook and Women's College
Health Sciences Centre, 2075 Bayview Avenue, Toronto, Ontario M4N 3M5 Canada.
Background. 1,1,1,2 Tetra¯uoroethane is a hydro¯uoroalkane (HFA) that is replacing chloro-
¯uorocarbons (CFC) as a medical aerosol propellant in an attempt to reduce damage to the
ozone layer. This study compared the effects of HFA- and CFC-based inhalers on four anaes-
thetic gas monitoring systems. Methods. The HFA- and CFC-based inhalers were activated in close proximity to the sample
line of two Datex Ohmeda, an Agilent and a Siemens infrared anaesthetic agent monitoring sys-
tems. The effects were recorded on each system for ®ve common anaesthetic agents. Results. The HFA inhaler caused either maximal false positive readings (with the exception of
des¯urane) or transient measurement failure on all systems. The Datex Ohmeda AS/3 system
misidenti®ed the HFA inhaler as carbon dioxide at low concentration (2 T 0 mm Hg). The
CFC-based inhaler caused a minor false-positive reading (0.4 T 0%) for halothane only on the
Datex Ohmeda AS/3 system only and was misidenti®ed as carbon dioxide at 33.3 (SD 2.1) mm
Hg and 22.4 (8.9) mm Hg by the Agilent and Siemens systems. Conclusions. The HFA inhaler adversely affected all equipment tested. The infrared spectra
of HFA and the common anaesthetic gases have considerable overlap at the 8±12 mm range
that is not shared by the CFCs. The differences in spectral overlap explain the different effects
of the HFA and CFC propellants. Anaesthetic gas concentration data may be erroneous using
the HFA-based inhalers. Br J Anaesth 2004; 92: 865±9Keywords: anaesthesia; complications, inhalation anaesthesia; equipment, inhalers;
pharmacology, salbutamolAccepted for publication: February 11, 2004
In an attempt to decrease emission of substances that tionality associated with ozone depletion in the upper
cause damage to the ozone layer, the Montreal Protocol atmosphere. The change in propellant has led to some
of 1987 encouraged the cessation of use of chloro- minor changes in inhaler function (including smaller
¯uorocarbons (CFCs).1 A contribution to this effort has particle size for example2 3), but in general has not been
come from some pharmaceutical companies that have of clinical signi®cance.4±7 Following the observation that
changed the propellant in their inhaler medications. during anaesthesia the use of a salbutamol inhaler with
Propellants based on CFCs (such as di¯uorodichloro- the newer propellant led to a sudden rise in the
methane, mono¯uorotrichloroethane and tetra¯uorodi- anaesthetic agent measurement on the infrared gas
chloroethane) are being phased out and replaced with monitor (Fig. 1), this bench study set out to explore
more `ozone friendly' agents, including a hydro- and explain this phenomenon.
known as Nor¯urane, Dymelâ 134a/P and HFA 134a
(DuPont Fluorochemicals, Wilmington, DE, USA). This ²This study was performed with the assistance of internal departmental
substance does not contain the carbon±chlorine func- funding only.
Ó The Board of Management and Trustees of the British Journal of Anaesthesia 2004
Fig 1 Tracing of sevo¯urane concentration recorded from the anaesthetic agent monitor (Datex-Ohmeda AS/3) following release of two puffs of
salbutamol/HFA-based inhaler into the breathing circuit (arrow). The patient was being ventilated at a rate of 8 bpm, tidal volume 600 ml, fresh gas
¯ow 2 litre min±1; paper speed 12.5 mm s±1.
(North American Drager Narcomed GS, Drager Medical
An HFA-based inhaler (Salbutamol 100 mg per puff, Inc., USA), including the inhaler adaptor, was attached to a
Ventolin, GlaxoSmithKline, UK) and a CFC-based inhaler bag. The ventilator was set at a rate of 10 bpm, I:E ratio of
(ipratropium bromide 20 mg per puff, Aerovent, Teva 1:2 and tidal volume of 600 ml. The fresh gas ¯ow (using
Pharmaceutical Industries Ltd, Israel) were compared for air) was set sequentially at 2, 5 and 10 litre min±1. At each
their effects on four anaesthetic gas monitoring systems: the setting, one puff of the inhaler was released into the circuit.
Datex Ohmeda G-AO gas analyser with AS/3 monitor The inspiratory concentration of halothane for each breath
(Datex Ohmeda, Finland), the Datex Ohmeda M CAiOV that appeared on the monitor was recorded until the
gas analyser with the Datex Ohmeda S/5 monitor (Datex concentration dropped to zero. The zero measurement was
Ohmeda, Finland), the Hewlett Packard M1026A gas observed for at least 2 min, before a subsequent measure-
analyser with Agilent monitor (Agilent Patient Care ment series was made. Four series were performed at each
System, Andover, MA, USA) and the Siemens SC7000 fresh gas ¯ow setting. Results are presented as mean (SD).
