Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Schwindel-sprechstunde.de
Articles Screening for dementia with the Memory Impairment Screen
H. Buschke, MD; G. Kuslansky, PhD; M. Katz, MPH; W.F. Stewart, PhD;
M.J. Sliwinski, PhD; H.M. Eckholdt, PhD; and R.B. Lipton, MD
Article abstract—Objectives: To validate a sensitive and specific screening test for AD and other dementias, assess its reliability and discriminative validity, and present normative data for its use in various applied settings. Background: To improve discrimination in screening for AD and dementia, we developed the Memory Impairment Screen (MIS), a 4-minute, four-item, delayed free- and cued-recall test of memory impairment. The MIS uses controlled learning to ensure attention, induce specific semantic processing, and optimize encoding specificity to improve detection of dementia. Meth- ods: Equivalent forms of the MIS were given at the beginning and end of the testing session to assess alternate forms reliability. Discriminative validity was assessed in a criterion sample of 483 aged individuals, 50 of whom had dementia according to Diagnostic and Statistical Manual of Mental Disorders (3rd ed., revised) criteria. Results: The MIS had good alternate forms reliability, high construct validity for memory impairment, and good discriminative validity in terms of sensitivity, specificity, and positive predictive value. We present normative data for use in settings with different base rates (prevalences) of AD and dementia. Conclusion: The MIS provides efficient, reliable, and valid screening for AD and other dementias.
There are urgent scientific and public health reasons
other metabolic causes, and infections.12,13 Effective
to develop effective methods of screening for AD and
recognition of the dementia syndrome is an impor-
other dementing disorders, especially in the early
tant step toward establishing and addressing a spe-
clinical stages.1 Individuals with early disease may
not consult physicians or may not mention their cog-
Despite several decades of research, the 1996 US
nitive complaints.2 They may be unaware of their
Agency for Health Care Policy and Research Clinical
decline or believe that their memory problems are
Practice Guideline on recognition and initial assess-
part of the normal aging process.3 Even if they report
ment of Alzheimer’s disease and related dementias14
symptoms, dementia often goes undetected and un-
indicates that there is no evidence to recommend one
screening test over another. Because memory im-
Dementia is a clinical syndrome with many reme-
pairment is often the earliest feature of AD, a very
diable causes. Two pharmacologic treatments for AD
brief test for memory impairment with sufficient
have been approved,5-7 and other pharmacologic
sensitivity, specificity, and positive predictive value
treatments are being developed.8,9 Early detection is
(PPV) should serve as a good screening test for AD
important because treatment may be more effective
and other dementias with memory impairment.
early in disease when useful cognitive function can
Very brief memory tests that assess (delayed) re-
still be preserved.10,11 AD may soon meet criteria for
call of three or four words are used in clinical prac-
community-based “tertiary prevention” programs.1
tice to screen for memory impairment15 and are
Other treatable causes of dementia include subdural
included in mental status assessments.16-22 However,
such very brief three- or four-word tests for memory
See also page 224
From The Saul R. Korey Department of Neurology (Drs. Buschke and Kuslansky, M. Katz, and Drs. Sliwinski, Eckholdt, and Lipton), Einstein Aging Study(Drs. Buschke and Kuslansky, M. Katz, and Drs. Sliwinski, Eckholdt, and Lipton), Rose F. Kennedy Center for Mental Retardation and Human Development(Drs. Buschke, Kuslansky, Sliwinski, and Eckholdt), and Department of Epidemiology and Social Medicine (Dr. Lipton), Albert Einstein College of Medicine,Bronx, NY; Department of Epidemiology (Dr. Stewart), School of Public Health, The Johns Hopkins University, Baltimore, MD; and Innovative MedicalResearch (Drs. Stewart and Lipton), Towson, MD.
Supported by NIA grants AG03949 and AG12448, and NICHD grant HD-01799.
Presented in part at the annual meeting of the American Neurological Association; San Diego, CA; September 1997.
Received March 16, 1998. Accepted in final form September 12, 1998.
Address correspondence and reprint requests to Dr. Herman Buschke, Department of Neurology, Kennedy 912, Albert Einstein College of Medicine, Bronx,NY 10461.
Copyright 1999 by the American Academy of Neurology
impairment have a high rate of false-negative errors
Health Care Financing Administration (HCFA) lists for
(low sensitivity) or false-positive errors (low specific-
the area adjacent to our clinical research center. According
ity) and may yield different results depending on the
to the HCFA, their lists include 97% of individuals over
words used.23-25 The 10-word Delayed Word Recall
the age of 65. The eligibility criteria for inclusion in this
Test26 discriminates between nondemented elderly
study were age 65 and over, ambulatory, and adequate
individuals and mild AD patients with high sensitiv-
ability to understand and speak English. In comparison
ity (89%) and specificity (98%) but takes longer to
with the entire HCFA sample for the relevant segment of
administer because the list is presented twice, and
the Bronx, our study sample was slightly older but other-
each time the individual must make up a sentence
wise similar to the community in terms of sex (36% male),
for each word. A very brief, well-standardized, accu-
racial distribution (80.7% white, 16.2% African American,
rate screening test for memory impairment and de-
and 2.7% other), and education (16.6% had fewer than 9
mentia might find broader use in clinical practice.
