Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Jsc201506 2328.2333
RESISTANCE TRAINING IMPROVES DEPRESSIVESYMPTOMS IN INDIVIDUALS AT HIGH RISK FORTYPE 2 DIABETES
ITAMAR LEVINGER,1 STEVE SELIG,1 CRAIG GOODMAN,1 GEORGE JERUMS,2 ANDREW STEWART,3
1Institute for Sport, Exercise and Active Living, School of Sport and Exercise Science, Victoria University, Melbourne, Australia;2Department of Endocrinology, University of Melbourne, Austin Health, Melbourne, Australia; and 3Department of Cardiology,University of Melbourne, Austin Health, Melbourne, Australia
moderate-high intensities appear to alleviate depressed mood
Levinger, I, Selig, S, Goodman, C, Jerums, G, Stewart, A, and
in individuals with clusters of metabolic risk factors.
Hare, DL. Resistance training improves depressive symptoms
KEY WORDS cardiac depression scale, depressed mood,
in individuals at high risk for type 2 diabetes. J Strength Cond
Res 25(8): 2328–2333, 2011—Depression is more prevalent
in obese individuals and those with diabetes, compared to the
general population. This study examined the effect of resistance
training on depressed mood in individuals with high (HiMF, n $
2) and low (LoMF, n # 1) numbers of risk factors for metabolic
The prevalence of obesity and its associated
conditions, such as hypertension, dyslipidemia,and insulin resistance, has proliferated worldwide
syndrome and type 2 diabetes. The primary hypothesis was that
over the past 2 decades (16). Increases in metabolic
resistance training would significantly reduce depressed mood,
risk profile can lead to metabolic syndrome, type II diabetes
as measured by the Cardiac Depression Scale (CDS), in
mellitus (T2DM), and cardiovascular disease (CVD). Obesity
individuals with HiMF. Fifty-five middle-aged volunteers (50.8 6
and metabolic risk factors may not only have physiological
0.9 years, mean 6 SEM) from the general community
and metabolic consequences (17) but may also have
participated in the study. After initial allocation to HiMF or
psychological effects (5). Depression is more prevalent in
LoMF, participants were randomly allocated to 4 groups, HiMF
obese individuals (11) and patients with diabetes (1),compared to in the general population. Depression may
training (HiMFT), HiMF control (HiMFC), LoMF training
also be a major risk factor for obesity and its related
(LoMFT), and LoMF control (LoMFC). Participants underwent
complications (such as T2DM) because it may lead to
resistance training involving major muscle groups on 3 dÁwk21
behavioral changes such as reduced physical activity and
for 10 weeks. Before and after interventions (training or
increased energy intake (24). In addition, in people with
control), participants completed the CDS to assess change in
chronic physical illness, depression is associated with
the level of depressed mood. Following resistance training, the
increased health care use and increased functional disability
CDS score of the HiMFT group was reduced by 214.8 6 4.9
and work absence, compared to in individuals with chronic
points on the CDS, a significant improvement in comparison to
physical illness without depression (23). Finally, individuals
both baseline (p = 0.01) and HiMFC (p = 0.049) values. No
with T2DM who also suffer from depression have an
significant change was observed for LoMFT. In the HiMF group
increased risk for developing diabetic complications(1).
only, the percent change in relative muscle strength was
Questionnaires to quantify depression (such as the Beck
correlated with the D change in CDS; r = 20.46, p = 0.008.
Depression Inventory) have commonly been developed forpsychiatric populations, but they produce skewed score
Resistance exercise training programs that consist 7 exercises
distributions in other populations (2). The cardiac depression
for the major muscle groups at both low-moderate and
scale (CDS) was specifically developed, originally in cardiacpatients, to assess the wide range of depressed moods seen in
Address correspondence to Dr. Itamar Levinger, itamar.levinger@vu.
nonpsychiatric populations, to encompass ‘‘adjustment
disorder with depressed mood’’ and ‘‘minor depression’’
and ‘‘major depression’’ on the Diagnostic and StatisticalManual of Mental Disorders, Fourth Edition classification (9).
