Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Inhaled bronchodilator administration during mechanical ventilation: how to optimize it, and for which clinical benefit?
JOURNAL OF AEROSOL MEDICINE AND PULMONARY DRUG DELIVERY Volume 21, Number 1, 2008 Mary Ann Liebert, Inc. Pp. 85–95 DOI: 10.1089/jamp.2007.0630
Inhaled Bronchodilator Administration During
Mechanical Ventilation: How to Optimize It, and
CLAUDE GUERIN, M.D., Ph.D.,1,2 THOMAS FASSIER, M.D.,2 FRÉDÉRIQUE BAYLE, M.D.,2
STÉPHANE LEMASSON, M.D.,2 and JEAN-CHRISTOPHE RICHARD, M.D., Ph.D.1,2
ABSTRACT Bronchodilators are frequently used in ICU patients, and are the most common medications administered by inhalation during mechanical ventilation. The amount of bronchodilator that deposits at its site of action depends on the amount of drug, inhaled mass, deposited mass, and particle size distribution. Mechanical ventilation challenges both inhaled mass and lung deposition by specific features, such as a ventilatory circuit, an endotracheal tube, and ven- tilator settings. Comprehensive in vitro studies have shown that an endotracheal tube is not as significant a barrier for the drug to travel as anticipated. Key variables of drug deposition are attachments of the inhalation device in the inspiratory line 10 to 30 cm to the endotra- cheal tube, use of chamber with metered-dose inhaler, dry air, high tidal volume, low respi- ratory frequency, and low inspiratory flow, which can increase the drug deposition. In vivo studies showed that a reduction by roughly 15% of the respiratory resistance was achieved with inhaled bronchodilators during invasive mechanical ventilation. The role of ventilatory settings is not as clear in vivo, and primary factors for optimal delivery and physiologic ef- fects were medication dose and device location. Nebulizers and pressurized metered-dose in- halers can equally achieve physiologic end points. The effects of bronchodilators should be carefully evaluated, which can easily be done with the interrupter technique. With the non- invasive ventilation, the data regarding drug delivery and physiologic effects are still lim- ited. With the bilevel ventilators the inhalation device should be located between the leak port and face mask. Further studies should investigate the effects of inhaled bronchodilators on patient outcome and methods to optimize delivery of inhaled bronchodilators during non- invasive ventilation. INTRODUCTION
halation route is to enhance the therapeutic/tox-icity index of the agent. However, a drawback is
BRONCHODILATORSAREFREQUENTLYUSEDin ICU lack/variability in efficiency. Because the clini-
patients receiving invasive mechanical venti-
cal/physiological efficiency largely depends on
lation (IMV) and commonly delivered through
amount of drug available at its site of action,
the inhalation route.(1) The main advantage of in-
namely 2 or muscarinic receptors in the smooth
1Creatis INSERM, CNRS, Lyon, France.
2Service de Réanimation Médicale, Hôpital de la Croix Rousse, Lyon, Université Claude Bernard, Lyon, France. GUERIN ET AL.
muscular cells in the wall of the bronchial tree,and given that there are numerous causes of druglosses in intubated patients, it has long beenthought that inhaled bronchodilators are ineffec-tive or exhibited markedly variable clinical ef-fects. Bench studies have shown that it should benot the case if the drug inhaled mass and de-posited mass are properly measured(2,3) and ven-tilator-related key factors involved in the drugdelivery carefully controlled.(2,4) A substantialamount of nebulized drug may actually reach itstarget in patients,(4) and guidelines have been de-veloped to optimize the administration of agentduring IMV.(3,5) With increasing use of noninva-sive ventilation (NIV) in ICU,(6) the issue of the
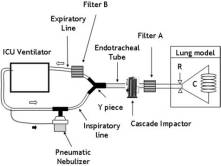
Schematic drawing of the experimental setup to
efficiency of inhaled bronchodilators in this set-
measure the pharmacological determinants of aerosol de-
ting has also to be examined. This review will go
position and to test the effects of various ventilator-re-
over pharmacological concepts of the aerosol ad-
lated factors on the drug lung deposition applied to in-
ministration, devices used to generate aerosol,
vasive mechanical ventilation. The pneumatic nebulizeris filled by the active drug and fed by the gas from the
ventilator-related factors for an optimal delivery
ICU ventilator at the recommended specific flow (usu-
of drug inhaled during IMV and NIV, indications
ally 6–8 L/min). The nebulizer is activated during the in-
and effects of inhaled bronchodilators in ICU pa-
spiratory phase (black-filled arrow), the tidal volume be-
tients during mechanical ventilation.
ing kept constant. The gas reaches filter A where theinhaled mass of the drug is determined. During inspira-tion some amount of nebulizer charge can be exhaled
Pharmacological concepts of aerosolization during
without being inhaled, and is captured in filter B. In sep-arate experiments, a cascade impactor can be inserted to
measure the particle size distribution of the aerosol. Theresistance (R) and/or compliance (C) of the lung model
During mechanical ventilation, the aerosolized
can be changed to mimick various clinical scenarii.
