Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Microsoft word - 131109-bmj_author_web_version.doc
Treatment of anxiety from musical obsessions with
a cognitive behaviour therapy tool. Liikkanen, Lassi A. & Raaska, Kari BMJ Case Studies.
Published Early online 8th of November 2013 DOI:10.1136/bcr-2013-201064
This is author reprint version of peer-reviewed paper
TITLE OF CASE
Treatment of anxiety from musical obsessions with a cognitive behaviour therapy tool SUMMARY Musical obsessions and hallucinations are disturbing experiences of repeating internal music. Antipsychotic medication can sometimes reduce these symptoms but can also trigger or augment them. We report about a female patient suffering from schizophrenia with drug-resistant obsessive musical hallucinations. The patient volunteered in a nine months pilot study to follow the development of the condition using an involuntary music and mood inventory. The patient perceived benefits from the intervention, including reduced anxiety, increased feeling of being in control and understanding the condition better. Findings from this case study suggest that cognitive therapy can be a useful complementary method of care for persons suffering from musical obsessions. The presented tool requires further investigations among those suffering from this rare condition.
BACKGROUND
The involuntary perception of music is a symptom that relates to a spectrum of mental disorders1. Musical hallucinations are among most commonly encountered hallucinations in clinical institutions. Although not foreign to schizophrenia, involuntary music perceptions also
occur among people without apparent mental disorders and no deterioration of subjective wellbeing. Recent studies of involuntary musical imagery (INMI) in psychology2-4 reveal a
high frequency of involuntary music episodes among the general population. In these cases, normal, healthy individuals repeatedly experience seemingly uncontrollable repetition of
musical memories, with a clear insight to the self-generated nature of the experience. These ‘earworms’ are a harmless everyday phenomenon and not a cause for concern. Musical hallucinations are the most common symptom in clinical conditions of involuntary music1, 5. Females, people over sixty years old, and socially isolated individuals may have an
elevated risk of developing these symptoms5. Musical hallucinations can be associated with peripheral hearing loss5, but also with mental disorders6.One study reported prevalence of
under 0.2% in general hospital population7, while another study reported a lifetime prevalence of 26.8% in psychiatric outpatients8. In the latter, musical hallucinations were
associated with obsessive-compulsive disorder (OCD) and were most frequent (> 50%) in OCD patients with comorbid psychiatric conditions (e.g. schizophrenia). Obsessive symptoms are more common in schizophrenia than in the general population9. Such obsessions of the
schizophrenia patients can be either similar to those of OCD patients or be psychotic, obsessive hallucinations.
There is no standard pharmacological or psychotherapeutic treatment for the obsessive
symptoms in schizophrenia patients. Because they can be both hallucinatory and obsessive9, they would be expected to respond to either antipsychotics alone or in combination with
antidepressants. Musical obsessions in patients without schizophrenia have been treated successfully with clomipramine5, 10. However, de-novo OCD symptoms in schizophrenia patients have been triggered by atypical antipsychotics, especially clozapine11, and also by
lamotrigine12. In the latter case, musical hallucinations become controlled by switching lamotrigine to valproate. This solution is not always available. Switching from clozapine is
not an option for patients resistant to other antipsychotics, who have clozapine-induced obsessive symptoms. As an alternative, the evidence supporting therapeutic care is
unfortunately also scarce13. This paper reports a case study of clozapine-triggered musical obsessions in a schizophrenia patient. The anxiety caused by these obsessions was
considerably reduced with a novel cognitive behavioural therapy (CBT) tool introduced here while continuing the clozapine treatment.
CASE PRESENTATION
The person, Mrs. B, is a 36-yer old Caucasian female diagnosed with paranoid schizophrenia. She has a college degree and no family history of mental or neurological disorders, but
suffers from slight bilateral hypacusis and lopsided tinnitus. Before the onset of her condition, she was pursuing a doctorate degree and working as a researcher. In November 2004, at the age of 27, she was treated first time for a psychotic episode with delusions and
various psychosomatic symptoms, apparently triggered by a trauma. She was admitted to a hospital and was first treated with risperidone with increasing dosage up to 4 mg without
any improvement of her condition and with the introduction of extrapyramidal adverse effects. Switching to olanzapine at 10 mg resolved her delusional fears over night without
apparent side effects. She was also treated with 20 mg fluoxetine to control depression and anxiety. She was released after five weeks in December 2004.