Journal of Strength and Conditioning ResearchÓ 2011 National Strength and Conditioning Association
Because many obese and middle-aged individuals have
Journal of Strength and Conditioning Research
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
al of Strength and Conditioning ResearchTM | www.nsca-jscr.org
mildly elevated levels of depressed mood, the CDS was
a person who was not involved in the study, using sealed
thought to be a potentially suitable tool for assessing
envelopes) to 1 of 4 groups: HiMF training (HiMFT, men = 8,
depression in the range found in these individuals who are
women = 5), HiMF nonexercise control (HiMFC, men = 10,
at high risk for developing T2DM and CVD.
women = 5), LoMF training (LoMFT, men = 3, women = 8),
Lifestyle modifications are considered as important
and LoMF nonexercise control (LoMFC, men = 4, women = 9).
interventions for obese individuals and those with metabolic
Randomization was stratified according to sex. Participants
risk factors for T2DM and CVD. Interventions including diet
were on a range of medications including beta-blockers
with behavioral modifications (10), aerobic exercise training
(n = 2), calcium channel blockers (n = 2), angiotensin-
(18), and resistance exercise training (RT) (12) have been
converting enzyme inhibitors (n = 4), diuretics (n = 1), statins
shown to improve quality of life (QoL) in obese populations
(n = 2), metformin (n = 1), and hormone replacement
and those with metabolic risk factors for T2DM and CVD. In
therapy (n = 6). Participants were excluded if they had
addition, Fox (8) has suggested that exercise may be useful in
documented incidence of cardiac disease or they were
the treatment of depression. As such, the aim of this study
involved in regular physical activity in the previous 6 months.
was to determine whether RT reduces the level of depressed
Participants were given written and verbal information on the
mood in middle-aged individuals with risk factors for
nature of the study including the experimental risks and then
developing T2DM and CVD. To our knowledge, no study
signed an informed consent document before the investigation.
has examined the effect of RT on the depressed mood of
The investigation was approved by the Victoria University and
people with a cluster of metabolic risk factors. The primary
Austin Health Human Research Ethics Committees.
hypothesis was that RT would significantly reduce depressed
mood, as measured by the CDS, in individuals with high
Assessment of the Number of Metabolic Risk Factors. The method
numbers of metabolic risk factors (HiMF).
of assessing the number of metabolic risk factors has been
described previously (12). In brief, plasma glucose, tri-glyceride, and high-density lipoprotein levels were analyzed
Experimental Approach to the ProblemParticipants with varying numbers of metabolic risk factors
(SYNCHRON LXÒ System/Lxi725, Beckman Coulter Inc,
were allocated to HiMF and LoMF groups, and then these
Carlsbad, CA, USA) after a 12-hour fast. Blood pressure was
2 groups were each randomly allotted to either the exercise
measured using a mercury sphygmomanometer after partic-
training or nonexercise control group. Levels of depressive
ipants had rested in a seated position for 15 minutes. Systolic
symptoms were analyzed before and after the 10 weeks of
and diastolic blood pressures were recorded to the nearest 2
interventions of either exercise or nonexercise group for both
mm Hg. Waist circumference was measured with a steel tape
and taken as the smallest circumference between the iliaccrest and the lower border of the ribs.