drug travels the inspiratory line and the endo-tracheal tube then deposits in the lungs, whilesome amounts flows out with the next expira-
of the nebulizer charge and 53% of the inhaled
tion (Fig. 1). By applying the mass balance law,
it comes that the amount of drug inhaled minus
Furthermore, by accommodating a cascade im-
the amount of drug exhaled is equal to the
pactor in the setup (Fig. 1) during a separate ex-
amount of drug deposited in the lungs. The
periment, the mass median aerodynamic diame-
setup shown in Figure 1(2,4,7–9) depicts these
ter (MMAD) can be determined. Particles with
components relative to the initial amount of ac-
MMAD Ͼ 5-m impact the endotracheal tube
tive drug filled in the nebulizer (nebulizer
and the ventilatory circuit during IMV and the
charge). The inhaled fraction is the ratio of the
pharynx during NIV. Particles with MMAD be-
amount of drug captured by the filter A (Fig. 1)
tween 1 and 5 m mainly deposit in the airways
to the nebulizer charge. It reflects the amount of
by sedimentation while particles with MMAD be-
drug available for inhalation by the patient be-
tween 1 and 3 m have the potential to reach the
cause it takes into account the amount of drug
lost into the nebulizer, the ventilator circuit andthe endotracheal tube. But the drug can also be
Devices to generate aerosols during
directly exhaled without being inhaled or ex-
haled from the lungs after inhalation, and thisamount is captured on the filter B (Fig. 1). O’Ri-
In patients receiving mechanical ventilation in-
ordan et al.(4) combined in vitro (Fig. 1) and in
haled bronchodilators can be administered by
vivo experiments in seven mechanically venti-
nebulizer or pressurized metered-dose inhaler
lated patients, computed the exhaled fraction
(MDI) devices. A nebulizer device is character-
and found that: (1) the inhaled fraction averaged
ized by a function curve that relates the cumula-
31%, and (2) the lung deposition averaged 15%
tive output of the drug against time. The nebu-
INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
lizer function curve has an initial slope and a
sition(13) with differences among the spac-
plateau. The time interval to the plateau is the
ers.(14–16) The MDI actuation should be synchro-
time during which the inhaled mass increases.
nized with the inspiratory phase of the ventilator
Once the plateau is reached the amount of in-
to increase the delivery.(17) Performing an end-in-
haled drug no longer increases and, hence, there
spiratory pause after actuation has been recom-
is no advantage to continue nebulization further.
mended.(1) Compared to chlorofluorocarbon, gas
In clinical practice there is a good correlation be-
propellant hydrofluoroalkane protects environ-
tween plateau onset and sputtering. Depending
ment better,(18) and MDIs powered by the latter
on the function curve of the nebulizer, both treat-
are as efficient as those propelled by the former.
ment time and amount of inhaled drug may varybetween devices.(2) The nebulizer fill volume can
Ventilator-related factors of inhaled drugs
also influence inhaled mass: the higher the vol-
deposition during mechanical ventilation
ume fill the greater the inhaled mass for a givennebulizer.(10) The performance of jet or pneumatic
Comprehensive in vitro studies have investi-
nebulizers depends on the powering flow of the
gated the role of ventilator-related factors to the
gas, which is usually between 6–8 L/min (Fig. 2).
lung deposition during mechanical ventilation
Ultrasonic nebulizers can also be used during me-
(Table 1). Ventilatory settings, location of the de-
chanical ventilation.(11) Contrary to pneumatic
vice in the circuit, density, and humidity of the
nebulizers, their performance is independent on
gas powering the device, the endotracheal tube,
the ventilatory settings (Table 1). Devices that uti-
lize a vibrating mesh or plate may be interesting
Among the ventilatory settings, low inspiratory
because they are highly efficient to deliver
flow, high tidal volume, low respiratory frequency,
and long duty cycle applied during the inhalation
In ambulatory spontaneously breathing pa-
have been shown to increase lung deposition with
tients, MDIs require training to ensure coordina-
both nebulizer and MDI. The location of nebulizer
tion for optimal delivery. However, up to 70% of
in the ventilatory circuit influences deposition,(10,19)
these patients fail to use MDIs properly.(3) For
the manifold location being more efficient than Y
ICU patients receiving mechanical ventilation, it
piece placement (Table 1). This is also true using
is caregivers’ responsibility to optimize MDI ad-
MDI with a chamber.(20) During NIV, the optimal
ministration. Of notice, MDI canister has to be
position of the nebulizer is between the leak port
shaken vigorously, and must be connected to an
and the patient connection to maximize the deliv-
inhalation chamber with the drug delivery port
of the canister placed bottom up (Fig. 2). The use
The modern ICU ventilators can directly power
of chamber with a MDI increases the drug depo-
the nebulizer, making the nebulization synchro-
Proper installation of pneumatic nebulizer (left panel) and pressurized metered-dose inhaler (MDI) (right
panel) in the ventilatory circuit. Both devices should be located 20–30 cm upstream from the Y piece. The pneumaticnebulizer should be powered with optimal gas flow. The MDI-canister should be actuated using a chamber. GUERIN ET AL.
