British Journal of Anaesthesia 1998; 81: 444–448 Antibacterial activity of lidocaine in mixtures with Diprivan
R. J. GAJRAJ, M. J. HODSON, J. A. GILLESPIE, G. N. C. KENNY AND N. B. SCOTT
of a range of organisms to lidocaine; the concentra-
tions of lidocaine required for bactericidal and bacte-
We have studied the antibacterial activity of dif-
riostatic effects; and the antibacterial effects of
ferent concentrations of 0.005–2% lidocaine (lig-
clinically used concentrations of lidocaine.
nocaine) in mixtures with Diprivan (propofol), against micro-organisms commonly implicated in sepsis as a result of extrinsically contaminated
Diprivan. Bacterial colony counts were reduced
Test mixtures of lidocaine and Diprivan were inocu-
progressively with increasing concentrations of
lated with suspensions of organisms, and colonies
lidocaine. Bacteriostatic and bactericidal concen-
were counted from samples of the inoculated suspen-
trations of lidocaine were 0.2–2%. Lidocaine 2%
sions after a period of incubation. The organisms
was not bactericidal for one of the seven organ-
used were clinical (hospital) isolates (CI) or standard-
isms tested. By inhibiting bacterial replication,
ized typed organisms from the National Collection of
lidocaine, when added to Diprivan to reduce pain
Typed Cultures (NCTC) as follows: Staphylococcus
on injection, may possibly reduce the harmful
(S.) aureus (NCTC 6571), S. epidermidis (coagulase-
consequences if extrinsic contamination occurs.
negative staphylococcus—NCTC 7944), Bacillus (B.)
(Br. J. Anaesth. 1998; 81: 444–448). subtilis (NCTC 10452), Escherichia (E.) coli (NCTC 10418), Moraxella (M.) osloensis (NCTC 10465),
Keywords: anaesthetics local, lidocaine; anaesthetics i.v.,
Serratia (S.) marcescens (CI) and Burkholderia (B.)
propofol; infection, bacterial; formulations, propofol; formu- lations, concentration
The lidocaine–Diprivan test mixtures (5.25 ml)
were prepared under aseptic conditions. The quan-
The lipid-based i.v. drugs Diprivan (propofol)1 2 and
tity of lidocaine in the mixtures ranged from 0.25 ml
Diazemuls (diazepam)3 have been shown to support
of 0.1% to 5.25 ml of 2%, producing a range of lido-
growth of micro-organisms at room temperature.
caine concentrations of 0.005–2%. Diprivan was the
Most other i.v. anaesthetics are not lipid-based, and
diluent used when preparing the lower concentra-
studies have confirmed that they do not support
tions of lidocaine. A sample of 1% Diprivan 5.25 ml
As a result, there is concern that infusion of
Suspensions of the bacteria diluted to a Bacto
Diprivan may contribute to an increased incidence of
McFarland Barium Sulfate Standard Number 1
postoperative infections. Investigators for the
(measured by a Vitek colorimeter), equivalent to
Centers for Disease Control (CDC) in the USA
found that in some cases of postoperative sepsis, the
millilitre, were prepared. Standardized suspensions
organism isolated from infected patients was the
containing approximately 105 cfu ml91 were made by
same as that cultured from the throat or hands of the
serial dil ution with 0.9% sal ine. The test mixtures
anaesthetic personnel involved, or from syringes of
were inoculated with 50-l samples of the standard
Diprivan that had been used in these patients.6 7
suspensions of organisms to produce a final concen-
Organisms implicated in postoperative sepsis caused
tration of approximately 103 cfu ml91. These inocu-
by administration of contaminated Diprivan include
lated test mixtures were incubated at 37ЊC for 24 h.
Staphylococcus (S.) aureus, Klebsiella pneumoniae,
After this initial incubation, 100-l sampl es were
Moraxella (M.) osloensis, Enterobacter agglomerans,
obtained from each culture and from serial dilutions
Serratia (S.) marcescens and Candida albicans.6–8
of each culture, and added to blood agar plates for
It is wel l known that Diprivan is associated with
another 24 h of incubation at 37ЊC. After this second
pain on injection.9 10 Of the many drugs and tech-
period of incubation, the resulting colony counts
niques used to reduce the incidence of pain, only
aspirin11 and local anaesthetics11–13 have demonstrable antimicrobial activity. The exact mechanism of the
R. J. GAJRAJ, DM, FRCA, Department of Anaesthesia, The General Infirmary at Leeds, Leeds. M. J. HODSON, FRCA, Department of
antimicrobial action of local anaesthetics is not
Anaesthesia, Southern General Hospital, Glasgow. J. A. GILLESPIE,
known, but may be caused by an effect on microbial
FRCA, Department of Anaesthesia, Victoria Infirmary, Glasgow.