SubjectsA total of 55 (men = 28, women = 27) untrained middle-aged
Cardiac Depression Scale. The CDS contains 26 items on a Likert
individuals (50.8 6 0.9 years, range = 40–69 years; mean 6
scale from 1 to 7, 4 items being reverse scored, and a higher score
SEM) took part in the study. Participants’ anthropometric
indicating a more severe depressed mood (9). The CDS has
measurements were as follows: height = 168.7 6 1.3 cm
excellent receiver operating characteristics with an area under
(range = 152–186 cm), mass = 79.4 6 2.3 kg (range = 40–116
the curve of 0.94 for any depression and 0.96 for major
kg), body mass index = 27.7 6 0.7 kgÁm22 (range = 17–40
depression (20). Although originally developed in cardiac
kgÁm22), and waist circumference = 92.2 6 1.9 cm (range =
patients, it measures core aspects of depression (e.g., depressed
59–121 cm). Participants with 2 or more metabolic risk
mood, anhedonia, and sleep disturbance) measured by
factors, according to the International Diabetes Federation
commonly used depression scales such as the Beck Depression
criteria (IDF) (28), were classified as having HiMF and those
Inventory, Hospital Anxiety Depression Scale, and the Center
with one or no metabolic risk factors were classified as having
for Epidemiologic Studies Depression Scale (22). In addition to
a low number of metabolic risk factors (LoMF). The
measurement of the severity of core depressive symptoms, it
rationale for the HiMF group allocation is that individuals
measures hopelessness-related cognitions associated with de-
with 2 or more risk factors are at a high risk of developing
pression in persons adjusting to a chronic illness such as
metabolic syndrome and T2DM (19). The IDF criteria
diabetes. The CDS has been shown to be a sensitive, reliable,
include the following: waist circumference $94 cm for men
and responsive tool for assessing changes in depression in both
and $80 cm for women, triglycerides $1.7 mmolÁL21, high-
English speaking (3) and non-English speaking populations (25).
density lipoprotein ,1.03 mmolÁL21 for men and ,1.29
Questionnaires were administered by a single investigator.
mmolÁL21 for women, systolic blood pressure $ 130 mm Hg
The internal construct validity of the CDS in this population
or diastolic blood pressure $ 85 mm Hg (or hypertensive
was tested in all 55 participants, at baseline. The test–retest
medications) and fasting blood glucose level $5.6 mmolÁL21.
reliability of the CDS was assessed in the 28 participants
As described previously (12), after the allocation into HiMF
randomly allocated to the nonexercise controls. The external
and LoMF groups, participants were randomly allocated (by
CDS validity was confirmed using the generic Short Form
VOLUME 25 | NUMBER 8 | AUGUST 2011 | 2329
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
36 (SF-36) Health Survey, which is although not designed to
dependent variable was the change (D) from pre-to-post in
measure depression, includes dimensions that reflect
the CDS score, the fixed factor (independent variable) was
depressed mood. The SF-36 contains 36 items comprising
the intervention group (training or control), and the covariate
8 subscales. Four subscales evaluate the physical health
was the baseline (pretraining) score. The relationship
dimension. The remaining 4 subscales constitute the mental
between the change in CDS and the change in muscle
health dimension (15,26). A higher score represents a higher
strength was assessed using Spearman correlation with
level of function and health-related QoL.
The relationship between the CDS and the SF-36 was
Resistance Training Protocol. The training protocol was as
assessed using Spearman correlation between the total CDS
described by Levinger et al. (12). In brief, the RT was
score, separately with both the physical and mental
conducted 3 dÁwk21 for 10 weeks. Training included
dimensions of the SF-36. The baseline data of the 55
7 exercises: chest press, leg press, lateral pull-down, triceps
participants were used for the internal construct validity for
pushdown, knee extension, seated row, and biceps curl.
the CDS in this particular population using standard methods
Training intensity was determined according to the
as used by Birks et al. (3). Cronbach’s a was calculated using
1 repetition maximum (1RM) method. This method has
the 26 individual items of each CDS questionnaire. Test–
been shown to have high reliability for assessing muscle
retest reliability was assessed by comparing the total CDS
strength (13). In the first week, training consisted of 2 sets
score at baseline and the score after 10 weeks for the 28
of 15–20 repetitions at 40–50% of the 1RM for that
participants who were randomly allocated to the control
particular exercise. From weeks 2–10, participants per-
group. These values were compared using Spearman
formed 3 sets of 8–20 repetitions at 50–85% 1RM for each
correlation, intraclass correlation coefficient (ICC), and
exercise. The wide range of repetitions is because of the
stages of progression, 15–20 repetitions in week 2, 12–15
Data are reported as mean 6 SEM, and all statistical
repetitions during weeks 3–6, and 8–12 repetitions during
analyses were conducted at the 95% level of significance.