TABLE 1. VENTILATOR-RELATED FACTORS OF LUNG DEPOSITION AFTER DRUG INHALATION: IN VITRO STUDIES
patient adaptor, respiratory rate 20/min,
increasing inspiratory pressure anddecreasing expiratory pressure(58)
CPAP, continuous positive airway pressurre; CMV, controlled mechanical ventilation; AC, assisted controlled me-
chanical ventilation; PS, pressure support; VT, tidal volume.
nized with the inspiration and, hence, enhancing
does not mean that the inhaled mass of the drug
its efficiency by as much as four times more than
is increased with helium. The humidity of air has
a continuous administration.(8) The flow diverted
a major impact on lung deposition during me-
from the ventilator to the nebulizer is automati-
chanical ventilation. Lung deposition may be re-
cally compensated to maintain tidal volume and
duced by as much as 40% with wet air compared
minute-ventilation constant. Use of helium–oxy-
to dry air with either nebulizer(7,8,10) or MDI.(24)
gen mixture may be attractive to increase the in-
Taken together, the above data provide the ICU
haled mass by reducing impaction in ventilator
physician with recommendations to optimally
circuit and promoting a more peripheral deposi-
deliver inhaled bronchodilators during mechani-
tion. In vitro, with MDI, albuterol deposition in-
creased by 50% with 80% helium–20% oxygen
Endotracheal tube has long been viewed as a
compared to oxygen feeding the ventilator.(22)
significant barrier to the deposition of inhaled
However, the performance of the nebulizer was
medications.(25) In vitro, the delivery to filter de-
impaired with heliox compared to oxygen at
creased with the reduction of the inner diameter
same flow.(22) Finally, the maximal drug deposi-
of the endotracheal tube.(17) In vivo, however, the
tion was obtained by powering the nebulizer with
endotracheal tube was not a significant barrier to
oxygen and feeding the ventilator with heliox.(22)
the deposition because it was found that only
This situation combines the maximal energy sup-
2.6% and 7% of the nebulizer charge deposited in
ply to the nebulizer and the facilitation of drug
the endotracheal tube during inspiration and ex-
transport to the airways. However, this result
INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
TABLE 2. THE 10 STEPS TO OPTIMIZE AND SECURE THE AEROSOL DELIVERY WITH MDI OR NEBULIZER IN PATIENTS
RECEIVING INVASIVE MECHANICAL VENTILATION IN VOLUME-CONTROLLED MODE
expiratory line before theexhalation valve
flow 30–50 L/min: make sure thatintrinsic PEEP does not rise
c. Allows at least 30 sec between b. Select optimal flow to powerc. two actuations.
a.a. the nebulizer. If unknown, choose 6–8
Adjust minute ventilation if required tokeep VT constant.
d. Set the optimal duration of nebulization.
a. b. Patient–ventilator synchronization
aa. .or nebulizerb. Reset previous ventilatory
Adapted from refs 1, 2, and 10. MDI, metered-dose inhaler; VT, tidal volume, PEEP, positive end-expiratory pressure; SpO2, transcutaneous oxy-
Indications of inhaled bronchodilators in
for using inhaled bronchodilators in the ICU set-
mechanically ventilated ICU patients
ting. The studies supporting this level of recom-mendation are essentially physiologic and short
The medications usually employed for inhala-
term. No controlled study to date in asthma or
tion therapy in France are provided in Table 3.