We previously demonstrated that the Double
These participants received a neuropsychological test
battery as well as medical, epidemiologic, social, and be-
Memory Test (DMT) has high discriminative validity
havioral questions every 18 months. A neurologic evalua-
for AD and related dementias in comparison with
tion was performed on those participants who had Blessed
standard memory tests that do not optimize encod-
Information Memory and Concentration (BIMC)16 test er-
ing specificity.27,28 The advantage of the DMT, rela-
ror scores of greater than 8, a total recall score of 44 or less
tive to conventional memory tests, is greatest for the
on the FCSRT,29,31 or who were suspected of having demen-
patients with mild disease; the DMT has a sensitiv-
tia based on self-report, informant report, or observations
ity of 93% and a specificity of 99% for the diagnosis
of the testers. Additional diagnostic testing, ordered by
of mild dementia.28 Although these unusually high
the neurologist, included neuroimaging, blood tests, and
sensitivities and specificities suggest that the DMT
other evaluations as needed. A diagnosis of dementia was
may be useful in detecting early dementia, it is not
made according to Diagnostic and Statistical Manual of
suitable as a screening test. It has 128 items, must
Mental Disorders (3rd ed., revised) (DSM-III-R) criteria,32
be administered by a trained tester in two parts, and
and a diagnosis of AD was based on National Institute of
requires approximately 20 minutes to complete. The
Neurological and Communicative Disorders and Stroke–
multi-trial Free and Cued Selective Reminding Test
Alzheimer’s Disease and Related Disorders Assocation
(FCSRT),29 a forerunner of the DMT, also uses con-
(NINCDS-ADRDA) criteria.33 Of the 50 participants with
trolled learning and cued recall but, because of its
DSM-III-R dementia (yielding a sample base rate of
length, is also not suitable for screening.
10.4%), 39 met criteria for AD. The other 433 participants
The Memory Impairment Screen (MIS) is a brief,
four-item delayed free- and cued-recall memory im-
The participants received the MIS as part
pairment test that also uses controlled learning and
of a neuropsychological test battery that included the
cued recall to optimize encoding specificity. Con-
Wechsler Adult Intelligence Scale–Revised,34 the Logical
trolled learning29 requires the individual to search
Memory I and Verbal Paired Associates I subtests from the
for and identify a to-be-remembered item in response
Wechsler Memory Scale–Revised,35 the FCSRT,29,31,36 the
to its category cue. The category cues are also used to
BIMC test,16 and the Zung Depression Scale.37 All partici-
elicit retrieval by cued recall. Using the same cues at
pants scoring in the depressed range on the Zung Depres-
acquisition and retrieval coordinates acquisition and
sion Scale (Ն50) were clinically assessed by a study
retrieval, optimizing encoding specificity because
psychiatrist using the Structured Clinical Interview for the
“specific encoding operations performed on what is
DSM-III-R.38 Alternate forms of the MIS were adminis-
perceived determine what is stored and what is
tered at the beginning and the end of the neuropsycholog-
stored determines what retrieval cues are effective in
ical test session in counterbalanced order. Participants
providing access to what is stored.”30 We postulated
were tested individually and told before presentation of the
that improving retrieval by these procedures would
test items that they should remember the items so thatthey could recall them later. Each participant was pre-
provide a screening test with improved discrimina-
tive validity. To test the potential of the MIS as a
items to be recalled printed in 24-point uppercase letters.
screening test for AD and dementia, we assessed its
Each item belonged to a different category. The individual
reliability, construct validity with respect to a stan-
was asked to read the items aloud and then asked to iden-
dard memory test, and discriminative validity as a
tify and name each item (e.g., “potato”) when the tester
said its category cue (e.g., “vegetable”). The sheet was thenremoved. After a nonsemantic interference task (repeated
Methods.
counting from 1 to 20 and back) lasting approximately 2 to
consent as specified by the Committee on Clinical Investi-
3 minutes, the individual was asked for free recall of the
gations at Albert Einstein College of Medicine. Partici-
four items in any order. The category cues were then pre-
pants were 483 community-residing volunteers, 50 of
sented to elicit cued recall of only those items that were
whom had dementia, who participated in the Einstein Ag-
not retrieved by free recall. The number of items retrieved
ing Study, a longitudinal study of dementia and normal
by free recall and the number retrieved by cued recall were
aging. The sample included 286 community volunteers re-
cruited from senior centers and physician practices. In ad-
The MIS score is calculated as [2 ϫ (free re-
dition, 197 individuals were systematically sampled from
call)] ϩ [cued recall]. Simple free recall provides a single
January (2 of 2) 1999
score—the number of items retrieved by free recall. Cued
Table 1 Demographic and neuropsychological characteristics of
recall in the MIS provides a second score—the number of
items retrieved by cued recall. If cued recall of all items
were tested, a combined free- and cued-recall score would
be obtained by adding the total cued-recall score to thetotal free-recall score. However, in the MIS, cued recall is
tested only for those items that were not retrieved by free
recall. Because items retrieved by free recall also are re-
trieved by cued recall, the equivalent of a total cued-recallscore can be obtained by adding free recall (i.e., those
items that would also have been retrieved by cued recall)
to the actual cued recall obtained by testing only those
items that were not retrieved by free recall. Adding thisequivalent total cued-recall score to the free-recall score
results in an MIS score equal to [2 ϫ (free recall)] plus
(obtained) cued recall. Adding cued recall to free recall alsoincreases the range of scores (0 to 8), which may improve
Means (SD) are presented except for sample size and sex.
BIMC ϭ Blessed Information Memory Concentration test; WAIS-
R ϭ Wechsler Adult Intelligence Scale–Revised; MIS ϭ Memory
nate forms reliability using the intraclass correlation. In-
ternal consistency was determined using Cronbach’scoefficient alpha.
Construct validity of the MIS for detecting memory im-
dementia group was slightly older and had slightly less
pairment was assessed using the chance corrected kappa
education, although the gender composition of the two
statistic to measure the concordance between memory im-
groups was similar. The dementia group scored approxi-
pairment on the MIS and impairment as defined by perfor-
mately one-half SD unit higher ( p Ͻ 0.001) on the Zung
mance on the FCSRT. The MIS is intended to screen for
Depression Scale than did the nondementia group. Zung
memory impairment and is not intended as an index of
Depression Scale scores were not correlated with the MIS
memory ability. The FCSRT cut-score was selected based
scores for the demented (Spearman ϭ 0.09, p ϭ 0.53) or for
on its ability to distinguish individuals with and without
the nondemented groups (Spearman ϭ 0.002, p ϭ 0.96).