weeks 7–10. At each session, weights were adjustedaccording to the capacity of the individual, with weightsincreased if the participant was able to achieve the
maximum number of prescribed range of repetitions for
Validity and Reliability of the Cardiac Depression Scale
that week and decreased if the minimum number of range
The internal reliability of the CDS score (n = 28) was high,
of repetitions was not able to be achieved.
with Cronbach’s a = 0.84. The test–retest reliability was
satisfactory with a Spearman correlation = 0.77 (p , 0.01)
Training data were analyzed for the 52 participants who
and ICC = 0.84. Bland–Altman plots revealed a mean and
completed the study. Multivariate analysis of variance was
SEM of difference, between repeat CDS scores, of 2.1 6 3.3.
used to examine the differences in anthropometric and
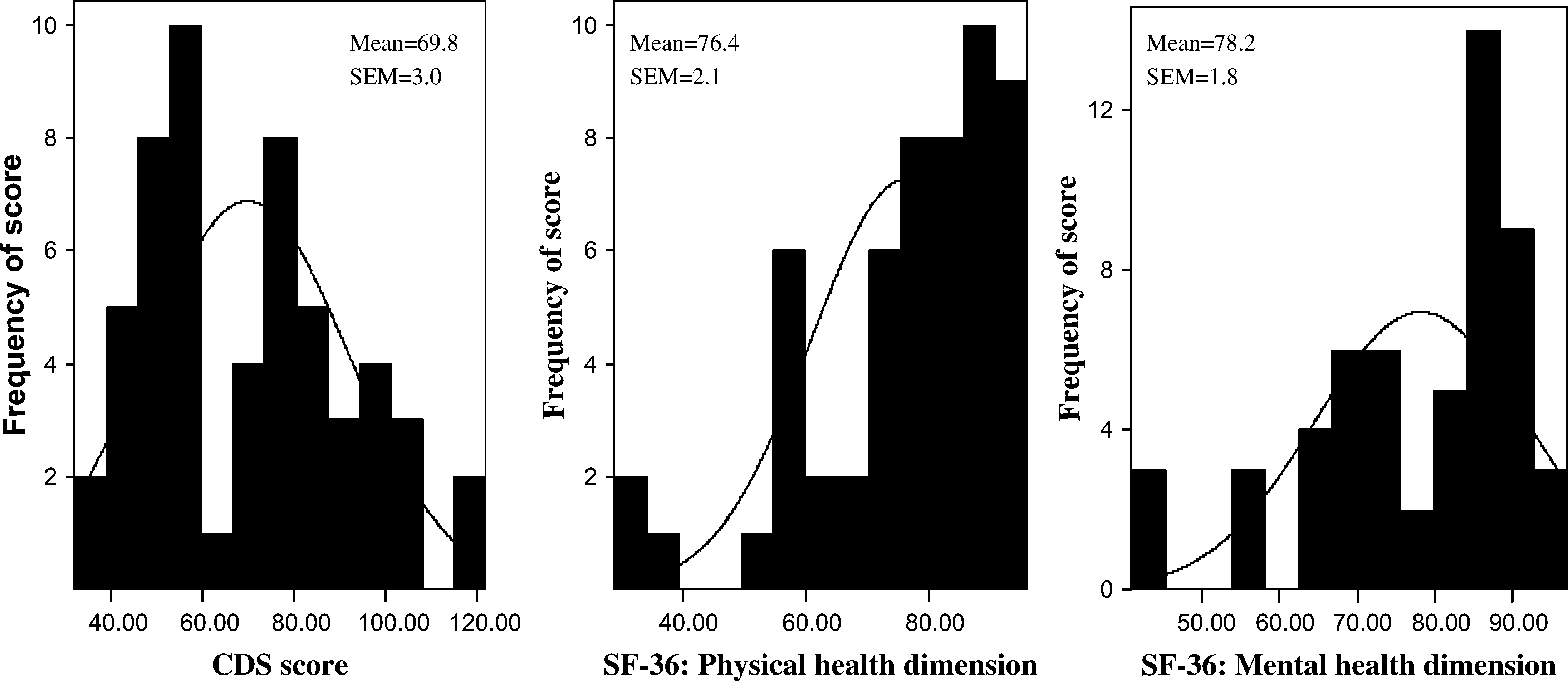
A significant correlation was found between the CDS
metabolic risk factors after the allocation to groups, that is,
scores and the physical (r = 20.78, p , 0.01) and mental
HiMFT vs. HiMFC and LoMFT vs. LoMFC (Table 1). One-
(r = 20.69, p , 0.01) health dimensions of the SF-36. In
way analysis of covariance (ANCOVA) was used to examine
addition, the distribution of scores in the CDS demonstrated
the effect of training on the CDS score as the HiMFT group
greater normality, compared to the physical and mental
had a significant higher CDS score at baseline. The
health dimensions of the SF-36 (Figure 1).
TABLE 1. Baseline comparisons between HiMFT vs. HiMFC and LoMFT vs. LoMFC (n = 52).*†
*HiMFT = high number of metabolic risk factor training group; HiMFC = high number of metabolic risk factor control group; LoMFT =
low number of metabolic risk factor training group; LoMFC = low number of metabolic risk factor control group.
Journal of Strength and Conditioning Research
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
al of Strength and Conditioning ResearchTM | www.nsca-jscr.org