cell membrane structure or function,11 14 15 or pH
G. N. C. KENNY, BSC (HONS), MD, FRCA, University Department of
Anaesthesia, Royal Infirmary, Glasgow. N. B. SCOTT, FRCS, FRCA, Department of Anaesthesia, HCI International Medical Centre,
The aims of this study were to investigate further
Beardmore Street, Clydebank G81 4HX. Accepted for publication:
the antibacterial activity of lidocaine (lignocaine) in
mixtures with Diprivan to determine: the susceptibility
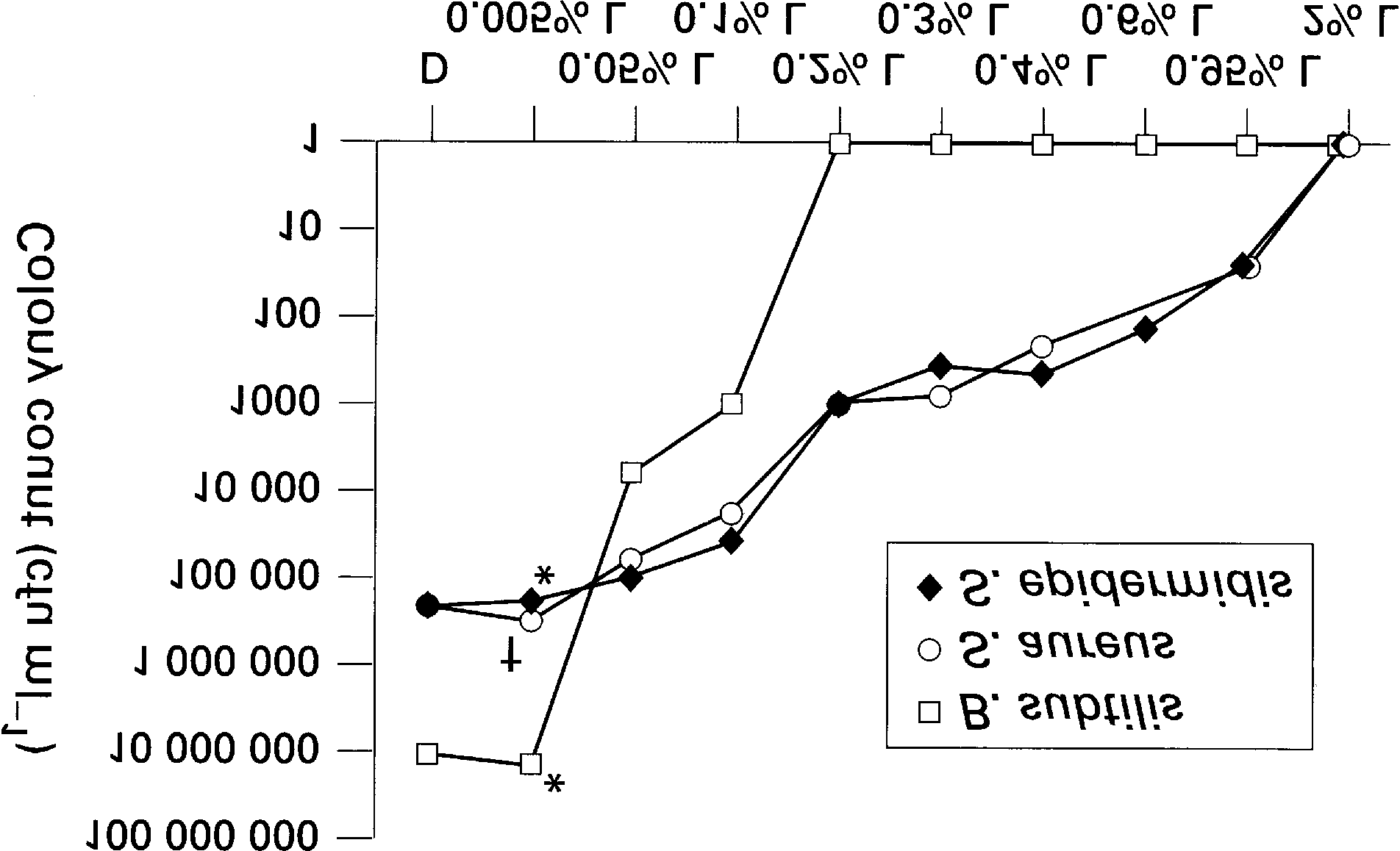
Antibacterial activity of lidocaine in Diprivan Figure 2 Colony counts for gram-positive bacteria (B. subtilis, S. aureus and S. epidermidis) after 24 h of incubation in Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony
counts higher (Mood Median test, P:0.05) than colony counts in Diprivan; *colony counts not significantly lower (Mood Median
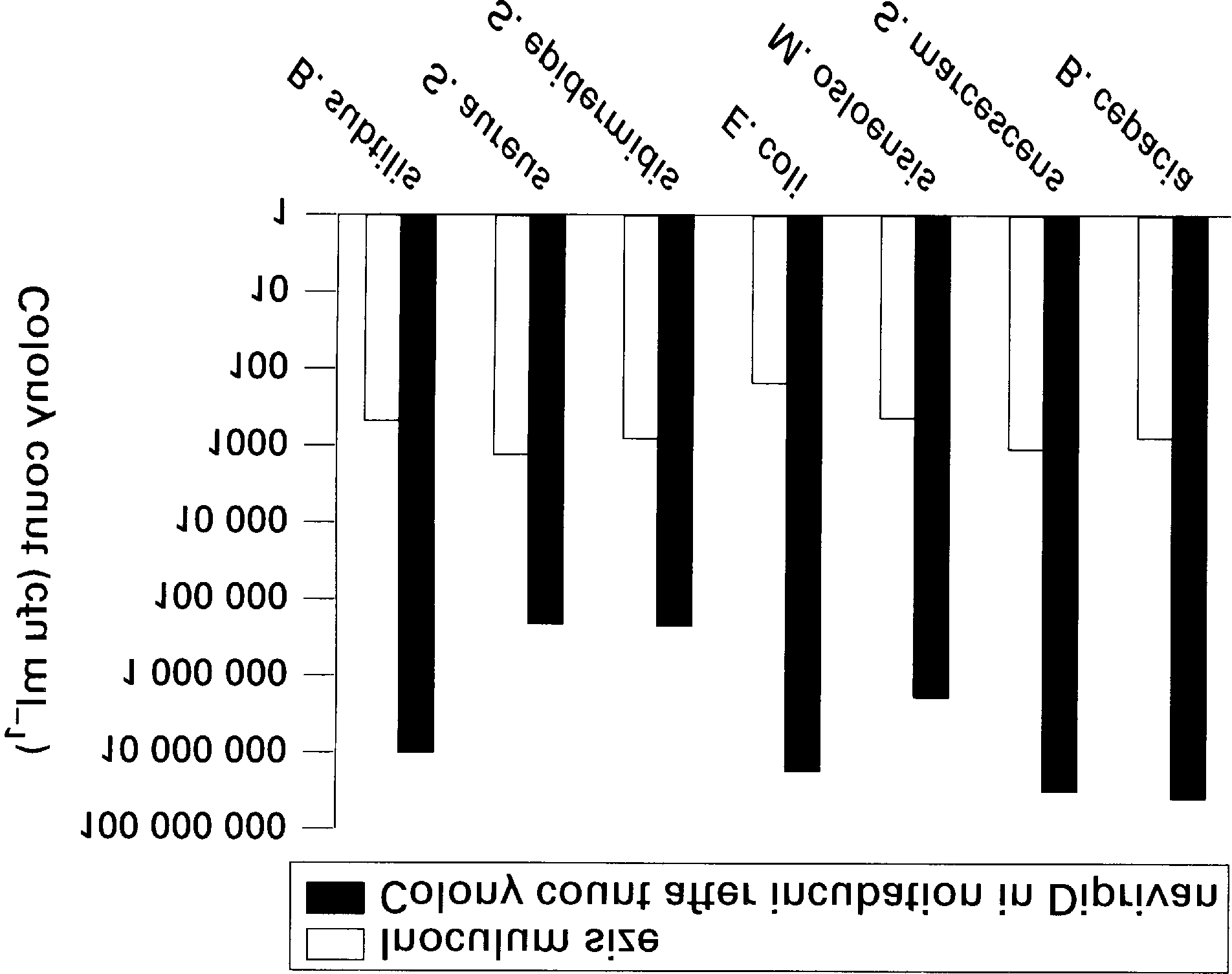
Figure 1 Inoculum sizes (colony counts at 0 h) and colony counts
test, P:0.05) than colony counts in Diprivan.