Based on clinical interviews by a psychiatrist of individu-
Discriminative validity of the MIS was assessed by cal-
als with Zung Depression Scale scores of Ն50, seven par-
culating the sensitivity and specificity of the MIS for de-
ticipants met DSM-III-R criteria for major depressive
tecting dementia and for detecting AD for various MIS
disorder, six of whom were in the nondemented group.
cut-scores. The base rate of dementia in our sample was
Alternate forms reliability for the MIS was
10.4% (50 of 483). Of the 50 demented participants, 39
assessed by administering one of two forms to a subset
(78%) met criteria for possible or probable AD.
(n ϭ 429) of clinically diagnosed demented and nonde-
Although normative data are often presented in the
mented participants at the beginning and end of a neuro-
form of percentiles or means and SDs, we present norms in
psychological evaluation. The intraclass correlation was
the form of the probability of dementia (or AD) given dif-
high, 0.69, indicating strong concordance between the two
ferent MIS cut-scores. To calculate the probability of de-
forms of the MIS and a high level of alternate forms reli-
mentia, one must know the test sensitivity and specificity
ability. Internal consistency also was good for both forms—
at each cut-score as well as the base rate of dementia.39,40
the coefficient alpha was 0.67 for both forms.
Because the base rate of dementia varies with setting as
well as age, we present normative data that cover a broad
a screening test for memory impairment as determined by
range of dementia base rates. Normative data are pre-
the 16-item multi-trial FCSRT.31 Memory impairment is
sented for various dementia base rates as the probability
identified by the FCSRT by a total free- plus cued-recall
of dementia or AD (i.e., the PPV) using each MIS score as a
score over all three trials of 44 or less. Classification of
memory impairment by the MIS (as defined by a score of 4
Probability of dementia or AD was calculated according
or less) was strongly associated with memory impairment
to Bayes’ theorem.39 The formula for PPV yields the pro-
as defined by the gold standard FCSRT (kappa ϭ 0.62).
portion of individuals who screen positive at a given cut-
score who actually have dementia (for a specific prevalence
tive validity of the MIS first as a screening test for demen-
rate). Note that the PPV also represents the probability of
tia in general and then specifically for clinically diagnosed
dementia for individuals with scores falling at or below a
AD. The trade-off between sensitivity and specificity of the
given score on the MIS in a sample with a given base rate
MIS as a screening test for dementia and AD as the cut-
of dementia. PPV is a useful index of the efficiency of a
score varies is shown by the receiver operating character-
screening test in different applied settings that have differ-
istic (ROC) curves41,42 in figure 1 (all dementia, including
ent base rates of dementia. The negative predictive value
AD, versus nondemented) and figure 2 (only AD versus
(NPV) is the proportion of individuals who screen negative
nondemented). The area under the ROC curve is regarded
as a useful index of a diagnostic test’s performance. Thearea under the ROC curve for discrimination of dementia
Results.
Demographic and neuropsychological character-
(including AD) is 0.94. The area under the ROC curve for
istics of the study sample are summarized in table 1. The
discrimination of AD is even larger, 0.97. These figures
January (2 of 2) 1999 Table 2 Dementia sensitivity and specificity of each MIS score with corresponding probabilities of dementia (PPV) at different base rates Figure 1. Receiver operating characteristics of the Mem-ory Impairment Screen as a screening test for dementia
MIS ϭ Memory Impairment Screen; PPV ϭ positive predictive
graphically indicate that the specificity of the MIS is con-
(see Discussion), a cut-score of 4 provides a high level of
sistently high for a large range of sensitivities. The influence
sensitivity (0.80), specificity (0.96), and PPV (Ͼ0.69) for all
of the sensitivity-specificity trade-off on the usefulness of the
base rates except the lowest at 5%. Because the base rate
MIS as a screening test for AD and dementia is examined in
of dementia in the current sample is approximately 10%,
the following section on normative data.
approximately 70% of study participants who scored 4 or
less had some type of dementia. The NPV reflects the
specificity, and PPV (i.e., probability of dementia or AD)
probability that an individual who screens negative does
for each cut-score on the MIS for different base rates of
not have disease. A cut-score of 4 provides excellent NPVs
dementia. Performance at or below the cut-score is taken
at low base rates of dementia. For example, at a base rate
as evidence of dementia. Sensitivity measures the propor-
of 5% the NPV is 0.99; at a base rate of 10% the NPV is
tion of those with dementia who are correctly identified as
0.98; at a base rate of 20% the NPV is 0.95. Thus one can
demented. Specificity measures the proportion of those
be reasonably sure that those who screen negative do not
without dementia who are correctly identified as nonde-
mented. PPV is the proportion of those who meet a given
The results are similar when the analysis is restricted
cut-score (i.e., screen positive) and actually have dementia.
to cases of AD and controls (see table 3). A MIS cut-score of
Table 2 displays the sensitivity and specificity for de-
4 had a sensitivity of 0.87 for AD, which is slightly higher
tecting any type of dementia using each level of MIS score
than the sensitivity for all dementia. This differential
as a cutoff. Although the selection of an optimal cut-score
sensitivity is expected because (early) memory impairment
will depend on the intended clinical or research application
Table 3 AD sensitivity and specificity of each MIS score with corresponding probabilities of AD (PPV) at different base rates Figure 2. Receiver operating characteristics of the Mem-
MIS ϭ Memory Impairment Screen; PPV ϭ positive predictive
ory Impairment Screen as a screening test for AD.January (2 of 2) 1999
is the hallmark of AD but not of all other (non-AD)
using the FCSRT as the gold standard; the FCSRT
has an empirically based cut-score for dementia-
To examine how the MIS performed for different levels
related memory impairment.31 Classifications by the
of dementia severity, we assessed discriminative validity
MIS and by the longer FCSRT were quite similar,
separately for demented individuals who fell at or below 13
supporting the view that the MIS measures the same
(mild) and at or above 14 (moderate) on the BIMC test.