chronic obstructive pulmonary disease (COPD)
Inhaled bronchodilator therapy has been graded
evaluated the impact of inhaled bronchodilators
as level B, that is, of probable value, in patients
on clinical outcomes as duration of mechanical
receiving mechanical ventilation and exhibiting
ventilation or weaning process. In a single ICU,
bronchospasm or asthma.(26) Wheezing, intrinsic
it has recently been observed that: (1) one-third
PEEP, elevated airway resistance, difficult to
of patients did receive inhaled bronchodilating
wean, ventilator dependence are also indications
agents for unclear reason, (2) mechanical ventila-
ȇ Ǟ ȇ ȇ 10%, 18%, 6% PEEPi 16%, 17%, 16% PEEPi
Expiratory iso-flow 0.1 L/sec with MDI or NEB
g MDI vs. 2.5 mg NEB g MDI vs. 200 g MDI vs. 40–100
For adults. Higher doses, that is, more frequent administrations, may be required in patients experiencing severe acute bronchoa
AO, airway obstruction; MDI, pressurized metered-dose inhaler; NEB, nebulizer; Rrs, total resistance of the respiratory system;
-adrenergic Albuterol-Salbutamol sulfate
pressure of the respiratory system; IP, ipratropium bromide. INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
tion duration was longer in patients who were
Dose. Contrasted dose–response effects on res-
treated with inhaled bronchodilators than in
piratory mechanics have been observed with
those who were not; and (3) related cost was
MDI and nebulizer. Dhand et al.(35) found that
maximal reduction of Raw was obtained after 4
Promising findings have been obtained in pa-
puffs of albuterol administered via an MDI with
tients with the acute respiratory distress syn-
no further reduction up to 16 puffs. Bernasconi et
drome (ARDS) in whom intravenous albuterol
al.(33) found that nebulized fenoterol resulted in
was able to reduce extravascular lung water and
significantly greater reduction of Raw than neb-
plateau pressure compared to placebo.(28) Be-
ulized saline but no dose–effect relationship with
cause nebulization can achieve relevant concen-
fenoterol. Manthous et al.(36) found no dose–re-
trations of albuterol in the edema fluid of patients
sponse relationship with albuterol administered
with ARDS,(29) the efficacy of this route to in-
via an MDI but a 10% decline in resistive pres-
crease the alveolar clearance of lung edema
sure while delivering the same molecule at 2.5, 5,
and 7.5 mg via a nebulizer. In this study(36) themodest reduction of respiratory resistance may
Effects of inhaled bronchodilators in mechanically
be attributed to the case mix because only two
patients were COPD. The lack of effect of MDI inthis work(36) may result from an administration
Physiologic effects. The primary objective of
not optimized because the device was attached
bronchodilator treatment in intubated and me-
directly to the endotracheal tube via an elbow
chanically ventilated COPD patients is to reduce
without any chamber. In this connection, the
pulmonary dynamic hyperinflation and resis-
same group found, in a further study,(37) a sig-
tance of the respiratory system to reduce the work
nificant reduction of respiratory resistance with
of breathing.(30) Respiratory mechanics was es-
the same molecule delivered by an MDI located
sentially assessed from the interrupter technique
during constant-flow inflation.(31) This technique
Increasing the dose of the molecule may also
is very popular in the ICUs because it is easy and
increase the risk for cardiac arrhythmias. Above
quick to perform at the bedside and allows par-
4 puffs of albuterol, any further reduction of res-
titioning of total inspiratory resistance into its air-
piratory resistance was obtained while heart rate
way (Raw) and tissue components. It requires,
significantly increased.(35) In a previous study,
however, fully relaxation of the patient during
the same group did not observe any significant
the maneuvre. A reduction of respiratory system
change in heart rate with 10 puffs of albuterol via
resistance, mostly stemming from a decline in
Raw, and of intrinsic PEEP, has consistently beendocumented after administration of inhaled bron-
Administration. It has been shown in vitro (Table
chodilators in intubated COPD patients by
1) that it was possible to optimize the delivery of
inhaled medication by accommodating the ven-tilator and its adjuncts. Accordingly, recommen-
Duration of effects. The beneficial effects of al-
dations were provided for patients receiving IMV
buterol inhalation on respiratory mechanics
(Table 2). However, Mouloudi et al.(39) demon-
were no longer observed after 240 min in stable
strated that some of these ventilator-related fac-
mechanically ventilated COPD patients, sug-
tors were no longer significant in the real life. The
gesting that this drug may be administered
authors studied the effects on respiratory me-
every 4 h.(32) However, 120 min after fenoterol
chanics of albuterol delivered via an MDI in in-
inhalation the resistance of the respiratory sys-
tubated and mechanically ventilated COPD pa-
tem did not significantly differ from the base-
tients. Although albuterol induced a significant
line.(33) Furthermore, the time course of respi-
reduction of respiratory resistance, the accom-
ratory mechanics after inhaled albuterol was
modation of tidal volume (8 vs. 12 mL/kg)(39) or
highly variable among patients, which pre-
inspiratory flow rate (0.6 vs. 1.2 L/s)(40) or pat-
cludes any fixed standardization of dosage
tern (decelerating versus constant)(41) or end-in-
schedule.(34) This lack of predictability is an ad-
spiratory pause (none or 5 sec)(42) at the time of
ditional argument to thoroughly evaluate the
inhalation did not influence the reduction of res-
piratory resistance and intrinsic PEEP. These re-
GUERIN ET AL.
