Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Viagra product information
PRODUCT INFORMATION VIAGRA TABLETS sildenafil (as citrate) NAME OF THE MEDICINE
Sildenafil citrate is an orally active selective inhibitor of cGMP - specific PDE5 (phosphodiesterase type 5) which is the predominant PDE isoenzyme in human corpora cavernosa.
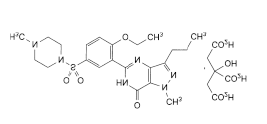
Sildenafil citrate is 5-[2-Ethoxy-5-[(4-methylpiperazin-1-yl)sulfonyl]phenyl]-1-methyl-3-
propyl-1,6-dihydro-7H-pyrazolo[4,3-d]pyrimidin-7-one dihydrogen 2-hydroxypropane-1,2,3-
The empirical formula for sildenafil citrate is C28H38N6O11S with a molecular weight of 666.7
Sildenafil citrate has the following structural formula:
DESCRIPTION
Sildenafil citrate is a white to almost white, crystalline powder. Its aqueous solubility is equivalent to 2.6 mg sildenafil per mL at 25°C.
In addition to sildenafil citrate, each VIAGRA tablet contains the following inactive ingredients: microcrystalline cellulose, calcium hydrogen phosphate anhydrous, croscarmellose sodium, magnesium stearate, hypromellose, titanium dioxide, lactose, glycerol triacetate, indigo carmine aluminium lake. VIAGRA tablets may contain PF0102 (PI3329).
PHARMACOLOGY Pharmacodynamics
VIAGRA is an oral therapy for erectile dysfunction which restores impaired erectile function by increasing blood flow to the penis, resulting in a natural response to sexual stimulation.
The physiological mechanism responsible for erection of the penis involves the release of nitric oxide (NO) in the corpus cavernosum during sexual stimulation. Nitric oxide then activates the enzyme, guanylate cyclase, which results in increased levels of cyclic guanosine monophosphate (cGMP), producing smooth muscle relaxation in the corpus cavernosum and allowing inflow of blood.
Sildenafil is a potent and selective inhibitor of cGMP specific phosphodiesterase type 5 (PDE5) which is responsible for degradation of cGMP in the corpus cavernosum. Sildenafil has a peripheral site of action on erections. Sildenafil has no direct relaxant effect on isolated human corpus cavernosum but potently enhances the relaxant effect of NO on this tissue. When the NO/cGMP pathway is activated, as occurs with sexual stimulation, inhibition of PDE5 by sildenafil results in increased corpus cavernosum levels of cGMP. Therefore, sexual stimulation is required in order for VIAGRA to produce its beneficial pharmacological effects.
Single oral doses of VIAGRA up to 100 mg in healthy volunteers produced no clinically relevant effects on ECG. The mean maximum decreases in supine systolic blood pressure following 100 mg oral dosing was 8.4 mmHg. The corresponding change in supine diastolic blood pressure was 5.5 mmHg. These decreases in blood pressure are consistent with the vasodilatory effects of sildenafil, probably due to increased cGMP levels in vascular smooth muscle.
Sildenafil has no effect on visual acuity or contrast sensitivity. Mild and transient differences in colour discrimination (blue/green) were detected in some subjects using Farnsworth-Munsell 100 hue test at 1 hour following a 100 mg dose, with no effects evident after 2 hours post-dose. The postulated mechanism for this change in colour discrimination is related to inhibition of PDE6, which is involved in the phototransduction cascade of the retina. In vitro studies show that sildenafil is 10-fold less potent against PDE6 than PDE5.
Human platelets contain PDE5 enzyme system. Sildenafil, in limited studies, did not affect platelet function in vivo. In in vitro studies sildenafil was shown to potentiate the antiaggregatory effect of the nitric oxide donor, sodium nitroprusside.
Studies in vitro have shown that sildenafil has between 10 and 10,000-fold greater selectivity for PDE5 than for other phosphodiesterase isoforms (PDEs 1, 2, 3, 4, 6, 7 to 11). In particular, sildenafil has greater than 4,000-fold selectivity for PDE5 over PDE3, the cAMP-specific phosphodiesterase isoform involved in the control of cardiac contractility.
Pharmacokinetics Absorption
Sildenafil is rapidly absorbed after oral administration. Maximum observed plasma concentrations are reached within 30 to 120 minutes (median 60 minutes) of oral dosing in
the fasted state. The mean absolute oral bioavailability is 41% (range 25-63%). The oral pharmacokinetics of sildenafil are proportional over the recommended dose range (25 mg-100 mg).