ENG monitor and gas analyser (Siemens Medical Systems,
For both inhalers and all systems, the inhaler was Results
activated once into an open tube about 1.5 cm from the Each of the four systems examined responded in a different
open end of the sampling tube of the infrared gas monitoring manner to inhaler exposure. None of the systems responded
equipment. For the systems that employed automatic agent at all to the nebulized drugs. No false-positive readings were
identi®cation (Datex Ohmeda M CAiOV S/5, Siemens recorded for nitrous oxide.
SC7000 and Agilent/Hewlett Packard M1026A), this was
tested ®rst, starting from a situation where no anaesthetic
gas had been identi®ed. For the systems where the Datex Ohmeda systems
anaesthetic agent either could or had to be set manually The Datex Ohmeda AS/3 equipment does not have
(all systems besides the Datex Ohmeda M CAiOV S/5), the automated anaesthetic agent identi®cation, but does allow
system was tested when set to each of the gases to be tested user selection of each of the ®ve anaesthetic agents. When
(halothane, en¯urane, iso¯urane, sevo¯urane and des¯ur- set to all agents besides des¯urane, the HFA inhaler caused
ane). The starting anaesthetic concentration was allowed to a maximal graphical and numerical monitor reading
return to zero before commencing each measurement. The (the maximum being 15%). When set to des¯urane, the
peak concentration was recorded for both inhalers and for monitor's response was sub-maximum, reaching 28.1
each anaesthetic agent setting three times; in addition, a (0.1)%. In contrast, the CFC inhaler caused a response
descriptive record was made of the graphical representation only when the monitor was set to halothane, for which the
of agent measurement. The effect of the inhalers on end tidal monitor uses the highest gain (with a reading of 0.4 (0)%).
carbon dioxide measurement was also recorded.
The end tidal carbon dioxide response was similar for both
Nebulized solutions of salbutamol 2.5 mg and ipratro- inhalers: 2 (0) mm Hg. These results are summarized in
pium bromide 0.125 mg were also tested in all systems as a Table 1.
control to ascertain the effects of the drug substances in the
On testing the newer Datex Ohmeda S/5 with automated
gas identi®cation, if the system had not previously identi®ed
The time course of the interference effect of HFA 134a an anaesthetic gas, the HFA inhaler produced no response;
was also investigated. The monitor selected for this the CFC inhaler was identi®ed as halothane. If the monitor
investigation was the Datex Ohmeda AS/3, set to measure had previously identi®ed another anaesthetic gas, such as
halothane. The breathing circuit of an anaesthetic machine iso¯urane, the use of the HFA inhaler led to measurement
HFA interference with anaesthetic gas monitors
Table 1 Effect of inhaler propellant on gas analyser readings for the Datex AS/3 system. CFC, chloro¯uorocarbon; Max, maximal monitor reading (15%).
failure for up to a few seconds. This equipment does not
allow user selection of the anaesthetic agent. The effect on
the carbon dioxide measurements was similar to that
Hewlett Packard Agilent systemWhen started in the automatic agent identi®cation mode,
exposure to the HFA inhaler caused an initial downwards
de¯ection of the graph followed by measurement failure and
auto-zero of the anaesthetic agent, carbon dioxide and
oxygen measurements. No agent identi®cation was made.
The CFC inhaler had no effect at all. Similar results were
achieved when the monitor was set to each individual agent.
The HFA inhaler was not identi®ed as carbon dioxide, Fig 2 Time course for the effect of one puff from an HFA inhaler on the
anaesthetic agent monitor at three different fresh gas ¯ow rates. The
while the CFC inhaler caused a reading of 33.3 (2.1) mm Hg
inhaler was included in a breathing circuit connected to a ventilator and
Siemens systemExposure to the HFA inhaler caused a maximal de¯ection of described previously,8±10 but on less technologically
the graphic representation of all ®ve anaesthetic agents, advanced equipment in some cases.