after 24 h of incubation in Diprivan for gram-positive and gram- negative bacteria.
organisms had significantly lower colony counts in
For a more precise measurement of the inoculum
lidocaine concentrations of 0.05% or higher, com-
size and to verify growth and viability of the organ-
pared with counts in propofol alone (fig. 2). All gram-
isms, 0.9% saline 5.25 ml was also inoculated with
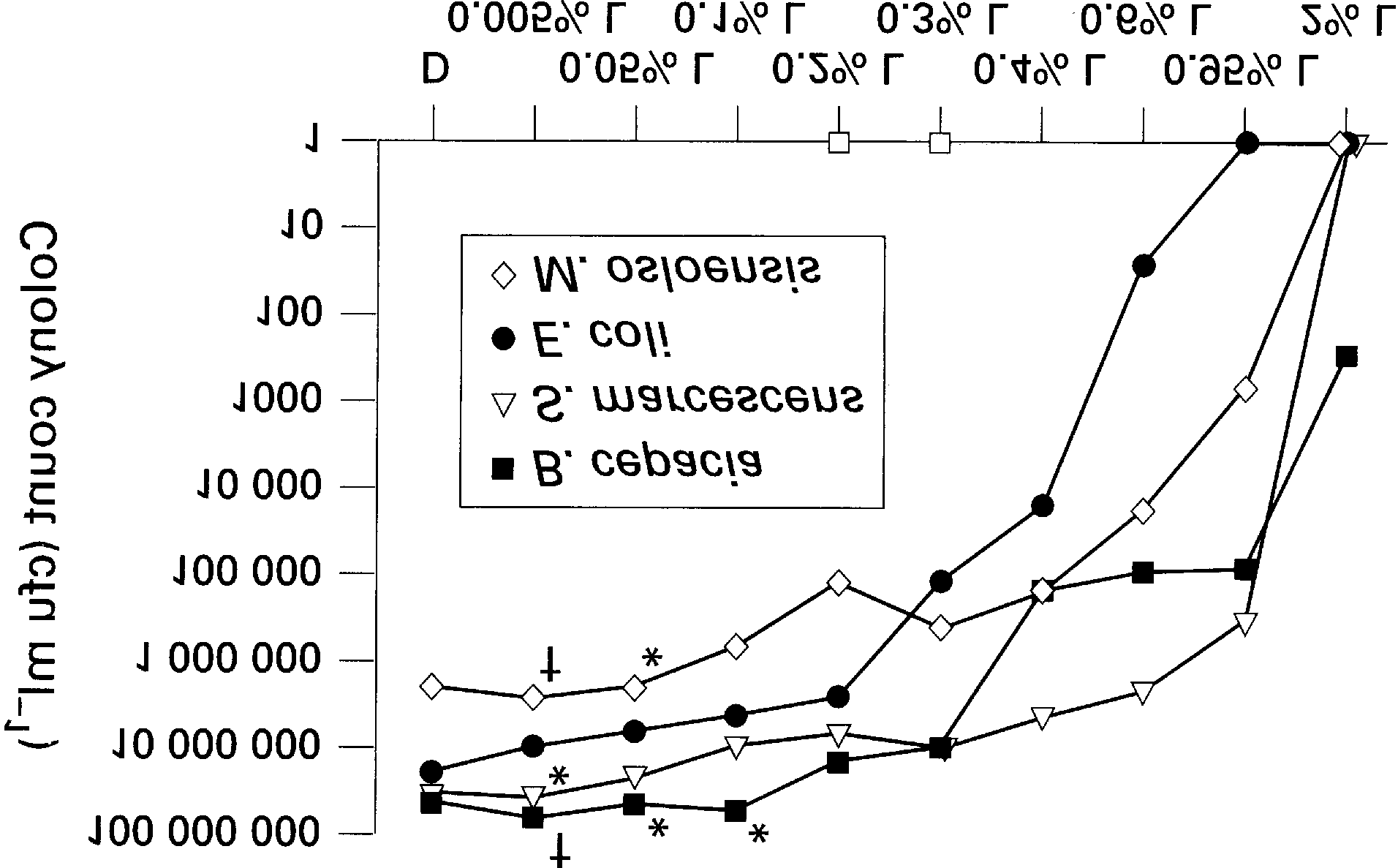
negative organisms had significantly lower colony
50 l of the standard suspensions of each bacterium
counts in lidocaine concentrations of 0.2% or higher,
to produce the same final concentration (103 cfu ml91)
compared with counts in propofol alone (fig. 3).