sults demonstrated that once dosage was ade-
were improved with the combination of PEEP
quate (200–600 g albuterol(39–42)) and adminis-
tration optimized (MDI plus spacer), manipula-tion of the ventilator settings did not produce
Nebulizer or MDI. Both devices were equally ef-
additional measurable effects on respiratory me-
fective to improve respiratory mechanics in most
studies (Table 4). Therefore, other arguments
The application of external PEEP in COPD pa-
than effectiveness should be taken into account
tients under invasive mechanical ventilation has
to prefer one device to the other. MDI are easier
been largely investigated in the last years.(43–50)
to use. Nebulizers are cumbersome and more
As far as the patient is sedated and receives pas-
costly. Whatever the device, the physician has to
sive mechanical ventilation the use of external
be familiar with the one she/he uses routinely
PEEP is not necessary. If it is nevertheless used,
and, of notice, with particle size distribution gen-
its level should be less than 85% of the static in-
erated and optimal powering flow in the case of
trinsic PEEP to avoid any hemodynamics com-
promise.(49) However, there may be a rationalefor using low levels of PEEP in passively venti-
lated COPD patients to reopen small airwaysclosed during the tidal breathing.(51,52) Further-
Although NIV is increasingly used in ICUs,
more, by maintaining small airways patency, ex-
the data regarding the effects of bronchodilators
ternal PEEP may facilitate the distribution and
in this setting are still scanty. NIV may be a
physiological effects of inhaled bronchodilators
method to increase the deposited mass in adults
medication. In vitro studies have shown that in-
with acute bronchospasm(56) or in children with
cystic fibrosis.(57) The mechanisms by which
PEEP.(9,53) The interaction between external
NIV can increase deposited mass are: dry air,
PEEP and inhaled bronchodilator was recently
larger tidal volume than during unassisted
investigated in two studies on COPD patients
spontaneous breathing, improvement of effi-
who received INV, which gave discrepant re-
ciency of the nebulizer,(57) combination with ex-
sults. In 10 COPD patients, Guérin et al.(54) stud-
ternal PEEP,(55) absence of endotracheal tube. In
ied the time course of the effects on respiratory
vitro, significant increase in inhaled mass was
mechanics of nebulized fenoterol either on zero
obtained during NIV by locating the nebulizer
external PEEP (ZEEP) or external PEEP amount-
between the leak port of the single limb circuit
ing to 85% intrinsic PEEP. They found that after
and the patient(58,59) and by using high inspira-
fenoterol administration respiratory mechanics
tory or expiratory pressures.(58,59) In a random-
improved with ZEEP but remained unchanged
ized controlled study in 18 stable COPD pa-
with external PEEP. The authors explained the
tients, Nava et al.(60) found that salbutamol
results by the fact that intrinsic PEEP declined
delivered via an MDI and a chamber during NIV
with fenoterol, and once its level became lower
exhibited a greater bronchodilating effect than
than external PEEP dynamic hyperinflation in-
placebo, but might be less efficient than during
creased as did respiratory resistance. Tzoufi et
al.(55) in 10 COPD patients, measured respiratorymechanics during five conditions: (1) baselineZEEP, (2) 30 min after nebulization of 5 mg al-
CONCLUSIONS
buterol on ZEEP, (3) 8 h after albuterol inhala-tion on ZEEP, (4) 30 min after application of
The administration of bronchodilators in ICU
PEEP equal to intrinsic PEEP, (5) 30 min after
patients receiving mechanical ventilation is pos-
nebulization of 5 mg albuterol on the same level
sible and efficient, using either nebulizer or MDI.
of PEEP as in condition 4. The authors found that
Based on in vitro studies, practical recommenda-
PEEP and albuterol had additive beneficial ef-
tions have been issued to help clinicians in opti-
fects on intrinsic PEEP which went from 7 cm
mization of this therapy. Future studies should
H2O at baseline to 4.8 cm H2O with albuterol
assess the effects of inhaled bronchodilators
alone, to 3.7 cm H2O with external PEEP alone
on patient outcome as duration of mechanical
and to 2 cm H2O with both interventions. Fur-
ventilation/weaning/ICU stay/cost-effectiveness
and determine how to optimize the delivery of
INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
inhaled bronchodilators during NIV in the acute
a corticosteroid with a mechanically-ventilated lung
model. Respir Care. 1998;43:705–712.
15. Bishop MJ, Larson RP, and Buschman DL: Metered
dose inhaler aerosol characteristics are affected by theendotracheal tube actuator/adaptor used. Anesthesi-
REFERENCES
16. Fuller HD, Dolovich MB, Turpie FH, and Newhouse
1. Dhand R, and Tobin MJ: Inhaled bronchodilator ther-
MT: Efficiency of bronchodilator aerosol delivery to
apy in mechanically ventilated patients. Am J Respir
the lungs from the metered dose inhaler in mechani-
cally ventilated patients. A study comparing four dif-
2. O’Riordan TG, Greco MJ, Perry RJ, and Smaldone GC:
ferent actuator devices. Chest. 1994;105:214–218.
Nebulizer function during mechanical ventilation.
17. Crogan SJ, and Bishop MJ: Delivery efficiency of me-
Am Rev Respir Dis. 1992;145:1117–1122.
tered dose aerosols given via endotracheal tubes.
3. Dolovich MB, Ahrens RC, Hess DR, Anderson P,
Anesthesiology. 1989;70:1008–1010.
Dhand R, Rau JL, Smaldone GC, and Guyatt G: De-
18. Taylor J, Kotch A, Rice K, Ghafouri M, Kurland CL,
vice selection and outcomes of aerosol therapy: evi-
Fagan NM, and Witek TJ Jr: Ipratropium bromide hy-
dence-based guidelines. Chest. 2005;127:335–371.
drofluoroalkane inhalation aerosol is safe and effec-
4. O’Riordan TG, Palmer LB, and Smaldone GC: Aerosol
tive in patients with COPD. Chest. 2001;120:
deposition in mechanically ventilated patients. Opti-
mizing nebulizer delivery. Am J Respir Crit Care
19. Hughes JM, and Saez J: Effects of nebulizer mode and
position in a mechanical ventilator circuit on dose ef-
5. Dolovich, MA, MacIntyre NR, Anderson PJ, Camargo
ficiency. Respir Care. 1987;32:1131–1135.