The sensitivity for mildly demented individuals with any
type of dementia at an MIS cut-score of 4 is 0.69; for
of the MIS for dementia and AD was assessed in a
moderately demented individuals the sensitivity is 0.92.
large sample of individuals with and without clini-
When analyses are restricted to only AD dementia, the
cally diagnosed dementia. In clinical practice, when
sensitivity for mildly demented individuals is 0.79, and for
older patients present with memory or cognitive
moderately demented individuals the sensitivity is 0.95.
complaints, the first issue is to diagnose or exclude
The demographic variables age, education, and gender
as well as their interactions (with each other and with the
dementia of any sort (e.g., AD, vascular dementia,
MIS) were added to a logistic regression model as covari-
dementia with Lewy bodies). If dementia is present,
ates to determine their effect on predictive accuracy. None
a more specific etiologic workup is essential. Thus, it
of these demographic variables or interaction terms was
is clinically important for a screening instrument to
significant at the 0.05 level. When the Zung Depression
identify dementia syndromes with diverse etiologies.
Scale score and its interaction were added to the logistic
Although we present normative data separately for
regression model, they were not significant at the 0.05
detecting all dementia (with memory impairment) or
level. The ethnicity of the 17 false positives was examined
only AD, we believe that the discriminative validity
to determine the possible influence of ethnic background
data for detecting all dementia is most relevant for
on classification by the MIS. Of the 17 nondemented indi-
the majority of clinical and research applications.
viduals who failed the MIS (cut-score ϭ 4), 2 (11.7%) were
Discriminative validity of the MIS is influenced by
African Americans, which is less than expected given the
dementia severity. In moderate dementia, sensitivity
sample composition of 16.2% African Americans. Thus, in-
is 0.92 for all dementia and 0.95 for AD. Although
dividuals of minority backgrounds were no more likely to
sensitivity for mild dementia is lower, it is reason-
be incorrectly identified as memory impaired by the MIS
ably high— 0.69 for all dementia and 0.79 for AD.
The number of participants with non-Alzheimer de-mentia is relatively small; further experience with
Discussion.
memory impairment, dementia, and AD that is brief,
The sensitivity and specificity of the MIS com-
easy to use, reliable, and valid. It is based on our
pares favorably with results in other samples for
previous research demonstrating that memory tests
longer screening tests for dementia such as the
with high encoding specificity, such as the DMT and
BIMC test16 and the Mini-Mental State Examination
the FCSRT, have higher discriminative validity for
(MMSE).17 Because the BIMC test was used by clini-
AD and for dementia in general.27-29,31,36 The MIS
cians in this study to assign diagnoses, we cannot
uses category cues during acquisition (learning) to
compare the MIS and the BIMC test obtained in this
ensure attention, induce semantic processing, and
study and must rely on analysis of the MMSE and
optimize encoding specificity, and during retrieval to
the BIMC test in other studies. Recent analyses of
benefit from encoding specificity, increase retrieval,
neuropsychological tests for diagnosis of dementia by
and improve discrimination. Because the MIS is a
Wilder et al.42 and Meiran et al.40 reported the dis-
screening test, individuals who fail it are referred for
criminative validity of the MMSE and the BIMC test
definitive diagnostic assessment. Individuals who
for detecting AD. When Wilder et al.42 selected cut-
pass the test may be rescreened in the future de-
scores for these tests so that sensitivity is high
pending upon the context of screening. In this sec-
(0.90), their specificities are unimpressive— 0.44 for
tion we summarize the psychometric properties of
the MMSE and 0.60 for the BIMC test. Data from
the MIS, illustrate how the normative data might be
Meiran et al.40 indicate that when MMSE sensitivity
used in particular clinical and research applications,
is 0.91, MMSE specificity is only 0.25. The specificity
of MIS for detecting AD is 0.96 when sensitivity is
We demonstrated that the MIS has high alternate
set to 0.87 (see table 3). These data suggest that the
forms reliability, indicating that the two forms are
MIS may be a more sensitive screen for AD than
similar and that individuals perform in a highly re-
these commonly used mental status examinations.
peatable fashion. The high reliability scores show
Because the sensitivity and specificity of the MIS in
that the alternate forms of the MIS can be used for
this study are compared with the sensitivity and
repeated administration. The availability of equiva-
specificity of the MMSE and the BIMC test in other
lent alternate forms is an advantage in applications
studies, these comparisons must be interpreted with
that require serial screening. There was a high de-
caution; the populations used in different studies
gree of internal consistency for the two forms of the
may have been different. In particular, the influence
MIS (Cronbach’s alpha ϭ 0.67 for both).
of education and cultural background on the relative
performance of the MIS, the MMSE, and the BIMC
as a screen for memory impairment was evaluated
test requires further study.43,44 Although the MMSE
January (2 of 2) 1999
and the BIMC test are influenced by education, at
ity (0.91). How accurately this cut-score classifies
least in this sample education did not affect the dis-
patients will depend on the dementia base rate in
the clinical setting. In a clinic-based sample of indi-
viduals with memory complaints we might reason-
performance on cognitive tests and enters into the
ably expect a dementia base rate of 20%. At that
differential diagnosis of dementia.38 In the current
base rate, a MIS cut-score of 5 corresponds to a 0.72
study, Zung Depression Scale scores were not corre-
probability of dementia. This means that 72% of
lated with MIS scores for the demented or for the
those meeting a MIS cut-score of 5 will have demen-
nondemented groups. Only seven participants met
tia (i.e., PPV ϭ 0.72), and the sensitivity of 0.86
DSM-III-R criteria for major depression, and of these
means that only 14% of all the demented patients
six were in the nondemented group. Of the 17 false-
will be missed by the screen. In this setting the NPV
positive instances in the study (MIS of 4 or less, but
of 0.96 means that of those who screen negative, only
not clinically demented), only one had depression.