Figure 1. Distribution of scores on the Cardiac Depression Scale (CDS) and physical and mental dimensions of the generic Short Form 36 (SF-36; n = 55).
(1 from the HiMFT group and 1 from the LoMFT group) or
Participants’ anthropometric characteristics are shown in
because of work-related reasons (1 person from the HiMFT
Table 1. At baseline, there were no significant depression
group). The adherence to training was high in both training
score differences between LoMFC and LoMFT (67.9 6 6.2
groups (HiMFT = 88%, and LoMFT = 96%).
vs. 65.5 6 7.2, respectively, p = 0.78). By chance, the HiMFT
The Effect of Training on Cardiac Depression Scale
group had higher depression scores at baseline, compared to
After training, the depression score for HiMFT was reduced
the HiMFC group (82.6 6 5.9 vs. 62.9 6 4.6, p = 0.01). There
(improved) by 14.8 6 4.9 points on the CDS, which was
was also a trend toward higher depression scores in the
a significant improvement compared to both baseline (p =
HiMFT group, compared to in the LoMFT group (p = 0.07).
0.01) and the HiMFC (p = 0.049) values (Figure 2). No
significant change was observed for the LoMFT or LoMFC
Three participants from the training groups (1 from the
group (all p . 0.05) (Figure 2). As reported previously (12),
LoMFT group and 2 from the HiMFT group) did not
muscle strength improved for both HiMFT training groups
complete the study, and their data were excluded from
(by 25%, p , 0.01) and the LoMFT (by 23.7%, p , 0.01),
the training analyses. These 3 individuals did not complete the
compared to their controls. In the HiMF group only, the
study because of medical reasons not related to the study
percent change in absolute muscle strength and relativemuscle strength (total muscle strength/body mass) wascorrelated with the D change in the CDS score (r = 20.045,p = 0.009, and r = 20.46, p = 0.008, respectively).
The main finding of this study is that RT may alleviatedepression in individuals at high risk of developing T2DMand CVD. It also confirms that the CDS is a robust measure ofdepressed mood in this population.