as the test mixtures. Samples of 100 l from this
The recommended dose of lidocaine 10 mg in
growth control were then added to Columbia blood
Diprivan 20 ml (producing a concentration of almost
agar plates and colony counts recorded after incuba-
0.05%) produced significantly lower colony counts
tion for 24 h at 37ЊC. To verify sterility, samples from
compared with colony counts in propofol alone, for
the sources of Diprivan, lidocaine and 0.9% saline
all except two organisms (table 1; figs 1, 2).
were also incubated for 24 h at 37ЊC, and added to
Lidocaine 0.1% (20 mg in Diprivan 20 ml) produced
blood agar plates for colony counts after another 24 h
significantly lower colony counts for all except one
For each organism a bactericidal effect was defined
Figure 4 demonstrates the bacteriostatic and bac-
as the killing (or 99.9% elimination) of the initial
tericidal concentrations of l idocaine for the organ-
inoculum, and a bacteriostatic effect as the preven-
isms tested. Lidocaine 0.2% was bacteriostatic for all
tion of growth, that is no significant change in viable
of gram-positive organisms. Bacteriostatic concen-
count from the initial inoculum.17 Three replicates
trations of lidocaine were 0.6–2% for the gram-nega-
were performed with each organism to complete the
tive organisms. Bactericidal concentrations were
0.2–2% for gram-positive organisms and 0.95–2%
for gram-negative organisms. Bactericidal concentra-
Windows) was used to compare the colony counts of
tion was not determined for B. cepacia, as growth of
each organism in each mixture of l idocaine and
this organism persisted at the highest concentration
Diprivan, with P:0.05 considered significant.
The final concentrations of the organisms after inoculation in Diprivan–lidocaine mixtures were 160–1350 cfu ml91. Figure 1 demonstrates the differ- ent rates of growth of the various organisms in Diprivan, most notable with S. aureus, which was the largest inoculum used yet had the lowest colony counts after 24 h of incubation in Diprivan. Figures 2 and 3 illustrate the colony counts of the gram- positive and gram-negative organisms after 24 h of incubation in the Diprivan–lidocaine mixtures.
With few exceptions, there was a progressive
reduction in colony counts of all organisms with increasing concentration of lidocaine (figs 2, 3).
Comparing colony counts in the lowest concentra-
Figure 3 Colony counts of gram-negative bacteria (B. cepacia,
tion of lidocaine (0.005%) with colony counts in
S. marcescens, E. coli and M. osloensis) after 24 h of incubation in
propofol alone, only one organism had significantly
Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony counts higher (Mood Median test, P:0.05) than colony
lower counts (E. coli) while three organisms had
counts in Diprivan; *colony counts not significantly lower (Mood
significantly higher colony counts. All gram-positive
Median test, P:0.05) than colony counts in Diprivan.
Table 1 Colony counts of gram-positive and gram-negative bacteria after 24 h of incubation in Diprivan and in mixtures of lidocaine (L) and Diprivan. The Mood Median test (P:0.05) was used to compare colony counts. Lidocaine–Diprivan mixtures with colony counts that were not significantly lower (ns) than the corresponding colony counts in Diprivan alone are indicated
Discussion
greater than 0.1 mg kg91.30 This dose of lidocaine (0.1 mg kg91) would be achieved with the manufac-
Postoperative immunosuppression is well recog-
turer’s recommended dose of 10 mg. However, other
nized18–20 and there is also concern that administration
studies have reported that larger doses of lidocaine
of contaminated infusions of Diprivan may contribute
are more effective.31–33 In several hundred anaesthet-
to an increased incidence of postoperative infections.
ics at our institution, one of the authors (N. B. S.) has
Unfortunately, poor aseptic technique is common-
used lidocaine in doses of at least 20 mg in Diprivan
place among health care workers in the hospital envi-
20 ml, and we are unaware of any clinical problems
ronment,21 22 and there is poor compliance with data
related to this practice. Further, Lilley and colleagues
sheet recommendations for the use of Diprivan.7 This
suggested that clinically significant emulsion instability
problem is so great that it led the authors of the CDC
does not occur when l idocaine 20 mg is added to
report7 and the accompanying editorial23 to suggest
restriction of the use of Diprivan to personnel prop-
In our study, the manufacturer’s recommended
erly educated in the aseptic techniques of handling
dose of 0.05% lidocaine was not bacteriostatic or
the drug. As there is a delay of 8 h or more before
bactericidal for any of the organisms tested, although
organisms begin to multiply rapidly when inoculated
there were significantly reduced colony counts for
into Diprivan, Langevin and colleagues24 disputed
al l gram-positive organisms and two of the gram-
the conclusions of the CDC report6 that simple bac-
negative organisms. Colony counts were reduced
terial replication in contaminated Diprivan results in
further with 0.1% lidocaine (equivalent to lidocaine
postoperative infections. Others have suggested that
20 mg in Diprivan 20 ml), but 0.2% was the lowest
by careful aseptic handl ing, it is possibl e to use the
concentration of lidocaine with bacteriostatic effects.
drug in multiple patients or long after opening the
The bacteriostatic concentration of lidocaine
ampoule, without significant risk of contamina-
against S. aureus was found to be lower in this study
than that reported in some studies34 35 but higher than
The manufacturers recommend the addition of
in others.36 The potency of l idocaine against E. coli
lidocaine 10 mg to Diprivan 20 ml (approximately
reported in some studies34 35 was similar to the find-
0.05% lidocaine) for the relief of pain on injection,28
ings of our study, but greater than in others.15 37 The
as there may be problems of chemical incompatibility
potency of lidocaine against S. marcescens and
with larger doses.29 Gehan and colleagues suggested
M. osloensis in one study35 was greater than that in our
that there was no additional improvement in reduc-
study. Fazly Bazaz and Salt concluded that the
ing the pain of injection with lidocaine in doses
antibacterial activity of lidocaine was greater against gram-positive than against gram-negative organisms.15 This is consistent with the findings of our study but contrary to those of Schmidt and Rosenkranz35 who investigated more than 1200 strains of bacteria and fungi and showed greater antibacterial activity against gram-negative organisms. These inconsisten- cies may be a result of differences in methodology34 or pH,16 presence of preservatives in the local anaes- thetic preparations,34 37 different serotypes of organ- isms tested,35 type of growth medium used38 and size of the initial inoculum.17
The size of the initial inoculum is an important
factor that influences determination of antimicrobial potency.17 This should ideally be between 4
106 bacteria per sample.39 40 The use of larger inoc-
ula may result in erroneously low antibacterial activ- ity because of the inclusion of spontaneously resistant bacteria,41 while measurement of Ն99.9%
Figure 4 Bacteriostatic and bactericidal concentrations of
killing for determination of bactericidal concentra-
lidocaine for various gram-positive and gram-negative bacteria.