4% would prove to have dementia on a definitive
We do not have adequate data to draw firm conclu-
sions about the influence of moderate or severe de-
In contrast to a purely clinical application, re-
pression on MIS performance, because of small
search applications may require higher specificity to
numbers of depressed individuals. However, there is
efficiently identify potentially diseased individuals.
little evidence to suggest that depression influenced
When the base rate of dementia is low, screening can
MIS performance in our study results.
be used to identify individuals likely to have demen-
tia on definitive evaluation. For example, if the base
mative data needed to select cut-scores for the MIS.
rate of dementia is 10% in the target population, a
The PPVs, which reflect the probability of dementia
researcher might select from table 2 a MIS cut-score
for individuals falling at or below a MIS cut-score for
of 3, which has a very high specificity (0.98). At that
a given base rate, provide an estimate of how likely
specificity the PPV is 0.78, which means that 78% of
those who screen positive will prove to have disease
those who screened positive will meet criteria for
upon definitive assessment. We provide the following
dementia. Unlike the clinician, whose choice of cut-
examples to illustrate how to use the MIS or any
score will often be driven by the need to maximize
screening test to classify individuals. A clinician
sensitivity, the researcher may require high specific-
could be confident about classifying individuals scor-
ity to yield a high PPV. But even with this more
ing 4 or less on the MIS as demented because the
restrictive criterion, the NPV of 0.97 means that only
probability of being demented is 0.84 (at a base rate
3% of those who screen negative would prove to have
of 20%; see table 2). However, if the base rate were
dementia with a definitive assessment. Depending
only 5%, a clinician could not make such a confident
on the context, individuals who initially screen nega-
classification because the probability of dementia is
tive may be rescreened to identify individuals missed
only 0.52. In general, clinicians will need to adopt
lower (i.e., more stringent) cut-scores to maintain a
Limitations and future directions.
given level of confidence for samples with lower base
results apply only to use of the MIS as a screening
test for detection of dementia-related memory im-
To select an optimal cut-score, a clinician or re-
pairment, dementia, and AD in community-residing
searcher needs to consider the base rate of the de-
adults aged 66 to 97 years. Cut-scores selected from
mentia in the screened population as well as the
tables 2 and 3 may not have the same level of dis-
clinical or research goals of the screening program.
crimination in specific clinical applications because
For example, a clinician might chose a cut-score to
the distribution of MIS scores for demented and non-
maximize sensitivity so that impaired individuals
demented older adults in primary care settings may
are not missed by the screen, whereas a researcher
not be equivalent to that observed in a sample of
conducting clinical trials might wish to maximize the
community volunteers. Although the current results
PPV so that only those with a very high probability
are encouraging, additional field studies are required
of dementia screen positive and are enrolled in the
to verify the validity of the MIS in screening for
memory impairment and dementia in primary care
settings. An important direction for future research
of the normative data presented in tables 2 and 3
would be to develop MIS norms for use in specific
will depend on the clinical or research goals of the
screening program. For a clinical application in
An additional concern is that the clinical diagnosis
which early diagnosis is important and follow-up
of dementia is a fallible gold standard, although we
testing for definitive diagnosis is safe and inexpen-
assigned diagnoses with great care using contempo-
sive, optimal sensitivity is important. In this case, a
rary research criteria. In this sample, individuals
missed diagnosis would be undesirable given the lost
with preclinical dementia may not have crossed the
opportunity for treatment of AD or other types of
threshold required for diagnosis. If such individuals
dementia. Accordingly, a clinician might use the
have memory impairment on the MIS, they appear
data in table 2 to select a MIS cut-score of 5, which
as false positives in our assessment of discriminative
has a reasonably high sensitivity (0.86) and specific-
validity. Of the 17 individuals considered false posi-
January (2 of 2) 1999
tives (MIS score of 4 or less but not clinically de-
13. Tatemichi T, Sacktor N, Mayeux R. Dementia associated with
mented), 12 had a Clinical Dementia Rating45 score
cerebrovascular disease, other degenerative diseases, andmetabolic disorders. In: Terry R, Katzman R, Bick KE, eds.
of 0.5 (i.e., questionable dementia) and four devel-
Alzheimer’s disease. New York: Raven Press, 1994:123–166.
oped DSM-III-R dementia by the next wave of
14. U.S. Agency for Health Care Policy and Research. Recognition
follow-up 18 months later. Although we do not have
and initial assessment of Alzheimer’s disease and related de-
adequate data to comment on the discriminative va-
mentias. Clinical Practice Guideline No. 19. Silver Springs,MD: U.S. Agency for Health Care Policy and Research, 1996.
lidity of the MIS for preclinical AD, it appears that
15. Petersen RC. Memory assessment at the bedside. In: Yanagi-
the preclinical group may account for a substantial
hara T, Petersen R, eds. Memory disorders. New York: Marcel
proportion of the false positives, arguably leading to
16. Blessed G, Tomlinson R, Roth M. The association between
quantitative measures of dementia and of senile changes in
One final and important limitation of the MIS is
the cerebral gray matter of elderly subjects. Br J Psychiatry
that it is a screening test and should not be used in
isolation to make clinical diagnoses of dementia. By
17. Folstein M, Folstein S, McHugh P. A practical method for
grading the cognitive state of patients for the clinician. J Psy-
identifying individuals with a very high (or very low)
likelihood of dementia, a good screening test can play
18. Strub R, Black F. The mental status examination in neurol-
an important part in the diagnostic process. No
screening test should replace a comprehensive clini-
19. Teng E, Chui H. The modified Mini-Mental State (3MS) exam-
ination. J Clin Psychiatry 1987;48:314 –317.