CA Jr, Chew N, Cole CH, Dhand R, Fink JB, Gross
20. Newhouse MT, and Fuller HD: Rose is a rose. Aerosol
NJ, Hess DR, Hickey AJ, Kim CS, Martonen TB, Pier-
therapy in ventilated patients: nebulizers versus me-
son DJ, Rubin BK, and Smaldone GC: Consensus
tered-dose inhalers-A continuing controversy. Am
statement: aerosols and delivery devices. American
Rev Respir Dis. 1993;148:1444–1446.
Association for Respiratory Care. Respir Care.
21. Chatmongkolchart S, Schettino GPP, Dillman C, Kac-
mareck RM, and Hess DR: In vitro evaluation of
6. Demoule A, Girou E, Richard JC, Taille S, and
aerosol bronchodilator delivery during non invasive
Brochard L: Increased use of noninvasive ventilation
positive pressure ventilation: effect of ventilator set-
in French intensive care units. Intensive Care Med.
tings and nebulizer position. Crit Care Med. 2002;
7. Diot P, Morra L, and Smaldone GC: Albuterol deliv-
22. Goode ML, Fink JB, Dhand R, and Tobin MJ: Im-
ery in a model of mechanical ventilation. Comparison
provement in aerosol delivery with helium–oxygen
of metered-dose inhaler and nebulizer efficiency. Am
mixtures during mechanical ventilation. Am J Respir
J Respir Crit Care Med. 1995;152:1391–1394.
8. Miller DD, Amin MM, Palmer LB, Shah AR, and Smal-
23. Hess DR, Acosta FL, Ritz RH, Kacmareck RM, and
done GC: Aerosol delivery and modern mechanical
Camargo CA: The effect of heliox on nebulizer func-
ventilation: in vitro/in vivo evaluation. Am J Respir
tion using a b-agonist bronchodilator. Chest. 1999;115:
Crit Care Med. 2003;168:1205–1209.
9. Vecellio L, Guerin C, Grimbert D, De Monte M, and
24. Fink JB, Dhand R, Duarte AG, Jenne JW, and Tobin
Diot P: In vitro study and semiempirical model for
MJ: Aerosol delivery from a metered-dose inhaler
aerosol delivery control during mechanical ventila-
during mechanical ventilation. An in vitro model. Am
tion. Intensive Care Med. 2005;31:871–876.
J Respir Crit Care Med. 1996;154:382–387.
10. O’Doherty MJ, Thomas SHL, Page CJ, Treacher DF,
25. Dhand R: Special problems in aerosol delivery: artifi-
and Nunan TO: Delivery of ventilator settings and
cial airways. Respir Care. 2000;45:636–645.
nebulizer type, position and volume of fill. Am Rev
26. O’Doherty MJ, and Thomas SHL: Nebulizer therapy
in the intensive care unit. Thorax. 1997;52:S56–S59.
11. Thomas SHL, O’Doherty MJ, Page CJ, Treacher DF,
27. Chang LH, Honiden S, Haithcock JA, Das AM, Short
and Nunan TO: Delivery of ultrasonic nebulized
KA, Nierman DM, and Carson SS: Utilization of bron-
aerosols to a lung model during mechanical ventila-
chodilators in ventilated patients without obstructive
tion. Am Rev Respir Dis. 1993;148:872–877.
airways disease. Respir Care. 2007;52:154–158.
12. Dhand R: Nebulizers that use a vibrating mesh or
28. Perkins GD, McAuley DF, Thickett DR, and Gao F:
plate with multiple apertures to generate aerosol.
The beta-agonist lung injury trial (BALTI): a ran-
domized placebo-controlled clinical trial. Am J Respir
13. Rau JL, Harwood RJ, and Groff JL: Evaluation of a
reservoir device for metered-dose bronchodilator de-
29. Atabai K, Ware LB, Snider ME, Koch P, Daniel B,
livery to intubated patients. Chest. 1992;102:924–930.
Nuckton TJ, and Matthay MA: Aerosolized beta(2)-
14. Rau JL, Dunlevy C, and Hill P: A comparison of in-
adrenergic agonists achieve therapeutic levels in the
line MDI actuators for delivery of a beta agonist and
pulmonary edema fluid of ventilated patients with
GUERIN ET AL.
acute respiratory failure. Intensive Care Med. 2002;
tilated COPD patients: influence of end-inspiratory
pause. Eur Respir J. 1998;12:165–169.