transient measurement failure and subsequently unstable
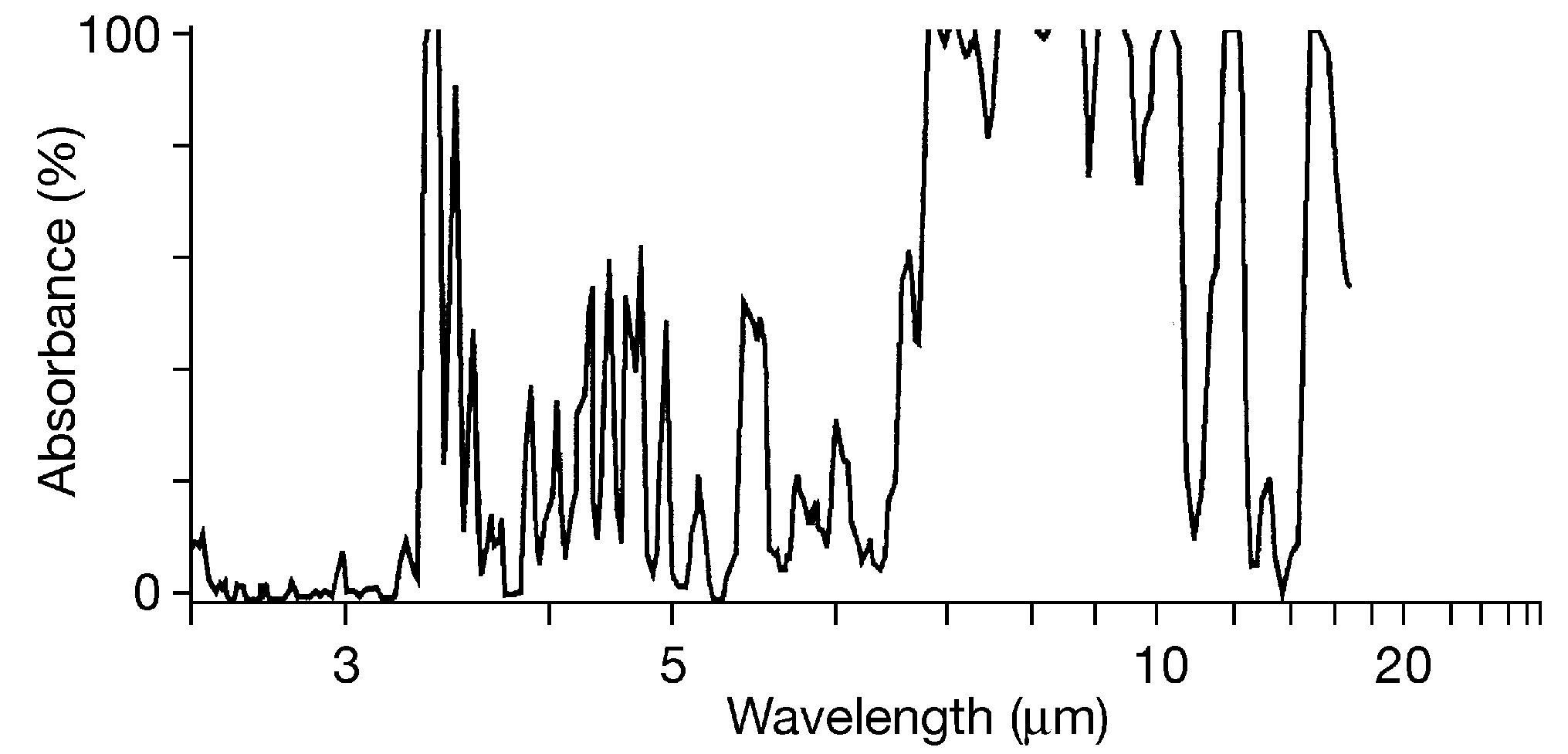
Modern infrared gas monitors function by measuring the
numerical readings until returning to zero. There was a absorption of infrared light by the sampled gas at up to ®ve
smaller response on the carbon dioxide tracing, without wavelengths in the 3.3 or 8±12 mm areas of the infrared
generation of a numerical value. No agent was identi®ed by spectrum and then solving a series of simultaneous equa-
the automatic agent identi®cation system.
tions to calculate the concentration of the anaesthetic agent
Exposure to the CFC inhaler had no effect on any of the or carbon dioxide. Multiple wavelengths are required in
gas measurements, but produced a marked effect on the order to distinguish between the different anaesthetic gases,
carbon dioxide measurement: 22.4 (8.9) mm Hg over ®ve and the 8±12 mm range is used as this represents the area of
the infrared spectrum where anaesthetic gases show max-
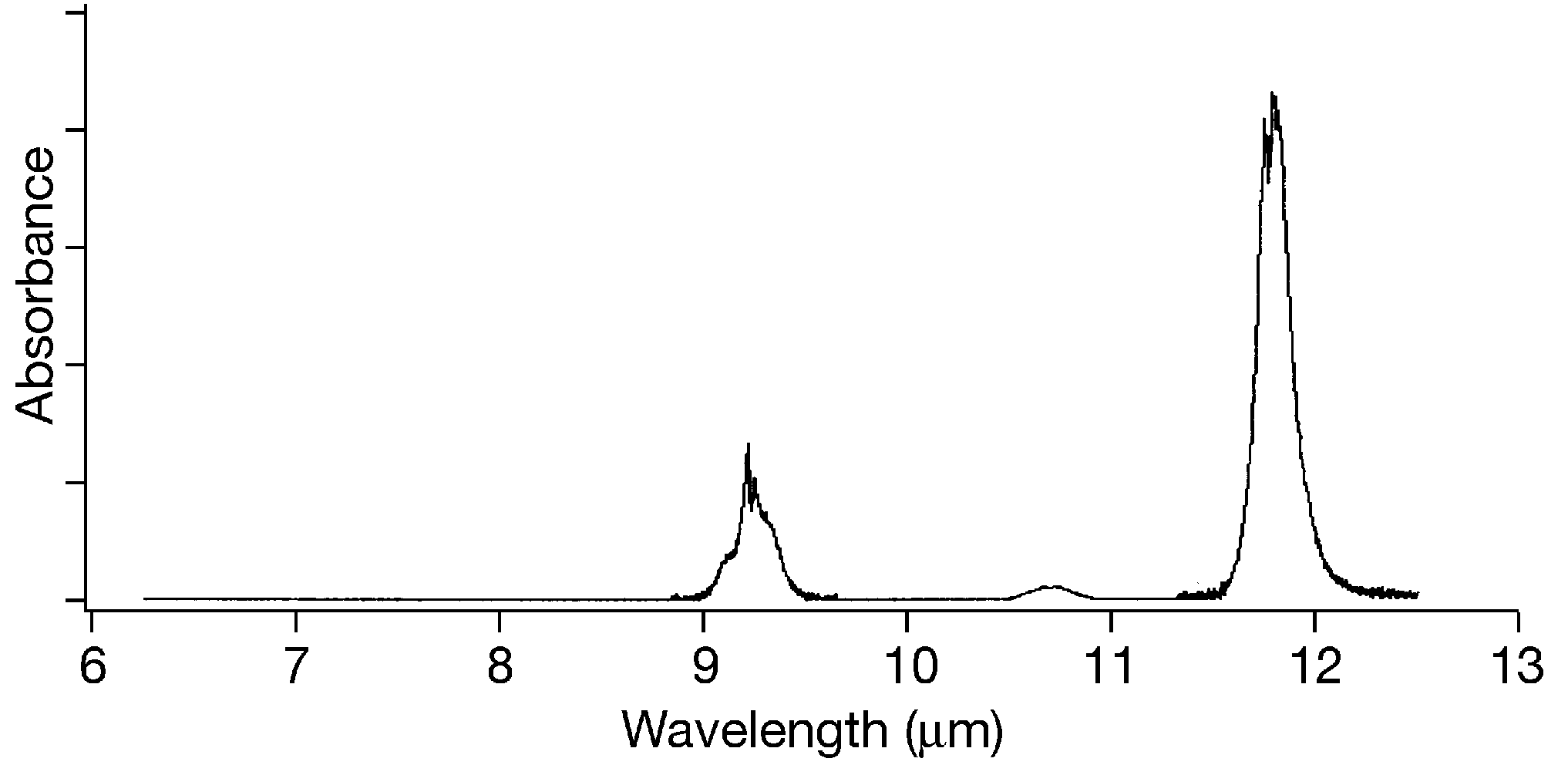
imum absorbance (Fig. 3). Figure 4 shows the infrared
absorbance spectrum of HFA 134a. As can be seen, HFA
134a demonstrates signi®cant infrared absorbance across
The time course for the effect of the HFA inhaler was the whole 8±12 mm wavelength range. This high absorbance
dependent on fresh gas ¯ow and is shown in Figure 2. The completely overlaps the peaks on the anaesthetic gas spectra
effect disappeared within ten breaths at all fresh gas ¯ow in the 8±12 mm range and presumably accounts for the