cal evaluation. The MIS is intended to identify for
20. Kokmen E, Naessens J, Offord K. A short test of mental
clinical evaluation individuals who are likely to have
status: description and preliminary results. Mayo Clin Proc
21. Weintraub S, Mesulam M. Mental state assessment of young
and elderly adults in behavioral neurology. In: Mesulam M,
Acknowledgment
ed. Principles of behavioral neurology. Philadelphia: FA
The authors thank Anna Sapozhnik Miller, Betty Forro, Charlotte
Magnotta, Maria Luisa Giraldi, and Mary Joan Sebastian for
22. Kokmen E, Smith G, Petersen R, Tangalos E, Ivnik R. The
their assistance with data collection, and Drs. Randall Berliner
short test of mental status: correlations with standardized
and Howard Crystal for assistance with clinical evaluations and
psychometric testing. Arch Neurol 1991;48:725–728.
23. Guilmette T, Tshoh J, Malcolm C. Orientation and three-word
recall in predicting memory: age effects and false-negativeerrors. Neuropsychiatry Neuropsychol Behav Neurol 1995;8:
Disclosure
The Albert Einstein College of Medicine owns the copyright and
24. Cullum C, Thompson L, Smernoff E. Three-word recall as a
makes this test available as a service to the research community
measure of memory. J Clin Exp Neuropsychol 1993;15:321–
but licenses the test for commercial use.
25. White T, Bauer R, Bowers D, Crosson B, Kessler H. Recall of
three words after five minutes: its relationship to performance
References
on neuropsychological memory tests. Appl Neuropsychol 1995;2:130 –138.
1. Wilcock G, Ashworth D, Langfield J. Detecting patients with
Alzheimer’s disease suitable for drug treatment. Br J Gen
26. Knopman DS, Ryberg S. A verbal memory test with high
predictive accuracy for dementia of the Alzheimer type. Arch
2. Ross G, Abbott R, Petrovitch H, et al. Frequency and charac-
teristics of silent dementia among elderly Japanese-American
27. Buschke H, Sliwinski M, Kuslansky G, Lipton RB. Aging,
encoding specificity and memory changes in the Double Mem-
3. Kotler-Cope S, Camp C. Anosognosia in Alzheimer’s disease.
ory Test. J Int Neuropsychol Soc 1995;1:483– 493.
Alzheimer Dis Assoc Disord 1995;9:52–56.
28. Buschke H, Sliwinski M, Kuslansky G, Lipton RB. Diagnosis
4. Callahan C, Hendrie HC, Tierney WM. Documentation and
of early dementia by the Double Memory Test: encoding spec-
evaluation of cognitive impairment in elderly primary care
ificity improves diagnostic sensitivity and specificity. Neurol-
patients. Ann Intern Med 1995;122:422– 429.
5. Farlow M, Gracon S, Hershey L, Lewis K, Sadowsky C, Dolan-
29. Buschke H. Cued recall in amnesia. J Clin Neuropsychol
Ureno J. A controlled trial of tacrine in patients with probable
Alzheimer’s disease. JAMA 1992;268:2523–2529.
30. Tulving E, Thomson D. Encoding specificity and retrieval pro-
6. Raskind M, Sadowsky C, Sigmund W, Beitler P, Auster S.
cesses in episodic memory. Psychol Rev 1973;80:352–372.
Effects of tacrine on language, praxis, and noncognitive be-
31. Grober E, Buschke H, Crystal H, Bang S, Dresner R. Screen-
havioral problems in Alzheimer’s disease. Arch Neurol 1997;
ing for dementia by memory testing. Neurology 1988;38:900 –
7. Gelmacher D. Donepezil (Aricept) therapy for Alzheimer’s dis-
32. American Psychiatric Association. Diagnostic and statistical
ease. Compr Ther 1997;23:492– 493.
manual of mental disorders. 3rd ed, revised. Washington, DC:
8. Schordert M. Alzheimer’s disease: fundamental and therapeu-
American Psychiatric Association, 1987.
tic aspects. Experientia 1995;51:99 –105.
33. McKhann G, Drachman D, Folstein M, Katzman R, Price D,
9. Van Reekum R, Black S, Conn D, Clarke D. Cognition-
Stadlan E. Clinical diagnosis of Alzheimer’s disease: report of
enhancing drugs in dementia: a guide to the near future. Can
the NINCDS-ADRDA Work Group under the auspices of De-
J Psychiatry 1997;42(suppl 1):35s–50s.
partment of Health and Human Services Task Force on Alz-
10. Khachatorian Z, Phelps C, Buckholtz N. The prospect of devel-
heimer’s Disease. Neurology 1984;34:939 –944.
oping treatments for Alzheimer’s disease. In: Terry R, Katz-
34. Wechsler D. Wechsler Adult Intelligence Scale–Revised. New
man R, Bick K, eds. Alzheimer’s disease. New York: Raven
York: The Psychological Corporation, 1981.