30. Mancebo J, Amaro P, Lorino H, Lemaire F, Harf A,
43. Georgopoulos D, Giannouli E, and Patakas D: Effects
and Brochard L: Effects of albuterol inhalation on the
of extrinsic positive end-expiratory pressure on me-
work of breathing during weaning from mechanical
chanically ventilated patients with chronic obstruc-
ventilation. Am Rev Respir Dis. 1991;144:95–100.
tive pulmonary disease and dynamic hyperinflation.
31. D’Angelo E, Calderini E, Torri G, Robatto FM, Bono
Intensive Care Med. 1993;19:197–203.
D, and Milic-Emili J: Respiratory mechanics in anes-
44. Guerin C, Fournier G, and Milic-Emili J. Effects of
thetized paralyzed humans: effects of flow, volume,
PEEP on inspiratory resistance in mechanically ven-
and time. J Appl Physiol. 1989;67:2556–2564.
tilated COPD patients. Eur Respir J 2001;18:491–498.
32. Duarte AG, Momii K, and Bidani A: Bronchodilator
45. Guerin C, Milic-Emili J, and Fournier G: Effect
therapy with metered-dose inhaler and spacer versus
of PEEP on work of breathing in mechanically venti-
nebulizer in mechanically ventilated patients: com-
lated COPD patients. Intensive Care Med. 2000;26:
parison of magnitude and duration of response.
46. Kondili E, Alexopoulou C, Prinianakis G, Xirouchaki
33. Bernasconi M, Brandolese R, Poggi R, Manzin E, and
N, and Georgopoulos D: Pattern of lung emptying
Rossi A: Dose–response effects and time course of ef-
and expiratory resistance in mechanically ventilated
fects of inhaled fenoterol on respiratory mechanics
patients with chronic obstructive pulmonary disease.
and arterial oxygen tension in mechanically venti-
Intensive Care Med. 2004;30:1311–1318.
lated patients with chronic airflow obstruction. In-
47. Musch G, Foti G, Cereda M, Pelosi P, Poppi D, and
tensive Care Med. 1990;16:108–114.
Pesenti A: Lung and chest wall mechanics in normal
34. Mouloudi E, Maliotakis C, Kondili E, Kafetzakis A,
anaesthetized subjects and in patients with COPD at
and Georgopoulos D: Duration of salbutamol-in-
different PEEP levels. Eur Respir J 1997;10:2545–2552.
duced bronchodilation delivered by metered-dose in-
48. Petrof BJ, Legare M, Goldberg P, Milic-Emili J, and
haler in mechanically ventilated COPD patients.
Gottfried SB: Continuous positive airway pressure re-
Monaldi Arch Chest Dis. 2001;56:189–194.
duces work of breathing and dyspnea during wean-
35. Dhand R, Duarte AG, Jubran A, Jenne JW, Fink JB,
ing from mechanical ventilation in severe chronic ob-
Fahey PJ, and Tobin MJ: Dose–response to bron-
structive pulmonary disease. Am Rev Respir Dis.
chodilator delivered by metered-dose inhaler in ven-
tilator-supported patients. Am J Respir Crit Care Med.
49. Ranieri VM, Giuliani R, Cinnella G, Pesce C, Brienza
N, Ippolito EL, Pomo V, Fiore T, Gottfried SB, and
36. Manthous CA, Hall JB, Schmidt GA, and Wood LDH:
Brienza A: Physiologic effects of positive end-expira-
Metered-dose inhaler versus nebulized albuterol in
tory pressure in patients with chronic obstructive pul-
mechanically ventilated patients. Am Rev Respir Dis.
monary disease during acute ventilatory failure and
controlled mechanical ventilation. Am Rev Respir
37. Manthous CA, Chatila W, Schmidt GA, and Hall JB:
Treatment of bronchospasm by metered-dose inhaler
50. van den Berg B, Stam H, and Bogaard JM: Effects of
albuterol in mechanically ventilated patients. Chest.
PEEP on respiratory mechanics in patients with
COPD on mechanical ventilation. Eur Respir J. 1991;
38. Dhand R, Jubran A, and Tobin MJ: Bronchodilator de-
livery by metered-dose inhaler in ventilator-sup-
51. Guerin C, LeMasson S, de Varax R, Milic-Emili J, and
ported patients. Am J Respir Crit Care Med. 1995;
Fournier G: Small airway closure and positive end-
expiratory pressure in mechanically ventilated pa-
39. Mouloudi E, Katsanoulas K, Anastasaki M, Hoing S,
tients with chronic obstructive pulmonary disease.
and Georgopoulos D: Bronchodilator delivery by me-
Am J Respir Crit Care Med. 1997;155:1949–1956.
tered-dose inhaler in mechanically ventilated COPD
52. Milic-Emili J: Does mechanical injury of the periph-
patients: influence of tidal volume. Intensive Care
eral airways play a role in the genesis of COPD in
40. Mouloudi E, Prinianakis G, Kondili E, and Geor-
53. Parkes SN, and Bersten AD: Aerosol kinetics and
gopoulos D: Effect of inspiratory flow rate on beta2-
bronchodilator efficacy during continuous positive
agonist induced bronchodilation in mechanically
airway pressure delivered by face mask. Thorax.
ventilated COPD patients. Intensive Care Med.