tions may not be possible with insufficient colonies
The bactericidal concentration for Burkholderia (B.) cepacia was not determined.
from small inocula.39 The inoculum size used in our
Antibacterial activity of lidocaine in Diprivan
study was large enough to determine Ն99.9% killing
11. Ohsuka S, Ohta M, Masuda K, Arakawa Y, Kaneda T, Kato N.
for only two of the organisms tested. Therefore, for
Lidocaine hydrochloride and acetylsalicylate kill bacteria by disrupting the bacterial membrane potential in different ways.
the other five organisms, we considered a bactericidal
Microbiology and Immunology 1994; 38: 429–434.
effect to be present when there was complete elimi-
12. Jonnesco T. Remarks on general spinal analgesia. British
nation of bacteria (100% killing). It should be noted
Medical Journal 1909; 2: 1396–1401.
that the degree of killing of the initial inoculum con-
13. Erlich H. Bacteriologic studies and effects of anesthetic solu-
sidered representative of bactericidal activity has
tions on bronchial secretions during bronchoscopy. American Review of Respiratory Diseases 1961; 84: 414–421.
been reported as 998% to 100% by others, although
14. Silva MT, Sousa JC, Polonia JJ, Macedo PM. Effects of local
anesthetics on bacterial cells. Journal of Bacteriology 1979;
Further studies may be useful in determining if
137: 461–468.
other local anaesthetic agents, such as procaine and
15. Fazly Bazaz BS, Salt WG. Local anaesthetics as antimicrobial
agents: structure–action considerations. Microbios 1983; 37:
prilocaine, are more effective than lidocaine as
antimicrobial agents at doses that are useful for
16. Thompson KD, Welykyj S, Massa MC. Antibacterial activity
preventing pain on injection caused by Diprivan.
of lidocaine in combination with a bicarbonate buffer. Journal
Studies may then be necessary to investigate if the
of Dermatologic Surgery and Oncology 1993; 19: 216–220.
emulsion is stable when the local anaesthetics are
17. Wol fson JS, Swartz MN. Drug therapy. Serum bactericidal
activity as a monitor of antibiotic therapy. New England
mixed with Diprivan at the effective antimicrobial
Journal of Medicine 1985; 312: 968–975.
concentrations. Although Weinstein and colleagues34
18. White IW, Gelb AW, Wexler HR, Stiller CR, Keown PA. The
found prilocaine and procaine, in common with lido-
effects of intravenous anaesthetic agents on human neutrophil
caine, to be weak antimicrobial agents in comparison
chemiluminescence. Canadian Anaesthetists Society Journal 1983; 30: 506–511.
with other local anaesthetics, other studies found
19. Bardosi L, Tekeres M. Impaired metabolic activity of phago-
procaine35 37 and prilocaine37 to be more potent than
cytic cells after anaesthesia and surgery. British Journal of Anaesthesia 1985; 57: 520–523.
Strict adherence to the manufacturer’s recommen-
20. Madsbad S, Buschard K, Siemssen O, Ropke C. Changes in
dations is the most rel iabl e method for preventing
T-lymphocyte subsets after elective surgery. Acta Chirurgica Scandinavica 1986; 152: 81–84.
postoperative sepsis caused by administration of
21. Harrison CA, Rogers DW, Rosen M. Blood contamination of
contaminated Diprivan. However, by inhibiting the
anaesthetic and related staff. Anaesthesia 1990; 45: 831–833.
growth of bacteria, lidocaine in the doses used to
22. O’Donnell NG, Asbury AJ. The occupational hazard of
prevent pain on injection may help to limit the conse-
human immunodeficiency virus and hepatitis B virus infec- tion. I. Perceived risks and preventive measures adopted by
quences if bacterial contamination of Diprivan
anaesthetists: a postal survey. Anaesthesia 1992; 47: 923–928.
23. Nichols RL, Smith JW. Bacterial contamination of an anes-
thetic agent. New England Journal of Medicine 1995; 333: 184–185. Acknowledgements
24. Langevin PB, Gul ig PA, Gravenstein N, Langevin SO. A
re-evaluation of the growth rate of Staphylococcus aureus in
We thank Mr Brian Wilson, Mr Jim Lamb and Dr Giles Edwards
propofol and intralipid: implications on infection. Anesthesia and Analgesia 1995; 80: S263.
25. Downs GJ, Hal ey PR, Parent JB. Propofol : can a singl e
References
ampule be used for multiple patients? Anesthesiology 1991; 74: 1156–1157.
1. Arduino MJ, Bland LA, McAllister SK, Aguero SM, Villarino
26. Farrington M, McGinnes J, Matthews I, Park GR. Do
ME, McNeil MM, Jarvis WR, Favero MS. Microbial growth
infusions of midazolam and propofol pose an infection risk to
and endotoxin production in the intravenous anesthetic
critically ill patients? British Journal of Anaesthesia 1994; 72:
propofol. Infection Control and Hospital Epidemiology 1991; 12:
27. Warwick JP, Blake D. Drawing up propofol. Anaesthesia 1994;
2. Tessl er M, Dascal A, Gioseffini S, Mil l er M, Mendel son J.
Growth curves of Staphylococcus aureus, Candida albicans, and
28. Diprivan 1%. In: Walker G, ed. ABPI Data Sheet Compendium Moraxella osloensis in propofol and other media. Canadian 1995–96. London: Datapharm Publications Ltd, 1995;
Journal of Anaesthesia 1992; 39: 509–511.