interference in monitoring function. In contrast, CFCs show
only isolated peaks of infrared absorption in the 8±12 mm
range,11 accounting for their lesser effect on anaesthetic gas
This study has shown that the HFA inhaler can cause short-
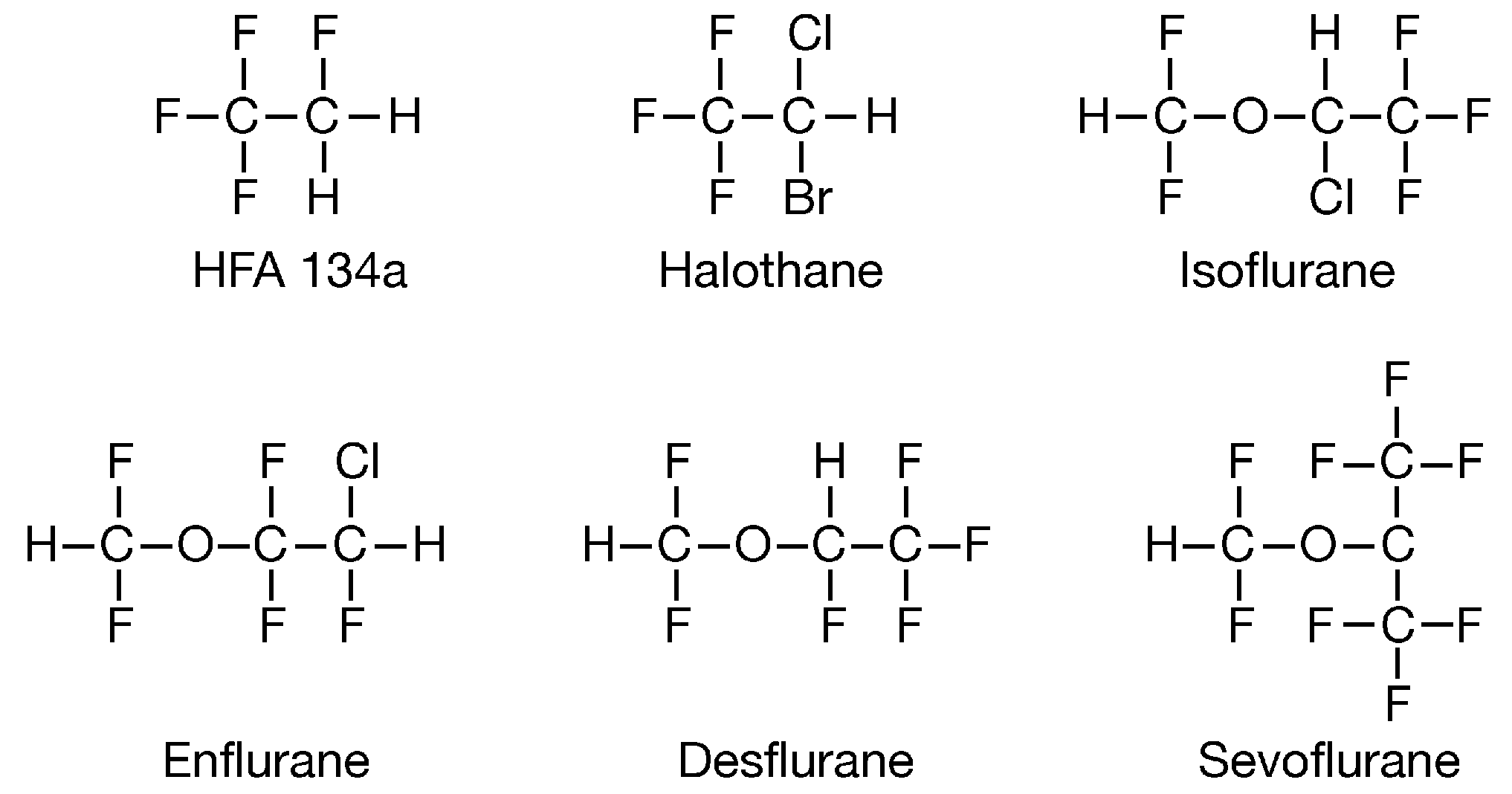
The similarities in absorption spectra between HFA 134a
lived, but clinically signi®cant, false-positive readings for and the anaesthetic gases can in part be predicted from the
all ®ve commonly used potent anaesthetic gases in various similarity in their molecular structure (Fig. 6), and from a
monitoring systems. These ®ndings are signi®cantly differ- historical point of view it is interesting to note that 1,1,1,2-
ent from those produced by a CFC-containing inhaler. The tetra¯uoroethane was tested as an anaesthetic agent in
small effect of CFCs on infrared gas monitors has been animals as early as 1967. It was found to have moderate
potency, requiring approximately 50 vol% to induce
anaesthesia,12 but was not developed for use in humans.
In doses associated with inhaler use, the propellant has been
shown to be safe and non-anaesthetic.13 14
HFA 134a is by no means unique in its ability to interfere
with infrared gas analysis. Many other gases (including
alcohol and methane for example) have been reported to
have similar effects,15±17 and monitoring technology has
been developed to overcome most of these interference
patterns. Salbutamol itself is not the cause of the inter-
Fig 3 Infrared absorption spectra for des¯urane, en¯urane and halothane.