35. Wechsler D. Wechsler Memory Scale–Revised. San Antonio,
11. Gauthier S, Thal L, Rosser M. The future diagnosis and treat-
TX: The Psychological Corporation, 1987.
ment of Alzheimer’s disease. In: Gauthier S, ed. Clinical diag-
36. Buschke H. Criteria for identification of memory deficits: im-
nosis and management of Alzheimer’s disease. London:
plications for the design of memory tests. In: Gorfein D, Hoff-
man RR, eds. Memory and learning: the Ebbinghaus
12. Siu A. Screening for dementia and investigating its causes.
Centennial Conference. Hillsdale, NJ: Lawrence Erlbaum As-
January (2 of 2) 1999
37. Zung W. A self-rating depression scale. Arch Gen Psychiatry
receiver operating characteristic (ROC) curve. Radiology 1982;
38. Spitzer R, Williams J, Gibbon M, First M. Structured Clinical
42. Wilder D, Cross P, Chen J, et al. Operating characteristics of
Interview for DSM-III-R. Nonpatient Edition (SCID-NP, ver-
brief screens for dementia in a multicultural population. Am J
sion 1). Washington, DC: American Psychiatric Press, 1990.
Geriatr Psychiatry 1995;3:96 –107.
39. Elwood R. Clinical discriminations and neuropsychological
43. Katzman R. Education and the prevalence of dementia and
tests: an appeal to Bayes’ theorem. Clin Neuropsychologist
Alzheimer’s disease. Neurology 1993;43:12–20.
44. Kittner SJ, White LR, Farmer ME, et al. Methodological is-
40. Meiran N, Stuss D, Guzman A, Lafleche G, Willmer J. Diag-
sues in screening for dementia: the problem of education ad-
nosis of dementia: methods for interpretation of scores of 5
justment. J Chron Dis 1986;39:163–170.
neuropsychological tests. Arch Neurol 1996;53:1043–1054.
45. Morris JC. The Clinical Dementia Rating (CDR): current ver-
41. Hanley J, McNeil B. The meaning and use of the area under a
sion and scoring rules. Neurology 1993;43:2412–2414. Tacrine use in nursing homes Implications for prescribing new cholinesterase inhibitors
D.R. Gifford, MD, MPH; K.L. Lapane, PhD; G. Gambassi, MD; F. Landi, MD;
V. Mor, PhD; and R. Bernabei, MD, for the SAGE Study Group*
Article abstract—Objective: To describe the use of tacrine in nursing home residents using data from a clinically based resident assessment instrument used by all US nursing homes. Methods: Data were from the Systematic Assessment of Geriatric Drug Use via Epidemiology (SAGE) database, a population-based data set with information on 329,520 patients admitted to all Medicare/Medicaid certified nursing homes in four US states (Maine, Mississippi, New York, and South Dakota) from 1992 through 1995. The SAGE database combines information from the Minimum Data Set (MDS) and the On-Line Survey and Certification Automated Record. We identified all residents receiving tacrine and up to five control residents per case matched on state, date of tacrine use, cognitive function, and dementia diagnosis. Results: A total of 1,640 (0.5%) nursing home residents received tacrine at least once. Only 38% of these residents had a diagnosis of AD documented on the MDS; regardless of dementia diagnosis, 25% had severe cognitive impairment, 35% were severely dependent in activities of daily living (ADL), and 17% had both severe cognitive and ADL impairment. Only 8% achieved a therapeutic dose of at least 120 mg/d. After adjusting for confounding variables, wandering and being physically abusive were the strongest predictors of tacrine use. Conclusions: A minority of nursing home residents received tacrine. Of those who did, a significant proportion were unlikely to benefit from its use because of their level of cognitive and ADL impairment, or because low doses were used. As new medications become available for dementia, MDS data can be used by nursing homes to monitor the use of these therapies.
The first cholinesterase inhibitor, tacrine, was ap-
tory setting, patients with a confirmed diagnosis of
proved in 1993 for the treatment of AD in the United
AD who receive tacrine exhibit, on average, statisti-
States.1 A second cholinesterase inhibitor, donepezil,
cally significant improvement on cognitive function
was approved in 1997.2 According to current guide-
tests.6-9 Data from these trials and others suggest
lines,3,4 cholinesterase inhibitors are only indicated
that tacrine also may affect other outcomes,7,10-12 but
for patients with a diagnosis of AD who have mild to
moderate dementia (e.g., Mini-Mental State Exami-
nation [MMSE] score of 10 to 26).1,2,5 In the ambula-
Little is known about the pharmacologic manage-
See also page 227
*See the Appendix on page 243 for a list of members of the SAGE Study Group.
From the Departments of Medicine (Dr. Gifford) and Community Health (Drs. Gifford, Lapane, Gambassi, and Mor) and the Center for Gerontology andHealth Care Research (Drs. Gifford, Lapane, Gambassi, and Mor), Brown University, Providence, RI; and Istituto di Medicina Interna e Geriatria (Drs. Gambassi, Landi, and Bernabei), Universita` Cattolica del Sacro Cuore, Rome, Italy.
This study was conducted while D.R.G. was a Pfizer/American Geriatric Society Postdoctoral Fellow and SURDNA fellow at the Brown Center forGerontology and Health Care Research. The study was also supported in part by the “Do Good Nursing Homes Achieve Good Outcomes?” project (NationalInstitute on Aging #AG11624) and by the “Changing Roles in Nursing Homes” project (#500-89-0046; US Department of Health and Human Services, HealthCare Financing Administration, to University of Michigan with subcontract to Brown University).
Received May 18, 1998. Accepted in final form October 24, 1998.
