Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Varsal.com.cn
C l i n i c a l C a r e / E d u c a t i o n / N u t r i t i o n O R I G I N A L Oral Treatment With ␣-Lipoic Acid Improves Symptomatic Diabetic Polyneuropathy The SYDNEY 2 trial AN ZIEGLER, MD, FRCPE ULLRICH MUNZEL, PHD LEXANDER AMETOV, MD NIKOLAI YAKHNO, MD Atleastoneoffourdiabeticpatients LEXEY BARINOV, MD ITAMAR RAZ, MD ETER J. DYCK, MD MARIA NOVOSADOVA, MD RINA GURIEVA, MD JOACHIM MAUS, MD HILLIP A. LOW, MD RUSTEM SAMIGULLIN, MD
pain and is responsible for both substan-tial morbidity and increased mortality (1–4). Neuropathic pain affects 16% of
OBJECTIVE — The aim of this trial was to evaluate the effects of ␣-lipoic acid (ALA) on
diabetic patients (5) and exerts a substan-
positive sensory symptoms and neuropathic deficits in diabetic patients with distal symmetric
tial impact on the quality of life, particu-
larly by causing interference of sleep and
RESEARCH DESIGN AND METHODS — In this multicenter, randomized, double-
enjoyment of life (6). Pain is a subjective
blind, placebo-controlled trial, 181 diabetic patients in Russia and Israel received once-daily oral
doses of 600 mg (n ϭ 45) (ALA600), 1,200 mg (n ϭ 47) (ALA1200), and 1,800 mg (ALA1800)
of ALA (n ϭ 46) or placebo (n ϭ 43) for 5 weeks after a 1-week placebo run-in period. The
primary outcome measure was the change from baseline of the Total Symptom Score (TSS),
including stabbing pain, burning pain, paresthesia, and asleep numbness of the feet. Secondary
end points included individual symptoms of TSS, Neuropathy Symptoms and Change (NSC)
score, Neuropathy Impairment Score (NIS), and patients’ global assessment of efficacy.
nisms of DSP (8), several therapeutic ap-proaches have been developed including
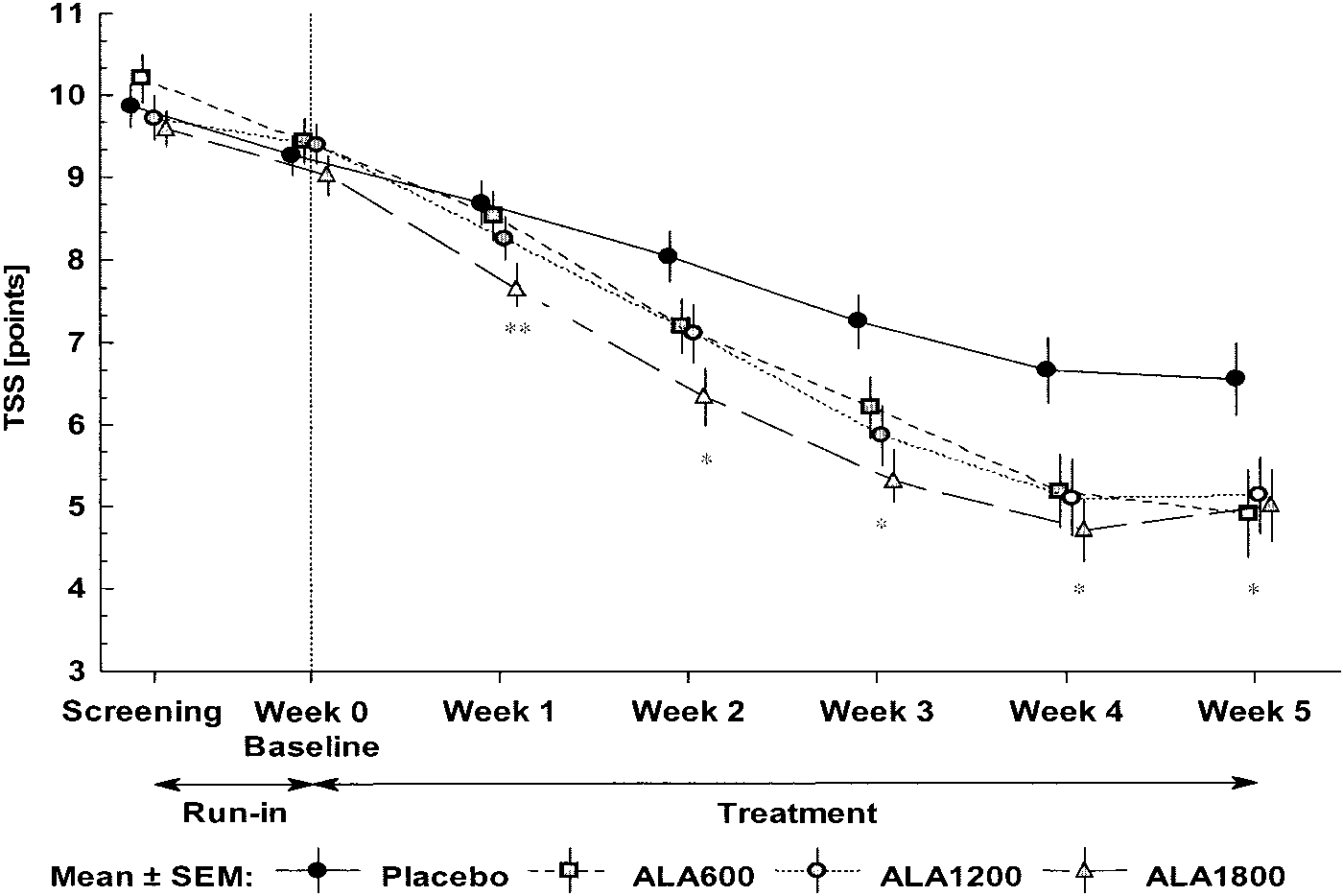
RESULTS — Mean TSS did not differ significantly at baseline among the treatment groups and on average decreased by 4.9 points (51%) in ALA600, 4.5 (48%) in ALA1200, and 4.7 (52%) in
antioxidants such as ␣-lipoic acid (ALA)
ALA1800 compared with 2.9 points (32%) in the placebo group (all P Ͻ 0.05 vs. placebo). The
corresponding response rates (Ն50% reduction in TSS) were 62, 50, 56, and 26%, respectively.
Significant improvements favoring all three ALA groups were also noted for stabbing and burn-