ference described as: (i) nebulized salbutamol had no effect
Copyright Datex Ohmeda Division, Instrumentarium Corporation. Note
on the infrared analysis and (ii) salbutamol is an aerosol of
different x-axis scale in Figures 4 and 5.
®ne particles and not a gas and is therefore unlikely to affect
The methodology of this study was designed to maximize
the effect of the inhaler propellant on the infrared gas
monitors, the propellant being released almost directly into
the monitor sample line. As shown in Figures 1 and 2,
however, in clinical and simulated clinical situations, the
This study was performed to verify and explain the
clinical ®nding that, when administered to a patient, the
newer inhaler produced a sudden peak in the measured
anaesthetic concentration on infrared gas monitoring equip-
ment. The ®ndings above demonstrate that this change was
Fig 4 Infrared absorption spectrum for HFA 134a. Modi®ed with
likely to be due to the inhaler propellant and that an
permission from DuPont Fluorochemicals, Wilmington, DE, USA. Note
explanation for it can be found in the similarity of the
different x-axis scale in Figures 3 and 5.
infrared spectra between the propellant agent and the
2 Seale JP, Harrison LI. Effect of changing the ®ne particle mass of
inhaled beclomethasone dipropionate on intrapulmonary
deposition and pharmacokinetics. Respir Med 1998; 92 (Suppl
3 Leach CL, Davidson PJ, Boudreau RJ. Improved airway targeting
with the CFC-free HFA-beclomethasone metered-dose inhaler
compared with CFC-beclomethasone. Eur Respir J 1998; 12:
Fig 5 Infrared absorption spectrum of CFC-11. Adapted from reference
4 Langley SJ, Sykes AP, Batty EP, Masterson CM, Woodcock A. A
11. Note different x-axis scale in Figures 3 and 4.
comparison of the ef®cacy and tolerability of single doses of HFA
134a albuterol and CFC albuterol in mild-to-moderate asthmatic
patients. Ann Allergy Asthma Immunol 2002; 88: 488±93
5 Shapiro G, Bronsky E, Murray A, Barnhart F, VanderMeer A,
Reisner C. Clinical comparability of Ventolin formulated with
propellants in children with asthma. Arch Pediatr Adolesc Med
6 Huchon G, Hofbauer P, Cannizzaro G, Iacono P, Wald F.
Comparison of the safety of drug delivery via HFA- and
CFC-metered dose inhalers in CAO. Eur Respir J 2000; 15:
7 Dahl R, Ringdal N, Ward SM, Stampone P, Donnell D.
Equivalence of asthma control with new CFC-free formulation
Fig 6 Chemical structures of HFA 134a and common volatile
beclomethasone dipropionate. Br J Clin Pract 1997; 51: 11±15
8 Bickler PE, Yung JS. Mass spectrometers and infrared gas
HFA interference with anaesthetic gas monitors
analysers interpret bronchodilator propellants as anaesthetic
13 Dekant W. Toxicology of chloro¯uorocarbon replacements.
gases. Letter to the editor. Anesth Analg 1992; 75: 142±3
Environ Health Perspect 1996; 104 (Suppl 1): 75±83
9 Elliot WR, Raemer DB, Goldman DB, Philip JH. The effects of
14 Emmen HH, Hoogendijk EM, Klopping-Ketelaars WA, et al.
bronchodilator-inhaler aerosol propellants on respiratory gas
Human safety and pharmacokinetics of the CFC alternative
propellants HFC 134a (1,1,1,2-tetra¯uoroethane) and HFC 227
10 Woehlck HJ, Dunning M 3rd, Kulier AH, Sasse FJ, Nithipataikom
K, Henry DW. The response of anaesthetic agent monitors to
exposure. Regul Toxicol Pharmacol 2000; 32: 22±35
tri¯uoromethane warns of the presence of carbon monoxide
15 Moens YP, Gootjes P. The in¯uence of methane on the infrared
from anaesthetic breakdown. J Clin Monit 1997; 13: 149±55
measurement of anaesthetic vapour concentration. Anaesthesia
11 http://www.nist.gov/kinetics/spectra/ir_spectra/ir_data_®le/
16 Morrison JE, McDonald C Erroneous data from an infrared
12 Shulman M, Sadove MS. 1,1,1,2-Tetra¯uoroethane: an inhalation
anaesthetic gas analyzer. J Clin Monit 1993; 9: 293±4
anaesthetic agent of intermediate potency. Anesth Analg 1967;
17 Guyton DC, Gravenstein N. Infrared analysis of volatile