Address correspondence and reprint requests to Dr. David R. Gifford, Center for Gerontology and Health Care Research, Brown University, Box G-B 222,Providence, RI 02912; e-mail: [email protected]
Copyright 1999 by the American Academy of Neurology
kufa university Physiology College of Nursing second year student Ass. Lect :- Hisham Qassem M. Lecture No :-11 ــــــــــــــــــ ـــ ــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــــ�
Chiavi del Quaderno delle attività Episodio Per cominciare 1 Siamo all’università e si sta svolgendo un esame. 2 Risposta libera Guardiamo 2 bocciato significa che non ha superato l’esame; mattone è, nel linguaggio degli studenti, un libro molto voluminoso, con molte pagine; appello è un altro termine per dire “esame”; secchiona è una studentessa ( maschile: �
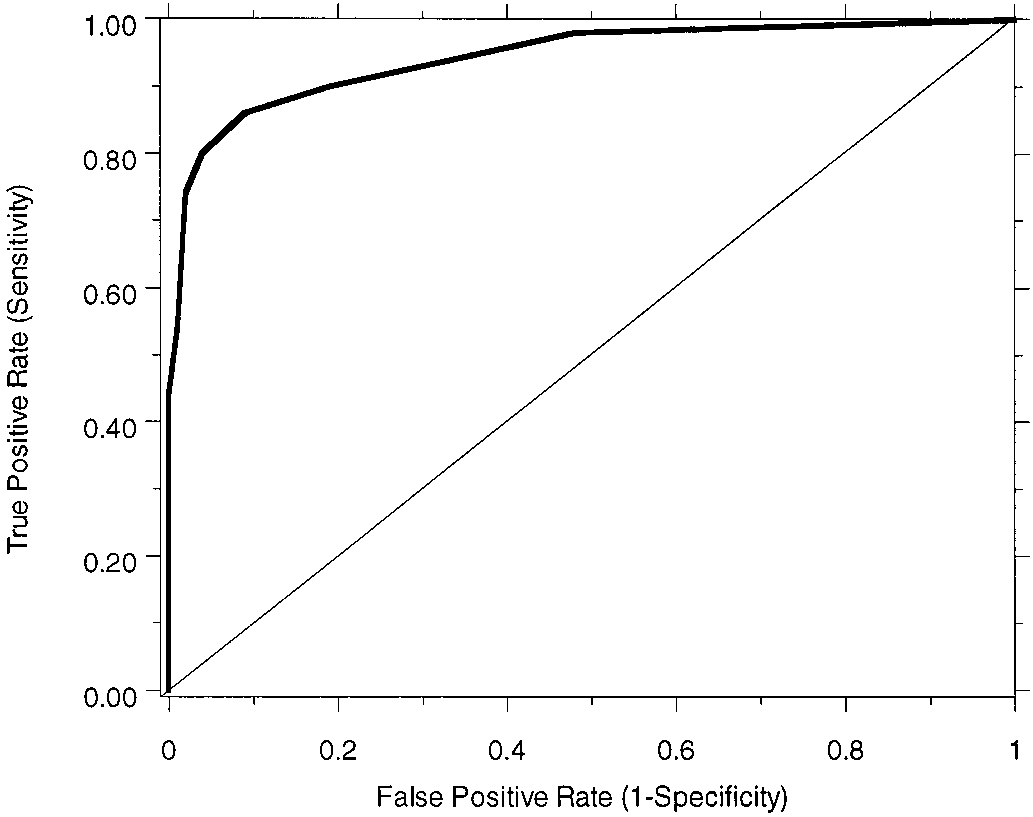
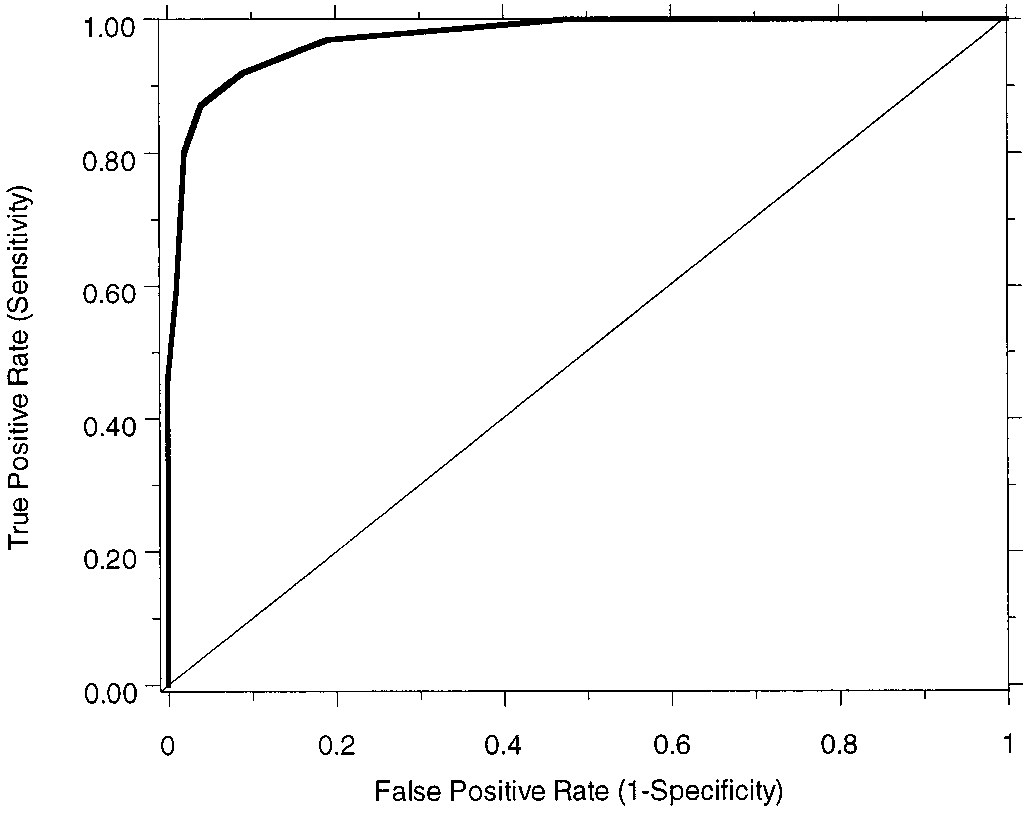 Table 2 Dementia sensitivity and specificity of each MIS score
Table 2 Dementia sensitivity and specificity of each MIS score