3. Berry CB, Gillespie T, Hood J, Scott NB. Growth of micro-
29. Lilley EMM, Isert PR, Carasso ML, Kennedy RA. The effect
organisms in solutions of intravenous anaesthetic agents.
of the addition of lignocaine on propofol emulsion stability.
Anaesthesia 1993; 48: 30–32. Anaesthesia 1996; 51: 815–818.
4. Highsmith AK, Greenhood GP, Allen JR. Growth of nosoco-
30. Gehan G, Karoubi P, Quinet F, Leroy A, Rathat C, Pourriat
mial pathogens in multiple-dose parenteral medication vials.
JL. Optimal dose of lignocaine for preventing pain on injec-
Journal of Clinical Microbiology 1982; 15: 1024–1028.
tion of propofol. British Journal of Anaesthesia 1991; 66:
5. Sosis MB, Braverman B. Growth of Staphylococcus aureus in
four intravenous anesthetics. Anesthesia and Analgesia 1993;
31. Johnson RA, Harper NJ, Chadwick S, Vohra A. Pain on injec-
77: 766–768.
tion of propofol. Methods of alleviation. Anaesthesia 1990; 45:
6. Postsurgical infections associated with an extrinsically conta-
minated intravenous anesthetic agent—California, Illinois,
32. King SY, Davis FM, Wells JE, Murchison DJ, Pryor PJ.
Maine, and Michigan, 1990. MMWR—Morbidity and
Lidocaine for the prevention of pain due to injection of propo-
Mortality Weekly Report 1990; 39:426–433.
fol. Anesthesia and Analgesia 1992; 74: 246–249.
7. Bennett SN, McNeil MM, Bland LA, Arduino MJ, Villarino
33. Cameron E, Johnston G, Crofts S, Morton NS. The minimum
ME, Perrotta DM, Burwen DR, Welbel SF, Pegues DA,
effective dose of lignocaine to prevent injection pain due to
Stroud L, Zeitz PS, Jarvis WR. Postoperative infections traced
propofol in children. Anaesthesia 1992; 47: 604–606.
to contamination of an intravenous anesthetic, propofol. New
34. Weinstein MP, Maderazo E, Tilton R, Maggini G, Quintiliani
England Journal of Medicine 1995; 333: 147–154.
R. Further observations on the antimicrobial effects of local
8. Veber B, Gachot B, Bedos JP, Wol ff M. Severe sepsis after
anesthetic agents. Current Therapeutic Research, Clinical and
intravenous injection of contaminated propofol. AnesthesiologyExperimental 1975; 17: 369–374.
1994; 80: 712–713.
35. Schmidt RM, Rosenkranz HS. Antimicrobial activity of local
9. Hynynen M, Korttila K,Tammisto T. Pain on i.v. injection of
anesthetics: lidocaine and procaine. Journal of Infectious
propofol (ICI 35 868) in emulsion formulation. Acta Diseases 1970; 121: 597–607. Anaesthesiologica Scandinavica 1985; 29: 651–652.
36. Kirk GA, Koontz FP, Chavez AJ. Lidocaine inhibits growth of
10. Skues MA, Prys-Roberts C. The pharmacology of propofol.
Staphylococcus aureus in propofol. Anesthesiology 1992; 77: Journal of Clinical Anesthesia 1989; 1: 387–400.
37. Zaidi S, Healy TE. A comparison of the antibacterial proper-
40. Pearson RD, Steigbigel RT, Davis HT, Chapman SW. Method
ties of six local analgesic agents. Anaesthesia 1977; 32: 69–70.
of reliable determination of minimal lethal antibiotic concen-
38. Crowther J, Hrazdil J, Jol l y DT, Gal braith JC, Greacen M,
trations. Antimicrobial Agents and Chemotherapy 1980; 18:
Grace M. Growth of microorganisms in propofol, thiopental,
and a 1:1 mixture of propofol and thiopental. Anesthesia and
41. Gould JC. The laboratory control of antibiotic therapy. British Analgesia 1996; 82: 475–478. Medical Bulletin1960; 16: 29–34.
39. Reller LB, Stratton CW. Serum dilution test for bactericidal
42. Morello JA, Mizer HE, Wilson ME, Granato PA. Tools and
activity. II. Standardization and correlation with antimicrobial
techniques in microbiology. In: Johnson M, ed. Microbiology in
assays and susceptibility tests. Journal of Infectious DiseasesPatient Care. Dubuque, Iowa: Wm. C. Brown Publ ishers,
1977; 136: 196–204.
Journal of Viral Hepatitis, 2010, 17, 459–468Efficacy and tolerability of peginterferon alfa-2a or alfa-2b plusribavirin in the daily routine treatment of patients with chronichepatitis C in Germany: The PRACTICE StudyT. Witthoeft,1 D. Hueppe,2 C. John,3 J. Goelz,4 R. Heyne,5 B. Moeller,5 G. Teuber,6 S. Wollschlaeger,7 A. Baumgarten,8 K.-G. Simon,9 G. Moog,10 N. Dikopoulos11 and S. Mauss121Pri
Euro Crafts 21: Developing competence for sustainable management in European handicraft Translation of Module S4: Marketing Concept Vienna, December 2009 Source: Westdeutscher Handwerkskammertag (Ed.): CD-ROM: Sustainable Management in crafts enterprises. A manual for the implementation of a qualification and consulting concept for consultants and teachers in the crafts sector.