anaesthetics: impact of monitor agent setting, volatile mixtures,
and alcohol. J Clin Monit 1990; 6: 203±6
THE HIGHLAND COUNCIL Resources Committee – 5th October 2005 Report by Director of Corporate Services Smoking Cessation Support in Support of the Policy on Managing Smoking at Work Summary This report proposes that smoking cessation support be made available for elected members and staff in support of the policy on Managing Smoking at Work. Introduction It was agree
 British Journal of Anaesthesia 92 (6): 865±9 (2004)
DOI: 10.1093/bja/aeh154 Advance Access publication April 30, 2004
Medical aerosol propellant interference with infrared anaesthetic
The Department of Anesthesia and Critical Care Medicine, Hebrew University Hadassah School of
*Corresponding author: Department of Critical Care Medicine, Room B7 08, Sunnybrook and Women's College
Health Sciences Centre, 2075 Bayview Avenue, Toronto, Ontario M4N 3M5 Canada.
British Journal of Anaesthesia 92 (6): 865±9 (2004)
DOI: 10.1093/bja/aeh154 Advance Access publication April 30, 2004
Medical aerosol propellant interference with infrared anaesthetic
The Department of Anesthesia and Critical Care Medicine, Hebrew University Hadassah School of
*Corresponding author: Department of Critical Care Medicine, Room B7 08, Sunnybrook and Women's College
Health Sciences Centre, 2075 Bayview Avenue, Toronto, Ontario M4N 3M5 Canada.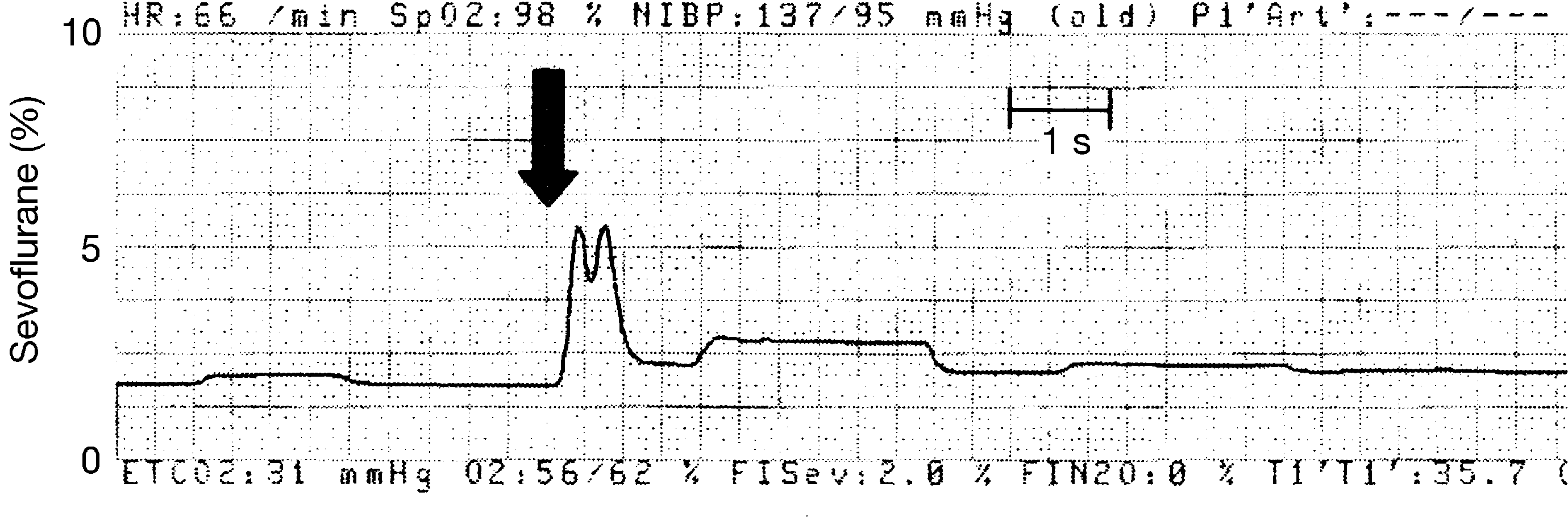 Fig 1 Tracing of sevo¯urane concentration recorded from the anaesthetic agent monitor (Datex-Ohmeda AS/3) following release of two puffs of
salbutamol/HFA-based inhaler into the breathing circuit (arrow). The patient was being ventilated at a rate of 8 bpm, tidal volume 600 ml, fresh gas
¯ow 2 litre min±1; paper speed 12.5 mm s±1.
Fig 1 Tracing of sevo¯urane concentration recorded from the anaesthetic agent monitor (Datex-Ohmeda AS/3) following release of two puffs of
salbutamol/HFA-based inhaler into the breathing circuit (arrow). The patient was being ventilated at a rate of 8 bpm, tidal volume 600 ml, fresh gas
¯ow 2 litre min±1; paper speed 12.5 mm s±1.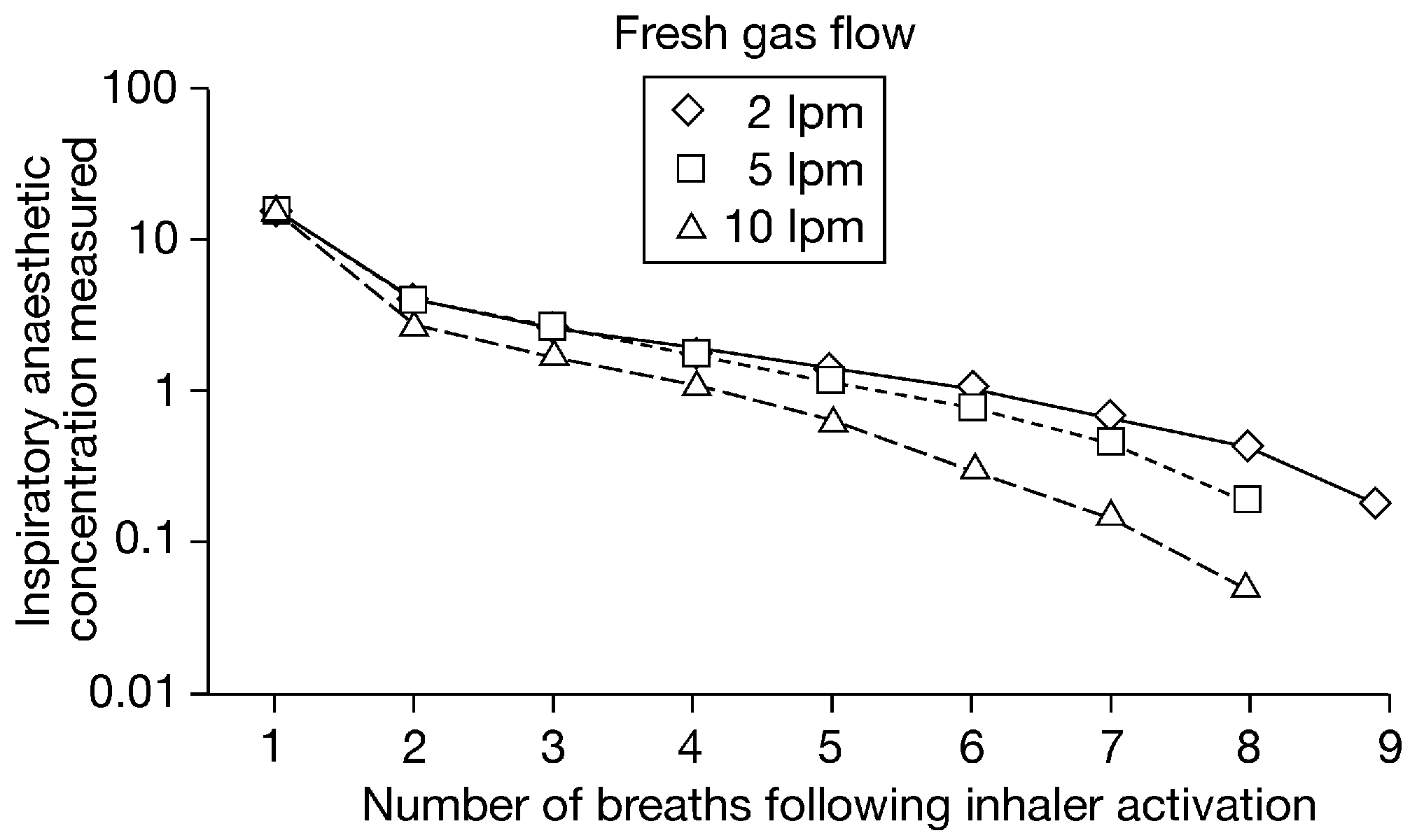 HFA interference with anaesthetic gas monitors
Table 1 Effect of inhaler propellant on gas analyser readings for the Datex AS/3 system. CFC, chloro¯uorocarbon; Max, maximal monitor reading (15%).