It is widely reported that exercise training (6) can improve
QoL in middle-aged and elderly individuals. It has also beenreported that both aerobic (18) and resistance (12) trainingregimens can improve QoL in individuals at high risk of
Figure 2. The effects of resistance exercise training (RT) on Cardiac
developing T2DM and CVD. Previous studies have shown that
Depression Scale (CDS) score of individuals with a high number of
exercise can improve depression in elderly individuals with
metabolic risk factor training group (HiMF) and a low number of metabolic
major or minor depression (21). There are, however, limited
risk factor training group (LoMF) (mean 6 SEM, n = 52). *p = 0.01compared to baseline, #p = 0.049 compared to control.
data with regard to the effect of RT on symptoms of depressionin middle-aged individuals at a high risk for developing T2DM
VOLUME 25 | NUMBER 8 | AUGUST 2011 | 2331
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
and CVD. We hypothesized that RT can improve depressive
of 55 participants, 28 were men and 27 were women. The
symptoms in this clinical population. We found that short-term
allocation to HiMF or LoMF groups was based on
RT improved depressive mood in the experimental cohort. The
objective IDF criteria, and participants were randomly
implication is that depression in these clinical populations may
allocated and stratified according to sex to ensure near
be alleviated by the application of RT, commencing at moderate
equal numbers of men and women in each study subgroup
intensity and progressing over several weeks to include high-
(i.e., LoMFC and LoMFT and HiMFC and HiMFT, Table 1).
intensity training. Further studies are needed to investigate the
(b) Despite the randomization, HiMFT had higher de-
sustainability of these early benefits. Previously, we have shown
pression scores at baseline, compared to HiMFC. We have
that, in this population, RT can improve muscle strength,
stratified the randomization to sex and used ANCOVA to
functional capacity, and self-perceived QoL (12) without
take the higher baseline depression severity score into
changing metabolic risk factors such as fasting glucose levels,
consideration. However, it is recommended that future
lipid profile, blood pressure, and waist circumference (14). This
studies stratify the randomization to groups according to
suggests that the improvement in the depression score for the
baseline depression scores and not only sex. (c) We did not
HiMFT group occurred independent of changes to metabolic
assess the long-term effect of RT on depressive symptoms
risk profiles. This also shows that the CDS is sensitive to
and as such future studies should include a follow-up measure
exercise training–induced changes in depression. It is important
to identify for how long the benefits of RT on depressive
to note that no change was observed in the depression score for
the LoMFT group, compared to baseline and LoMFC. The
In conclusion, RT programs that consist of 7–8 exercises for
different effects of exercise on HiMFT and LoMFT may be
the major muscle groups at both low-moderate and
related to higher depression scores for HiMFT at baseline. This
moderate-high intensities appear to alleviate the depressed
suggests that it is more difficult to improve depression score in
mood in individuals who have multiple numbers of metabolic
individuals with relatively lower scores of depression or that
risk factors associated with T2DM and CVD. The CDS, as
a longer or more intense training protocol may be needed to
a measure of depressed mood, is a responsive tool for
improve depression scores in individuals with LoMF. It is
assessing exercise intervention in these individuals.
unlikely that the improvement in the depression score in theHiMFT group was simply because of ‘‘regression toward the
mean,’’ as (a) this bias phenomenon is of more relevance in
Resistance exercise training appears to alleviate depressed
nonrandomized studies (27), (b) we have used ANCOVA
mood in individuals who have multiple numbers of metabolic
analysis to take the higher baseline score under consideration in
risk factors associated with T2DM and CVD. Implications
the statistical analysis and (c) the percent changes in absolute
from this study are that RT programs consisting of both low–
muscle strength and relative muscle strength were correlated
moderate and moderate–high intensities can have positive
with the D change in CDS in the HiMF group only. This
effects on the depressive mood of people with clusters of
suggests that the improvement in CDS score was related to the
metabolic risk factors. Furthermore, based on the data that we
increase in muscle strength as a result of the training.