signed to favorably influence the underly-
ing pain, the NSC score, and the patients’ global assessment of efficacy. The NIS was numerically
reduced. Safety analysis showed a dose-dependent increase in nausea, vomiting, and vertigo.
solely to relieve pain. It is likely that in theforeseeable future, near normoglycemia
CONCLUSIONS — Oral treatment with ALA for 5 weeks improved neuropathic symptoms
will not be achievable in the majority of
and deficits in patients with DSP. An oral dose of 600 mg once daily appears to provide the
pounds could offer the advantage of being
Diabetes Care 29:2365–2370, 2006
effective despite persistent hyperglycemia.
1,258 diabetic patients with symptomaticDSP from four randomized clinical trials(14) including the first Symptomatic Dia-
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1German Diabetes Clinic, German Diabetes Center, Leibniz Institute at the Heinrich Heine Uni-
versity, Du¨sseldorf, Germany; the 2Russian Medical Academy for Advanced Studies, Moscow, Russia; the3Neurology Clinic, Moscow Medical Academy, Moscow, Russia; the 4Department of Neurology, Mayo
600 mg i.v. as a daily infusion for 3 weeks
Clinic, Rochester, Minnesota; the 5Federal Center for Diabetic Foot, Moscow, Russia; 6MEDA Pharma, Bad
Homburg, Germany; and 7Hadassah University, Jerusalem, Israel.
to a clinically meaningful degree. This ef-
Address correspondence and reprint requests to Prof. Dan Ziegler, MD, FRCPE, Deutsche Diabetes-
Klinik, Deutsches Diabetes-Zentrum, Leibniz-Institut an der Heinrich-Heine-Universita¨t, Auf’m Hen-nekamp 65, 40225 Du¨sseldorf, Germany. E-mail: [email protected].
of neuropathic deficits, assuming a poten-
Received for publication 12 June 2006 and accepted in revised form 26 July 2006.
tial of the drug to favorably influence the
Abbreviations: ALA, ␣-lipoic acid; DSP, distal symmetric polyneuropathy; NIS, Neuropathy Impairment
Score; NSC, Neuropathy Symptoms and Change; TSS, Total Symptom Score.
from a small oral pilot study (ORPIL) us-
D. Z., A.A., A.B., P.J.D., I.G., P.A.L., N.Y., I.R., and M.N. received honoraria for speaking activities and
A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
DOI: 10.2337/dc06-1216. Clinical trial reg. no. NCT00328601, clinicaltrials.gov.