HFA interference with anaesthetic gas monitors
Table 1 Effect of inhaler propellant on gas analyser readings for the Datex AS/3 system. CFC, chloro¯uorocarbon; Max, maximal monitor reading (15%).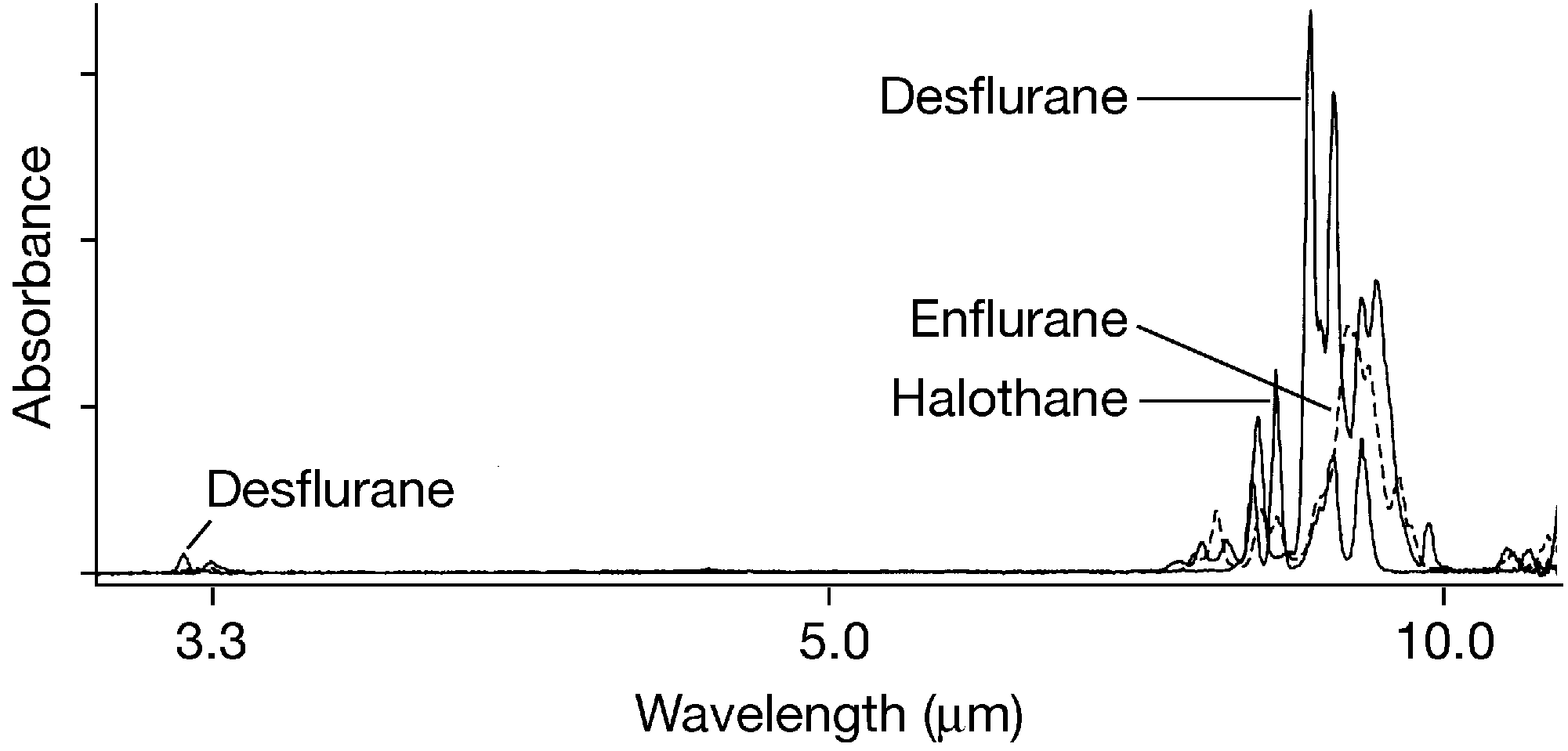
 potency, requiring approximately 50 vol% to induce
anaesthesia,12 but was not developed for use in humans.
potency, requiring approximately 50 vol% to induce
anaesthesia,12 but was not developed for use in humans.