 Antibacterial activity of lidocaine in Diprivan
Figure 2 Colony counts for gram-positive bacteria (B. subtilis, S. aureus and S. epidermidis) after 24 h of incubation in Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony
counts higher (Mood Median test, P:0.05) than colony counts in Diprivan; *colony counts not significantly lower (Mood Median
Figure 1 Inoculum sizes (colony counts at 0 h) and colony counts
test, P:0.05) than colony counts in Diprivan.
after 24 h of incubation in Diprivan for gram-positive and gram- negative bacteria.
organisms had significantly lower colony counts in
For a more precise measurement of the inoculum
lidocaine concentrations of 0.05% or higher, com-
size and to verify growth and viability of the organ-
pared with counts in propofol alone (fig. 2). All gram-
isms, 0.9% saline 5.25 ml was also inoculated with
negative organisms had significantly lower colony
50 l of the standard suspensions of each bacterium
counts in lidocaine concentrations of 0.2% or higher,
to produce the same final concentration (103 cfu ml91)
compared with counts in propofol alone (fig. 3).
as the test mixtures. Samples of 100 l from this
The recommended dose of lidocaine 10 mg in
growth control were then added to Columbia blood
Diprivan 20 ml (producing a concentration of almost
agar plates and colony counts recorded after incuba-
0.05%) produced significantly lower colony counts
tion for 24 h at 37ЊC. To verify sterility, samples from
compared with colony counts in propofol alone, for
the sources of Diprivan, lidocaine and 0.9% saline
all except two organisms (table 1; figs 1, 2).
were also incubated for 24 h at 37ЊC, and added to
Lidocaine 0.1% (20 mg in Diprivan 20 ml) produced
blood agar plates for colony counts after another 24 h
significantly lower colony counts for all except one
For each organism a bactericidal effect was defined
Figure 4 demonstrates the bacteriostatic and bac-
as the killing (or 99.9% elimination) of the initial
tericidal concentrations of l idocaine for the organ-
inoculum, and a bacteriostatic effect as the preven-
isms tested. Lidocaine 0.2% was bacteriostatic for all
tion of growth, that is no significant change in viable
of gram-positive organisms. Bacteriostatic concen-
count from the initial inoculum.17 Three replicates
trations of lidocaine were 0.6–2% for the gram-nega-
were performed with each organism to complete the
tive organisms. Bactericidal concentrations were
0.2–2% for gram-positive organisms and 0.95–2%
for gram-negative organisms. Bactericidal concentra-
Windows) was used to compare the colony counts of
tion was not determined for B. cepacia, as growth of
each organism in each mixture of l idocaine and
this organism persisted at the highest concentration
Diprivan, with P:0.05 considered significant.
The final concentrations of the organisms after inoculation in Diprivan–lidocaine mixtures were 160–1350 cfu ml91. Figure 1 demonstrates the differ- ent rates of growth of the various organisms in Diprivan, most notable with S. aureus, which was the largest inoculum used yet had the lowest colony counts after 24 h of incubation in Diprivan. Figures 2 and 3 illustrate the colony counts of the gram- positive and gram-negative organisms after 24 h of incubation in the Diprivan–lidocaine mixtures.
With few exceptions, there was a progressive
reduction in colony counts of all organisms with increasing concentration of lidocaine (figs 2, 3).
Comparing colony counts in the lowest concentra-
Figure 3 Colony counts of gram-negative bacteria (B. cepacia,
tion of lidocaine (0.005%) with colony counts in
S. marcescens, E. coli and M. osloensis) after 24 h of incubation in
propofol alone, only one organism had significantly
Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony counts higher (Mood Median test, P:0.05) than colony
lower counts (E. coli) while three organisms had
counts in Diprivan; *colony counts not significantly lower (Mood
significantly higher colony counts. All gram-positive
Median test, P:0.05) than colony counts in Diprivan.
Antibacterial activity of lidocaine in Diprivan
Figure 2 Colony counts for gram-positive bacteria (B. subtilis, S. aureus and S. epidermidis) after 24 h of incubation in Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony
counts higher (Mood Median test, P:0.05) than colony counts in Diprivan; *colony counts not significantly lower (Mood Median
Figure 1 Inoculum sizes (colony counts at 0 h) and colony counts
test, P:0.05) than colony counts in Diprivan.
after 24 h of incubation in Diprivan for gram-positive and gram- negative bacteria.
organisms had significantly lower colony counts in
For a more precise measurement of the inoculum
lidocaine concentrations of 0.05% or higher, com-
size and to verify growth and viability of the organ-
pared with counts in propofol alone (fig. 2). All gram-
isms, 0.9% saline 5.25 ml was also inoculated with
negative organisms had significantly lower colony
50 l of the standard suspensions of each bacterium
counts in lidocaine concentrations of 0.2% or higher,
to produce the same final concentration (103 cfu ml91)
compared with counts in propofol alone (fig. 3).
as the test mixtures. Samples of 100 l from this
The recommended dose of lidocaine 10 mg in
growth control were then added to Columbia blood
Diprivan 20 ml (producing a concentration of almost
agar plates and colony counts recorded after incuba-
0.05%) produced significantly lower colony counts
tion for 24 h at 37ЊC. To verify sterility, samples from
compared with colony counts in propofol alone, for
the sources of Diprivan, lidocaine and 0.9% saline
all except two organisms (table 1; figs 1, 2).
were also incubated for 24 h at 37ЊC, and added to
Lidocaine 0.1% (20 mg in Diprivan 20 ml) produced
blood agar plates for colony counts after another 24 h
significantly lower colony counts for all except one
For each organism a bactericidal effect was defined
Figure 4 demonstrates the bacteriostatic and bac-
as the killing (or 99.9% elimination) of the initial
tericidal concentrations of l idocaine for the organ-
inoculum, and a bacteriostatic effect as the preven-
isms tested. Lidocaine 0.2% was bacteriostatic for all
tion of growth, that is no significant change in viable
of gram-positive organisms. Bacteriostatic concen-
count from the initial inoculum.17 Three replicates
trations of lidocaine were 0.6–2% for the gram-nega-
were performed with each organism to complete the
tive organisms. Bactericidal concentrations were
0.2–2% for gram-positive organisms and 0.95–2%
for gram-negative organisms. Bactericidal concentra-
Windows) was used to compare the colony counts of
tion was not determined for B. cepacia, as growth of
each organism in each mixture of l idocaine and
this organism persisted at the highest concentration
Diprivan, with P:0.05 considered significant.