2006 by the American Diabetes Association.
have not yet been established. Therefore,
The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
␣-Lipoic acid in diabetic polyneuropathy
response trial using ALA (600, 1,200, and
ripheral vascular disease severe enough to
ble), and stage 3 (disabling neuropathy).
after a 1-week placebo run-in period.
ulcers or limb ischemia; significant he-patic or renal disease, antioxidant ther-
RESEARCH DESIGN AND METHODS — The SYDNEY 2 trial
blood pressure and heart rate after 3 min
␥-linolenic acid– containing substances of sitting, body weight, and standard lab-
multicenter trial using three oral doses of
Primary outcome measure. The pri-
the comparison of the changes in TSS from
baseline to the end of treatment among the
stabbing pain, burning pain, paresthesia,
effects but no treatment-center interactions.
start of study treatment, and after 1, 2, 3,
4, and 5 weeks of treatment. All other pa-
meaningful response to treatment. For all
screening and at the end of the study.
efficacy variables, the analyses of the in-
Secondary outcome measures. The
tention-to-treat population were primary.
three centers in Russia. All patients were
plied with the baseline as covariate. In the
for 1 week (single-blind run-in phase).
sessment as previously described (15).
5), the last value carried forward principle
action, each time point was analyzed anal-
(0 ϭ normal to 4 ϭ paralyzed), reflexes
(0 ϭ normal to 2 ϭ absent with reinforce-
because, in previous studies, no plateau in
c e n t e r - a d j u s t e d C o c h r a n - M a n t e l -
dality) of the index finger and great toe
and is scored for both sides of the body.
a slower onset of efficacy was assumed for
confirmatory analysis. The level of signif-
Inclusion criteria at the screening visit
icance (two sided) was set at ␣ ϭ 0.05.
1–19; sensation, questions 20 –29; and
tes (type 1 or 2) defined by American Di-
RESULTS — Of the 227 patients
and latency of the sural nerve) were per-
patic or renal disease. Thus, 187 patients
score for lower limbs (NIS[LL]) Ն2 points,
prick test absent or decreased. At the ran-
domization visit after the 1-week run-in,
subjects had to comply with all of the fol-
lowing criteria: TSS Ն5 points; TSS range
efficacy was rated by the patient as very
trial. Most patients (12) discontinued be-
good/good, satisfactory, or insufficient.
cause of adverse events: 1 in the placebo
al. (17,18): stage 0 (no neuropathy), stage
last 3 months, sufficient compliance 85–
plete the trial because of lack of efficacy;
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
Ziegler and Associates Table 1—Clinical characteristics in the intention-to-treat population
Treatment with oral antidiabetic agents (%)
Data means Ϯ SD unless otherwise indicated. *Smoker within the last 2 years.
compared with the placebo arm (all P Ͻ
the changes in mean TSS at any of the time
0.05) (Table 2). No significant differences
tients are shown in Table 1. As a sign of
pared with 26% after placebo (P Ͻ 0.05).
ment with oral antidiabetic agents (P ϭ
0.018) and BMI (P ϭ 0.036, Table 1).
blind period of the trial are illustrated in
and NIS[LL] at screening and their changes
Table 3. There were no significant differ-
line TSS and its individual subscores.
groups versus placebo at weeks 2–5 (P Ͻ
After 5 weeks of treatment, a significant
placebo at week 1 (P Ͻ 0.05).
scores for stabbing/lancinating and burn-
Table 2—Baseline levels and changes from baseline (negative values correspond to improvement) in the TSS and its individual subscores after 5 weeks of treatment (last value carried forward)
Data are means Ϯ SD. *P Ͻ 0.05 vs. placebo.
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
␣-Lipoic acid in diabetic polyneuropathy
the ALA1800 group (P Ͻ 0.05 for all ALAdoses vs. placebo).
verse events were 9 (21%) in the placebogroup, 12 (27%) in the ALA600 group(P ϭ 0.53 vs. placebo), 20 (43%) in theALA1200 group (P ϭ 0.03 vs. placebo),and 25 (54%) in the ALA1800 group (P ϭ0.001 vs. placebo). The rates of treat-ment-emergent adverse events in WorldHealth Organization preferred terms(Ͼ10% in any group) increased with es-calating doses and were nausea 0, 6(13%), 10 (21%), and 22 (48%) (P Ͻ 0.05for all ALA groups vs. placebo); vomiting0, 1 (2%), 2 (4%), and 12 (26%) (P Ͻ0.05 for ALA1800 vs. placebo); vertigo 0,2 (4%), 2 (4%), and 5 (11%), respectively(P ϭ 0.056 for ALA1800 vs. placebo). CONCLUSIONS — The results of the
Figure 1—Mean TSS levels on a weekly basis during the placebo run-in and the randomizeddouble-blind period of the trial. *P Ͻ 0.05 for ALA600, ALA 1200, and ALA1800 vs. placebo;**P Ͻ 0.05 for ALA1800 vs. placebo.