Four months after her release from the unit, B discontinued olanzapine as it interfered with
her everyday life and the desire to continue working. Since February 2004, she was taking fluoxetine antidepressant, which was later switched to fluvoxamine 50 mg due to side effects. After two months and doubling of the dose of fluvoxamine it was deemed effective
for controlling neither anxiety nor depression and was replaced by escitalopram 10 mg. However, B also discontinued this medication after 6 weeks due to perceived lack of efficacy.
In December 2005, B again experienced somatic symptoms and increased level of anxiety.
She was again prescribed olanzapine from 5 mg up to 10 mg, but this time without efficacy for her symptoms. In the following month, she continued to experience dizziness,
tachycardia, and other somatic symptoms. After the onset of paranoid thoughts and insomnia, she was admitted to the psychiatric ward in January 2006 and remained in care until mid April 2006. She was examined for an early psychosis, with a consideration for a
schizo-affective disorder, although the eventual diagnosis was paranoid schizophrenia. After several unsuccessful trials with different antipsychotics (risperidone, olanzapine, aripiprazole,
quetiapine, perphenazine), her psychotic and affective symptoms were successfully controlled in early April 2006 with clozapine only 75 mg per day. By this time B had been
examined a full head MRI scan following the first psychosis, and an EEG examination after the second, but these examinations did not suggest any functional or structural abnormality.
During the time of the second episode of hospital care, involving experiments with different drug treatments, she noticed that he was often singing aloud and felt a strong craving for
music. She was the most disturbed by the repetition of musical fragments inside her head. Mrs. B was accustomed to INMI experiences, but perceived her apparently drug-induced
condition as obsessive and intrusive. Although she does not recall being much bothered with music after being going out of hospital in 2006, she believes the disruptive musical thoughts
surfaced again in spring 2007. She recalls an episode from May in which music experiences were obsessive. She joined a choir in late 2007, which she thought improved her moods but
further exaggerated musical symptoms. The symptoms neither varied in response to small (25mg) changes in clozapine dosage nor along her hormonal cycle. She believed that increased work-related stress did exaggerate the symptoms.
TREATMENT
Having suffered from musical obsessions for over three years, B contacted the author A in
2009. She agreed to participate in a trial with a novel CBT inspired instrument Music and Moods Inventory (MMI) and document her musical symptoms daily14. This longitudinal study
concentrated on her daily moods and involuntary music experiences. An adaptation of an instrument illustrated in Figure 1 was developed for the general population2 was used, now
focused on the disruptiveness and repetitiveness of music in everyday life. Emotional state was reported with a modified 10-item The Positive And Negative Affect Schedule (PANAS)
scale15. B used a printed survey to make numerical estimates of her feelings and experiences with the help of scoring guidelines provided by A. Clozapine and regular outpatient visits continued during the trial as usual and the communications between A and B happened
solely via email approximately once a month.
Figure 1. A sample of MMI form as it was printed and
OUTCOME AND FOLLOW-UP
Patient B kept the diary for 278 consecutive days, approximately nine months. During this time, the frequency and disturbance of her symptoms decreased, as measured by the
instrument (see Fig. 2). The positive outcomes of the trial were confirmed by B’s outpatient care psychiatrist. The content of her musical obsessions reflected her choir repertoire, for
instance including numerous Abba songs. She discontinued the reporting at a time when the music repetition and disturbance scores had reached a floor level and she found the documenting meaningless. The analysis of MMI scores found that B largely equated the
disturbance of involuntary music by its frequency of repetition over the day. Across the 278 data points, the two scores were linearly correlated (r=.818). There was no correlation
between negative and positive mood scores or between them and music repetition or disturbance.
Figure 2. Line chart showing major trends in the daily states
reported by Mrs. B. Xaxis shows the calendar month
since the reporting started in October 2009.
Values on Y-axis represent monthly averages and
are not comparable across the plotted variables.
In a three year follow-up after the therapy, she continues on clozapine, but has remained less anxious and less disturbed by the musical symptoms.