presented here, we recommend the following: low–moderate
Depression, especially mild depression, is more common in
intensity training of 6–8 exercises covering all major muscle
middle-aged individuals and those with metabolic risk factors
groups with 2–3 sets of 15–20 repetitions each and at
or CVD, compared to the general population (7). As such, to
approximately 50–65% of 1RM; and moderate–high intensity
identify and to treat individuals with depression, it is
training consisting of the same exercises with 2–3 sets of 8–15
important to have a valid, reliable, sensitive, and simple tool
repetitions, up to 85% of 1RM. In summary, RT is a simple and
for assessing depression. The results from this study indicate
effective method to improve depressed mood in this
that, although designed for patients with overt cardiac
population and should form an important part of the exercise
disease, the CDS would appear to be a valid and reliable tool
training regimens for people at a high risk of developing
for middle-aged individuals without overt cardiac disease.
The intercorrelations between the CDS and the SF-36 in thisstudy are similar to the intercorrelations reported previously
between the 2 questionnaires in cardiac patients (3). Inaddition, in both this study and that of Birks et al. (3), the
1. Astle, F. Diabetes and depression: A review of the literature. Nutr
CDS demonstrated a more normal distribution of scores
2. Beck, AT, Ward, CH, Mendelson, M, Mock, J, and Erbaugh, J. An
compared to the SF-36, suggesting that the CDS is more
inventory for measuring depression. Arch Gen Psych 4: 561–571,
sensitive to extreme (lower and higher) scores (3). Another
advantage of the CDS is that it is written in relatively simple
3. Birks, Y, Roebuck, A, and Thompson, DR. A validation study of the
language and takes only minutes to complete.
Cardiac Depression Scale (CDS) in a UK population. Br J HealthPsychol 9: 15–24, 2004.
This study has 3 potential limitations: (a) the possibility
4. Bland, JM and Altman, DG. Statistical methods for assessing
for sex bias between HiMF (male:female 20:10) and LoMF
agreement between two methods of clinical measurement. Lancet 1:
(8:17) groups. It is important to note that of the total sample
Journal of Strength and Conditioning Research
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
al of Strength and Conditioning ResearchTM | www.nsca-jscr.org
5. Bray, GA. Medical consequences of obesity. J Clin Endocrinol
17. Must, A, Spadano, J, Coakley, EH, Field, AE, Colditz, G, and Dietz, WH.
The disease burden associated with overweight and obesity. J Am
6. Ellingson, T and Conn, VS. Exercise and quality of life in elderly
individuals. J Gerontol Nutr 26: 17-–25, 2000.
18. Nishijima, H, Satake, K, Igarashi, K, Morita, N, Kanazawa, N, and
7. Fontaine, KR, Cheskin, LJ, and Barofsky, I. Health-related quality of life
Okita, K. Effects of exercise in overweight Japanese with multiple
in obese persons seeking treatment. J Fam Prac 43: 265–270, 1996.
cardiovascular risk factors. Med Sci Sports Exerc 39: 926–933, 2007.
8. Fox, KR. The influence of physical activity on mental well-being.
19. Reaven, GM. The metabolic syndrome: Is this diagnosis necessary?
Public Health Nutr 2: 411–418, 1999.
Am J Clin Nutr 83: 1237–1247, 2006.
9. Hare, DL and Davis, CR. Cardiac depression scale: Validation of
20. Shi, WY, Stewart, AG, and Hare, DL. Both major and minor
a new depression scale for cardiac patients. J Psychosom Res 40: 379–
depression can be accurately assessed using the cardiac depression
10. Kaukua, J, Pekkarinen, T, Sane, T, and Mustajoki, P. Health-related
21. Singh, NA, Clements, KM, and Singh, MA. The efficacy of exercise
quality of life in obese outpatients losing weight with very-low-
as a long-term antidepressant in elderly subjects: A randomized,
energy diet and behaviour modification—A 2-y follow-up study. Int J
controlled trial. J Gerontol 56: M497–M504, 2001.