The final concentrations of the organisms after inoculation in Diprivan–lidocaine mixtures were 160–1350 cfu ml91. Figure 1 demonstrates the differ- ent rates of growth of the various organisms in Diprivan, most notable with S. aureus, which was the largest inoculum used yet had the lowest colony counts after 24 h of incubation in Diprivan. Figures 2 and 3 illustrate the colony counts of the gram- positive and gram-negative organisms after 24 h of incubation in the Diprivan–lidocaine mixtures.
With few exceptions, there was a progressive
reduction in colony counts of all organisms with increasing concentration of lidocaine (figs 2, 3).
Comparing colony counts in the lowest concentra-
Figure 3 Colony counts of gram-negative bacteria (B. cepacia,
tion of lidocaine (0.005%) with colony counts in
S. marcescens, E. coli and M. osloensis) after 24 h of incubation in
propofol alone, only one organism had significantly
Diprivan (D), 2% lidocaine (L) and Diprivan–lidocaine mixtures. †Colony counts higher (Mood Median test, P:0.05) than colony
lower counts (E. coli) while three organisms had
counts in Diprivan; *colony counts not significantly lower (Mood
significantly higher colony counts. All gram-positive
Median test, P:0.05) than colony counts in Diprivan.
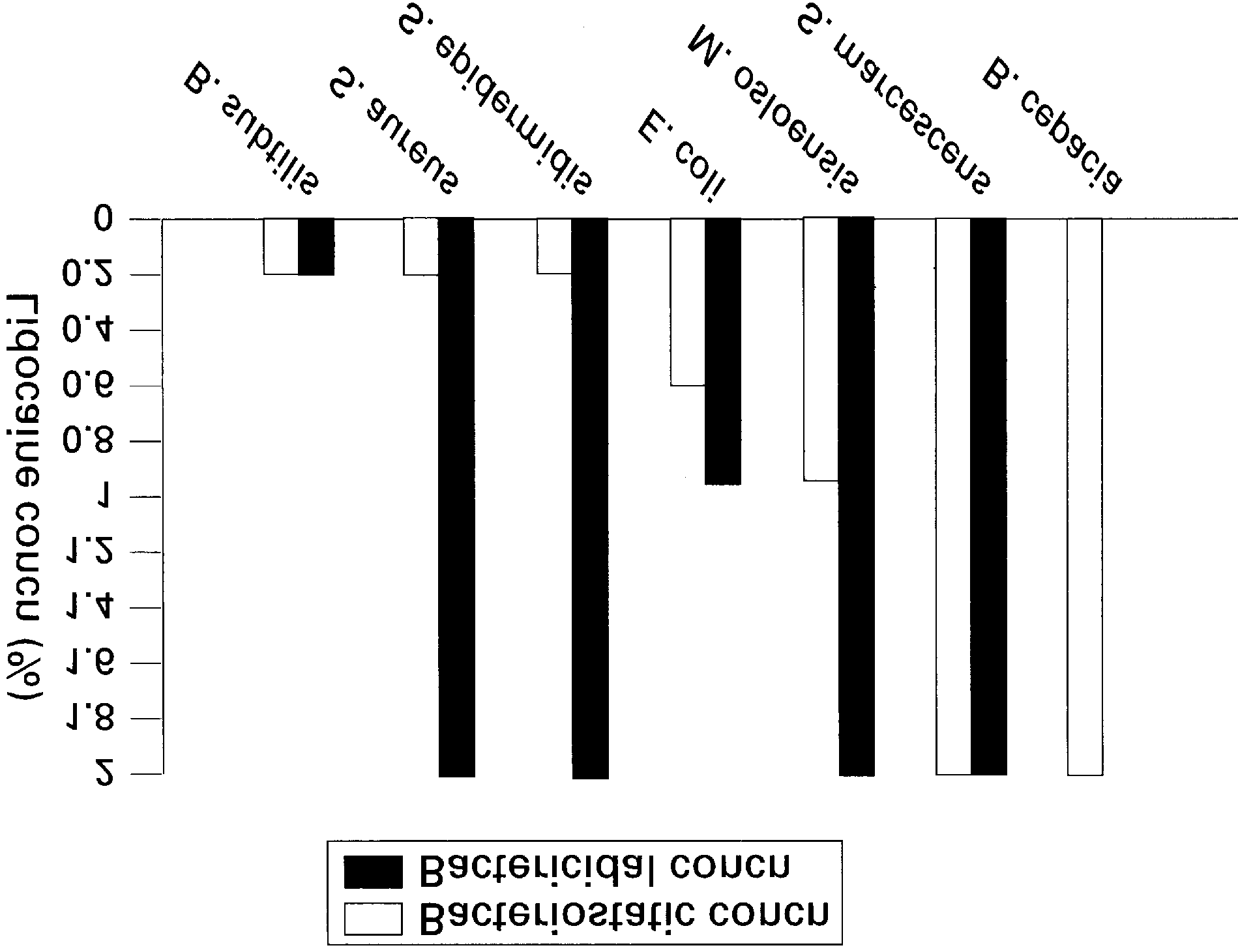 Table 1 Colony counts of gram-positive and gram-negative bacteria after 24 h of incubation in Diprivan and in mixtures of lidocaine (L) and Diprivan. The Mood Median test (P:0.05) was used to compare colony counts. Lidocaine–Diprivan mixtures with colony counts that were not significantly lower (ns) than the corresponding colony counts in Diprivan alone are indicated
Discussion
Table 1 Colony counts of gram-positive and gram-negative bacteria after 24 h of incubation in Diprivan and in mixtures of lidocaine (L) and Diprivan. The Mood Median test (P:0.05) was used to compare colony counts. Lidocaine–Diprivan mixtures with colony counts that were not significantly lower (ns) than the corresponding colony counts in Diprivan alone are indicated
Discussion