proved the positive sensory symptomsscored by the TSS in diabetic patients
cebo group (all P Ͻ 0.05, except for NSC
with DSP. This overall effect was not dose
number in ALA1800: P ϭ 0.08). For the
with placebo (P ϭ 0.09) were noted. No
dependent, as there were no differences in
ment was noted in ALA1200 (P Ͻ 0.05)
ALA1800 versus placebo (P ϭ 0.055). Re-
garding the changes in NIS[LL], a trend for
good/good, satisfactory, and insufficient
ALA600 group (P ϭ 0.07 vs. placebo).
paresthesia and numbness was observed.
the placebo group, 62, 27, and 11% for the
and placebo (P Ͻ 0.05) and a borderline
Table 3—Screening levels and changes from screening in NSC scores, NIS, and NIS͓LL͔ after 5 weeks of treatment (last value carried forward)
Data are means Ϯ SD. Negative values correspond to improvement. *P Ͻ 0.05, †P ϭ 0.08, ‡P ϭ 0.055, §P ϭ 0.07, and ʈP ϭ 0.09 (each vs. placebo).
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
Ziegler and Associates
formulation. The coefficient of variation
Diabetes Association. Diabetes Care 28:
(R. Hermann, unpublished observations).
related to increased mortality in diabeticpatients: a survival analysis using an ac-
celerated failure time model. J Clin Epide-
A c i d i n E n d o t h e l i a l D y s f u n c t i o n
that a response of at least 50% reduction
definition, the response rates were 50 –
drome resulted in a significant increase in
betes. Diabet Med 21:976 –982, 2004
vasodilation of the brachial artery by 44
dose of oral ALA q.d. is 2.7. Whether the
6. Galer BS, Gianas A, Jensen MP: Painful
placebo treatment after 4 weeks. This ef-
description, and quality of life. Diabetes
7. Finnerup NB, Otto M, McQuay HJ, Jensen
our finding that neuropathic deficits such
proposal. Pain 118:289 –305, 2005
tion via anti-inflammatory and antithrom-
faye S: Vascular factors and metabolic in-
infusion of 600 mg ALA exerts an acute ef-
teractions in the pathogenesis of diabetic
fect on microcirculation in patients with di-
neuropathy. Diabetologia 44:1973–1988,
impairment of nitric oxide–mediated vaso-
9. Ziegler D: Thioctic acid: a critical review
dilation in diabetes has been attributed to
of its effects in patients with symptomatic
increased vascular oxidative stress. At this
diabetic polyneuropathy. Treat Endocrinol
point, acute infusion of ALA improved ni-
that resulting from intravenous treatment
10. Tesfaye S: Symptomatic diabetic periph-
dependent vasodilation in diabetic patients
the PKC  inhibitor ruboxistaurin: trial
ously reported (14). It is notable that this
design (Abstract). Diabetologia 48 (Suppl.
favorable safety profile for the low dose.
11. Bril V, Buchanan RA: Long-term effects of
tinued the study, whereas with the higher
function in patients with diabetic sensori-
rates of gastrointestinal side effects, 600
motor polyneuropathy. Diabetes Care 29:
12. Vincent AM, Russell JW, Low P, Feldman
EL: Oxidative stress in the pathogenesis of
diabetic neuropathy. Endocr Rev 25:612–
Acknowledgments — This study was sup-
13. Ziegler D, Sohr CGH, Nourooz-Zadeh J:
many. In addition to the authors listed, thefollowing colleagues contributed equally to
in relation to the severity of diabetic poly-
the study: Natalia Chernikova, MD; Barbara
neuropathy and autonomic neuropathy.
ing 21 and 48%, respectively. The rate of
Ellers-Lenz, Dipl.math.oec; Igor Strokov, MD;
Diabetes Care 27:2178 –2183, 2004
Julio Wainstein, MD; and Hans J. Tritschler,
14. Ziegler D, Nowak H, Kempler P, Vargha
reported in the ␣-Lipoic Acid in Diabetic
dant ␣-lipoic acid: a meta-analysis. DiabetReferences
1. Shaw JE, Zimmet PZ, Gries FA, Ziegler D:
15. Ametov A, Barinov A, O’Brien P, Dyck PJ,
q.d. intravenously (32). However, a direct
Textbook of Diabetic Neuropathy. Gries FA,
comparison of these studies is not possi-
janovic M, Samigullin R, Schuette K,Strokov I, Tritschler HJ, Wessel K, Ya-
ble because of the different routes of ad-
senko JM: Diabetic somatic neuropathies.