DISCUSSION
This paper has described a woman with drug-resistant “musical obsessions” comorbid with schizophrenia. Her musical symptoms increased after otherwise successful clozapine
treatment began. However, because her psychotic and affective symptoms responded well to clozapine but were resistant to several other antipsychotics and antidepressants benefits of
clozapine were considered to outweight the increase in musical obsessions. Therefore, instead of discontinuing clozapine a CBT tool was tested here for the treatment of musical
The improvement of the patient seemed to occur through increased introspective insights to her condition. Having means to quantify the extent of her symptoms reduced the worries
that the symptoms were uncontrollable and not understandable, and seemed to empower the patient. This is in line with an earlier case study of applying therapy to musical
obsessions13. The type of CBT treatment tried here placed considerable requirements for the compliance of the patient. Mrs. B was very motivated, persistent, and co-operative in the face of minimal
contact hours with the therapist. This was deemed very important for the success of the trial. Experiences with this patient suggest that cognitive therapy can be an effective
treatment for certain conditions of involuntary. Based on the current insights, it is valuable to consider therapy treatment in occasions where involuntary music experience is a comorbid symptom.
What does the case of Mrs. B reveal about the nature of involuntary music? It is consistent
with the idea that involuntary music involves a continuum of phenomena from casual involuntary musical imagery to more troublesome and debilitating musical obsessions and
hallucinations16. This means that only a slight, gradual change in the pervasiveness of the involuntary music might be required to turn the normally manageable condition into a
debilitating one. Currently, we do not know enough of the neural underpinnings of regular INMI to pinpoint
any cortical area, connection, or neurotransmitter system as a cause of this shift. This is also a remaining challenge for diagnosis, as no clear-cut criteria exist for distinguishing different
types of music conditions from each other. Especially the discussion about the existence of musical pseudohallucinations16, 17 should take into consideration the recent findings of
involuntary music outside the clinical sphere 2, 18. Taking new knowledge from psychology to bear on psychiatric can be useful in the long term.
For future research, it would be beneficial to use MMI to other cases of musical obsession to assess its validity. Given the rare morbidity of musical obsessions, discovering and helping
these patients will require international collaboration. Although some norms about the frequency and characteristics INMI exists2 additional research to standardizing these
measures is needed. If objective measures to quantify the characteristics of involuntary music were found, then we could considerably improve the diagnosis and care of this
condition. Disclosure of Interest The study and reporting by Author A were supported by a research grant (#129477) from the Academy of Finland. Authors state no other conflicts of interests.
LEARNING POINTS Involuntary music is a wide ranging phenomenon with few extreme cases
Musical obsessions are debilitating but a rare and poorly understood condition
Musical obsessions can be drug-resistant or even drug-induced
This case shows promise for treating drug-resistant music with cognitive therapy
REFERENCES 1.
Berrios GE. Musical hallucinations. A historical and clinical study. The British Journal
of Psychiatry. 1990 February 1, 1990;156(2):188-94.
Liikkanen LA. Musical Activities Predispose to Involuntary Musical Imagery.
Williamson VJ, Jilka SR, Fry J, Finkel S, Müllensiefen D, Stewart L. How do
"earworms" start? Classifying the everyday circumstances of Involuntary Musical Imagery. Psychology of Music. 2012 September 27, 2011;40(3):259-84.
Beaman CP, Williams TI. Earworms (‘stuck song syndrome’): Towards a natural
history of intrusive thoughts British Journal of Psychology. 2010;101(4):637–53.
Cope TE, Baguley DM. Is musical hallucination an otological phenomenon? a review of the literature. Clinical Otolaryngology. 2009;34(5):423-30.
Baba A, Hamada H, Kocha H. Musical hallucinations in schizophrenia - 2. Relations
with verbal hallucinations. Psychopathology. 2003 Mar-Apr;36(2):104-10.
Fukunishi I, Horikawa N, Onai H. Prevalence Rate of Musical Hallucinations in a
General Hospital Setting. Psychosomatics. 1998;39(2):175.
Hermesh H, Konas S, Shiloh R, Dar R, Marom S, Weizman A, et al. Musical
hallucinations: Prevalence in psychotic and nonpsychotic outpatients. Journal Of Clinical Psychiatry. 2004 Feb;65(2):191-7.