Obes Relat Metabol Dis 27: 1233–1241, 2003.
22. Snaith, P. What do depression rating scales measure? Br J Psychiatry
11. Kottke, TE, Wu, LA, and Hoffman, RS. Economic and psychological
implications of the obesity. Mayo Clinic Proc 78: 92–94, 2003.
23. Stein, MB, Cox, BJ, Afifi, TO, Belik, SL, and Sareen, J. Does co-
12. Levinger, I, Goodman, C, Hare, DL, Jerums, G, and Selig, S. The
morbid depressive illness magnify the impact of chronic physical
effect of resistance training on functional capacity and quality of life
illness? A population-based perspective. Psychol Med 36: 587–596,
in individuals with high and low numbers of metabolic risk factors.
Diabetes Care 30: 2205–2210, 2007.
24. Stunkard, AJ, Faith, MS, and Allison, KC. Depression and obesity.
13. Levinger, I, Goodman, C, Hare, DL, Jerums, G, Toia, D, and Selig, S.
Biol Psychiatry 54: 330–337, 2003.
The reliability of the 1RM strength test for untrained middle-aged
25. Wang, W, Thompson, DR, Chair, SY, and Hare, DL. A
individuals. J Sci Med Sport 12: 310–316, 2009.
psychometric evaluation of a Chinese version of the Cardiac
14. Levinger, I, Goodman, C, Matthews, V, Hare, DL, Jerums, G,
Depression Scale. J Psychosom Res 65: 123–129, 2008.
Garnham, A, and Selig, S. BDNF, risk factors for metabolic
26. Ware, JE. SF-36 Physical and Mental Health Summary Scales: A Manual
syndrome and resistance training in middle-aged individuals Med Sci
for Users of Version 1. Boston, MA: The Health Institute, New England
15. McHorney, CA, Ware, JE, and Raczek, AE. The MOS 36-item short-
27. Weeks, DL. The regression effect as a neglected source of bias in
form health survey (SF-36): II. Psychometric and clinical tests of
nonrandomized intervention trials and systematic reviews of
validity in measuring physical and mental health constructs. Med
observational studies. Eval Health Prof 30: 254–265, 2007.
28. Zimmet, PZ, Alberti, KG, and Shaw, JE. Mainstreaming the
16. Miranda, PJ, DeFronzo, RA, Califf, RM, and Guyton, JR. Metabolic
metabolic syndrome: A definitive definition. This new definition
syndrome: Definition, pathophysiology, and mechanisms. Am Heart
should assist both researchers and clinicians. Med J Aus 183: 175–
VOLUME 25 | NUMBER 8 | AUGUST 2011 | 2333
Copyright National Strength and Conditioning Association Unauthorized reproduction of this article is prohibited.
Creative workout competition: Week 7-14 March This is a monthly opportunity to pit your wits against other communications students across Europe on a real brief. But be quick as you only have one week to work on the brief and upload your ideas to ourgroup. The UK based advertising agency “ Crayon ” will then judge what they deem to be the best and most exciting solution to the proble
This article was downloaded by:On: 4 November 2010Access details: Access Details: Free AccessPublisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UKPublication details, including instructions for authors and subscription information:Curcumin, the Golden Spice From Indian Saffron, Is a
 al of Strength and Conditioning ResearchTM | www.nsca-jscr.org
Figure 1. Distribution of scores on the Cardiac Depression Scale (CDS) and physical and mental dimensions of the generic Short Form 36 (SF-36; n = 55).
al of Strength and Conditioning ResearchTM | www.nsca-jscr.org
Figure 1. Distribution of scores on the Cardiac Depression Scale (CDS) and physical and mental dimensions of the generic Short Form 36 (SF-36; n = 55).