54. Guerin C, Durand PG, Pereira C, Richard JC, Poupelin
41. Mouloudi E, Prinianakis G, Kondili E, and Geor-
JC, Lemasson S, Badet M, Philit F, Vecellio L, and
gopoulos D: Bronchodilator delivery by metered-dose
Chantrel G: Effects of inhaled fenoterol and positive
inhaler in mechanically ventilated COPD patients: in-
end-expiratory pressure on the respiratory mechan-
fluence of flow pattern. Eur Respir J. 2000;16:263–268.
ics of patients with chronic obstructive pulmonary
42. Mouloudi E, Katsanoulas K, Anastasaki M, Aski-
disease. Can Respir J. 2005;12:329–335.
topoulou E, and Georgopoulos D: Bronchodilator de-
55. Tzoufi M, Mentzelopoulos SD, Roussos C, and Ar-
livery by metered-dose inhaler in mechanically ven-
maganidis A: The effects of nebulized salbutamol, ex-
INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
ternal positive end-expiratory pressure, and their
ery in intubated, mechanically ventilated patients.
combination on respiratory mechanics, hemodynam-
ics, and gas exchange in mechanically ventilated
63. Fernandez A, Lazaro A, Garcia A, Aragon C, and
chronic obstructive pulmonary disease patients.
Cerda E: Bronchodilators in patients with chronic ob-
structive pulmonary disease on mechanical ventila-
56. Pollack CVJ, Fleisch KB, and Dowsey K: Treatment of
tion. Utilization of metered-dose inhalers. Am Rev
acute bronchospasm with beta-adrenergic agonist
aerosols delivered by a nasal bilevel positive airway
64. Fernandez A, Munoz J, de la Calle B, Alia I, Ezpeleta
pressure circuit. Ann Emerg Med. 1995;26:552–557.
A, de la Cal MA, and Reyes A: Comparison of one
57. Fauroux B, Itti E, Pigeot J, Isabey D, Meignan M, Ferry
versus two bronchodilators in ventilated COPD pa-
G, Lofaso F, Willemot JM, Clement A, and Harf A:
tients. Intensive Care Med. 1994;20:199–202.
Optimization of aerosol deposition by pressure sup-
65. Guerin C, Chevre A, Dessirier P, Poncet T, Becquemin
port in children with cystic fibrosis: an experimental
MH, Dequin PF, Le Guellec C, Jacques D, and
and clinical study. Am J Respir Crit Care Med. 2000;
Fournier G: Inhaled fenoterol-ipratropium bromide in
mechanically ventilated patients with chronic ob-
58. Chatmongkolchart S, Schettino GP, Dillman C, Kac-
structive pulmonary disease. Am J Respir Crit Care
marek RM, and Hess DR: In vitro evaluation of aerosol
bronchodilator delivery during noninvasive positivepressure ventilation: effect of ventilator settings and neb-ulizer position. Crit Care Med. 2002;30:2515–2519.
59. Branconnier MP, and Hess DR: Albuterol delivery
during noninvasive ventilation. Respir Care. 2005;50:1649–1653.
60. Nava S, Karakurt S, Rampulla C, Braschi A, and Fan-
fulla F: Salbutamol delivery during non-invasive me-
chanical ventilation in patients with chronic obstruc-tive pulmonary disease: a randomized, controlled
study. Intensive Care Med. 2001;27:1627–1635.
61. Hess DR, Dillmna C, and Kacmareck RM: In vitro
evaluation of aerosol bronchodilator delivery during
mechanical ventilation: pressure-control vs. volume
control ventilation. Intensive Care Med. 2003;29:1145–1150.
62. Gay PC, Patel HG, Nelson SB, Gilles B, and Hubmayr
RD: Metered dose inhalers for bronchodilator deliv-
CHAPTER 6 Test Yourself, p. 228 1. What is classical conditioning? How was it discovered? ANSWER CLUES: A. Classical conditioning is sometimes called Pavlovian conditioning because it was discovered by Ivan Pavlov. a. Pavlov studied salivation in dogs. He collected the saliva in tubes connected to the dogs’ salivary glands. Pavlov noticed that his dogs were salivating simply on se
Spiagge, immersioni e tartarughe nel nord di Cipro Il nord di Cipro offre al Turista spiagge con acque limpide e cristalline come difficilmente si possono trovare nel mediterraneo. Le sue coste sono variegate: roccia e sabbia si mescolano in un connubio unico. Chilometri e chilometri di spiagge sabbiose nascoste dietro alle dune. Sulla costa est tra Famagosta e Bogaz, troverete un ar
 GUERIN ET AL.
GUERIN ET AL.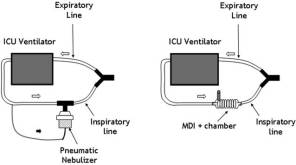 INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION
INHALED BRONCHODILATORS DURING MECHANICAL VENTILATION