Poyurovsky M, Weizman A, Weizman R. Obsessive-compulsive disorder in schizophrenia: clinical characteristics and treatment. CNS Drugs. 2004;18(14):989-
Matsui T, Matsunaga H, Ohya K, Iwasaki Y, Koshimune K, Miyata A, et al. Clinical features in two cases with musical obsessions who successfully responded to
clomipramine. Psychiatry And Clinical Neurosciences. 2003 Feb;57(1):47-51.
Schirmbeck F, Zink M. Clozapine-induced obsessive-compulsive symptoms in
schizophrenia: A critical review. Current Neuropharmacology. 2012;10(1):88.
Bleich-Cohen M, Hendler T, Pashinian A, Faragian S, Poyurovsky M. Obsessive Musical
Hallucinations in a Schizophrenia Patient: Psychopathological and fMRI Characteristics. CNS spectrums. 2011;16(07):153-6.
Gomibuchi T, Gomibuchi K, Akiyama T, Tsuda H, Hayakawa T. Obsession of hearing music: From the viewpoint of Morita theory. Psychiatry And Clinical Neurosciences. 2000 Apr;54(2):203-6.
Kahneman D, Krueger AB, Schkade DA, Schwarz N, Stone AA. A survey method for characterizing daily life experience: The day reconstruction method. Science.
Watson D, Clark LA. The PANAS-X: Manual for the positive and negative affect
schedule-expanded form. Journal [serial on the Internet]. 1999 Date; 8: Available from: http://ir.uiowa.edu/psychology/psychology_pubs/11.
van der Zwaard R, Polak MA. Pseudohallucinations: A pseudoconcept? A review of the validity of the concept, related to associate symptomatology. Comprehensive Psychiatry. 2001;42(1):42-50.
Praharaj SK, Goyal N, Sarkar S, Bagati D, Sinha P, Sinha VK. Musical obsession or pseudohallucination: Electrophysiological standpoint. Psychiatry And Clinical
Liikkanen LA. Involuntary Music Among Normal Population and Clinical Cases.
Advances in Clinical Neuroscience and Rehabilitation. [Review]. 2012;12(4):12-3.
We have managed to survive the wet weather and are hoping for a drier weekend! The children have made an excellent start to the school year, with all our pupils and staff working really hard and playing their part fully to help us to continue moving forward as a school. Start of the School Day We would just like to remind parents of the arrangements at t
ABORDAJE FARMACOLÓGICO DEL PACIENTE AGITADO Comisión de Farmacia y Terapéutica X.A.P de Santiago 1. AGITACIÓN ORGÁNICA Deben extremarse las precauciones por los riesgos que supone administrar a un paciente médicamente grave un depresor del SNC. Mientras se resuelve la causa de la agitación, se puede recurrir a la sedación - De primera elección: Haloperidol , 2.5-5 mg IM, re
 Treatment of anxiety from musical obsessions with
a cognitive behaviour therapy tool.
Treatment of anxiety from musical obsessions with
a cognitive behaviour therapy tool. 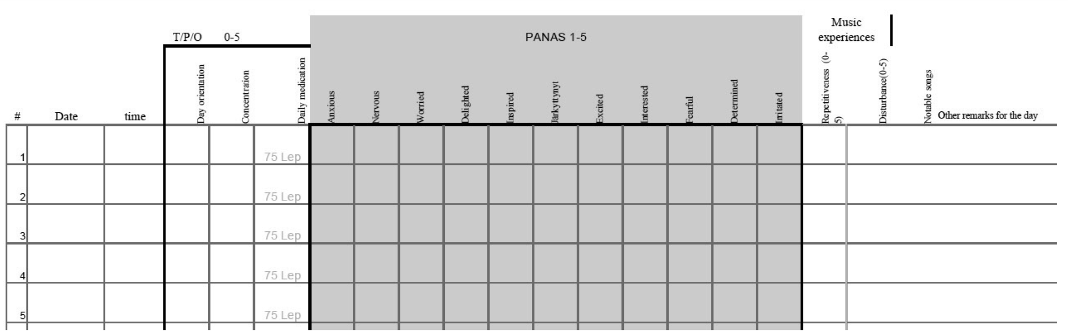
 Figure 1. A sample of MMI form as it was printed and
Figure 1. A sample of MMI form as it was printed and