used. The oral HR (high release) formula-
Diabetes Care 27:1458 –1486, 2004
with ␣-lipoic acid: the SYDNEY trial. Di-
tion of ALA used in this study was specif-
3. Boulton AJM, Vinik AI, Arezzo JC, Bril V,
ically developed to reduce the relatively
16. Ruhnau K-J, Meissner HP, Finn J-R, Rel-
high variability in drug plasma levels after
dich D, Tritschler HJ, Mehnert H, Ziegler
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
␣-Lipoic acid in diabetic polyneuropathy
23. Yorek MA, Coppey LJ, Gellett JS, David-
the antioxidant thioctic acid (␣-lipoic
son EP, Lund DD: Effect of fidarestat and
29. Haak ES, Usadel KH, Kohleisen M, Yilmaz
␣-lipoic acid on diabetes-induced epin-
A, Kusterer K, Haak T: The effect of ␣-li-
ropathy. Diabet Med 16:1040 –1043,
eurial arteriole vascular dysfunction. Exp
poic acid on the neurovascular reflex arc
17. Dyck PJ: Detection, characterization, and
24. Kunt T, Forst T, Wilhelm A, Tritschler H,
sessed by capillary microscopy. Microvasc
staging of polyneuropathy: assessed in di-
abetics. Muscle Nerve 11:21–32, 1988
Zschaebitz A, Stofft E, Beyer J: ␣-Lipoic
30. Heitzer T, Finckh B, Albers S, Krohn K,
18. Dyck PJ, Karnes JL, O’Brien PC, Litchy
Kohlschu¨tter A, Meinertz T: Beneficial ef-
fects of ␣-lipoic acid and ascorbic acid
ide-mediated vasodilation in diabetic pa-
and staged severity. Neurology 42:1164 –
products. Clin Sci (Lond) 96:75– 82, 1999
tients: relation to parameters of oxidative
stress. Free Radic Biol Med 31:53– 61,
31. Reljanovic M, Reichel G, Rett K, Lobisch
Nawroth PP: ␣-Lipoic acid decreases ox-
M, Schuette K, Mo¨ller W, Tritschler H-J,
perimental diabetic neuropathy. Diabetes
uria. Free Radic Biol Med 22:1495–1500,
with the antioxidant thioctic acid (␣-li-
26. Androne L, Gavan NA, Veresiu IA, Orasan
Tritschler HJ: Effects of ␣-lipoic acid on
R: In vivo effect of lipoic acid on lipid
ized double blind placebo controlled trial
(ALADIN II). Free Radic Res 31:171–179,
interaction with essential fatty acids. Dia-
neuropathy. In Vivo 14:327–330, 2000
21. Mitsui Y, Schmelzer JD, Zollman PJ, Mit-
Meißner HP, Lobisch M, Schu¨tte K, Gries
athy with the anti-oxidant ␣-lipoic acid: a
nerve. J Neurol Sci 163:11–16, 1999
22. Coppey LJ, Gellett JS, Davidson EP, Dun-
trolled trial (ALADIN Study). Diabetologia
(ISLAND) study. Circulation 111:343–
33. Abbott CA, Vileikyte L, Williamson S,
28. Haak E, Usadel KH, Kusterer K, Amini P,
locity, and vascular reactivity of epineur-
fects of ␣-lipoic acid on microcirculation
risk factors for diabetic neuropathic foot
ial arterioles of the sciatic nerve. Diabetes
in patients with peripheral diabetic neu-
ulceration. Diabetes Care 21:1071–1075,
ropathy. Exp Clin Endocrinol Diabetes 108:
DIABETES CARE, VOLUME 29, NUMBER 11, NOVEMBER 2006
Martim de Gouveia e Sousa que «em Lisboa se vendia a sorrelfa» e «onde se abocanhavaSe a obra lírica nada traz de particular, fundando-sea dignidade da rainha» (ver Rego), alude-se « aos amores numa incaracterística toada debutante, a tradução de Lessáficos da rainha D. Amélia, por quem Mouzinho de Civilisés (1906) de Claude Farrère (1876-1957) trouxe-lhe aAlbuquerque
MP 0636355 SAMA 74851 MPS 01/39363 PR 0511242WHAT ARE DERMAL FILLERS?Dermal fillers are injectable treatments to reduce the appearance of lines and wrinkles. The most widely usedproducts contain hyaluronic acid such as Restylane, Perlane and Juvederm.Ask your doctor which filler is beingused since the regulations at present are not very demanding and a product can be promoted after min
 ␣-Lipoic acid in diabetic polyneuropathy
␣-Lipoic acid in diabetic polyneuropathy