When VIAGRA film-coated tablets are taken with a high fat meal, the rate of absorption of sildenafil is reduced with a mean delay in Tmax of 60 minutes and a mean reduction in Cmax of 29%. Patients may need to individualise their dosing relative to their food intake based on their own experienced clinical response.
Distribution
The mean steady state volume of distribution (Vss) for sildenafil is 105 L, indicating distribution into the tissues. Sildenafil and its major circulating N-desmethyl metabolite are both approximately 96% bound to plasma proteins. Protein binding is independent of total drug concentrations.
In sixteen healthy volunteers receiving sildenafil (100 mg single dose), the mean semen concentrations of sildenafil 1.5 and 4 hours post-dose were 18% and 17% respectively of the plasma concentration at the same time point. The amount in the ejaculate at 90 minutes after dosing was less than 0.0002% of the administered dose.
Metabolism
Sildenafil is cleared predominantly by the CYP3A4 (major route) and CYP2C9 (minor route) hepatic microsomal isoenzymes. The major circulating metabolite results from N-demethylation of sildenafil. This metabolite has a PDE selectivity profile similar to sildenafil and an in-vitro potency for PDE5 approximately 50% of the parent drug. Plasma concentrations of this metabolite are approximately 40% of those seen for sildenafil. The N-desmethyl metabolite is further metabolised with a terminal half-life of approximately 4 hours.
Elimination
The total body clearance of sildenafil is 41 L/h with a resultant terminal phase half-life of 3-5 hours. After either oral or intravenous administration, sildenafil is excreted as metabolites predominantly in the faeces (approximately 80% of administered oral dose) to a lesser extent in the urine (approximately 13% of administered oral dose).
Pharmacokinetics in Special Patient Groups Elderly
Healthy elderly volunteers (65 years or over) had a reduced clearance of sildenafil, with free plasma concentrations approximately 40% greater than those seen in younger volunteers (18-45 years). However, analysis of the safety database showed that age had no effect on the incidence of adverse events.
Renal Insufficiency
In volunteers with mild (Clcr = 50-80 mL/min) and moderate (Clcr = 30-49 mL/min) renal impairment, the pharmacokinetics of a single oral dose of sildenafil (50 mg) were not altered. In volunteers with severe (Clcr = <30 mL/min) renal impairment, sildenafil clearance was
reduced, resulting in increases in AUC (100%) and Cmax (88%) compared to age-matched volunteers with no renal impairment.
Hepatic Insufficiency
In volunteers with hepatic cirrhosis (Child-Pugh A and B), sildenafil clearance was reduced, resulting in increases in AUC (85%) and Cmax (47%) compared to age-matched volunteers with no hepatic impairment. The pharmacokinetics of sildenafil in patients with severe hepatic impairment have not been studied.
CLINICAL TRIALS
The efficacy and safety of VIAGRA was evaluated in 21 randomised, double-blind placebo controlled trials up to 6 months duration. VIAGRA was administered to more than 3,000 patients aged 19-87, with erectile dysfunction of various aetiologies (organic, psychogenic, mixed). The efficacy was evaluated by global assessment questions, diary of erections, the International Index of Erectile Function (IIEF, a validated sexual function questionnaire) and a partner questionnaire.
VIAGRA efficacy, determined as the ability to achieve and maintain an erection sufficient for sexual intercourse, was demonstrated in all 21 studies and was maintained in long term extension studies (one year). In fixed dose studies the proportions of patients reporting that treatment improved their erections were 62% (25 mg), 74% (50 mg), 82% (100 mg) compared to 25% on placebo. In addition to improvements in erectile function, analysis of IIEF showed that VIAGRA treatment also improved the domains of orgasm, satisfaction with intercourse and overall satisfaction.
Across all trials, the proportion of patients reporting improvement on VIAGRA were 59% of diabetic patients, 43% of radical prostatectomy patients and 83% of patients with spinal cord injury (versus 16%, 15% and 12% on placebo respectively).
INDICATIONS
VIAGRA is indicated for the treatment of erectile dysfunction in adult males.
VIAGRA is not indicated for use by women.
CONTRAINDICATIONS
Use of VIAGRA is contraindicated in patients with known hypersensitivity to any component of the tablet.
Nitrates and VIAGRA must not be used concomitantly. VIAGRA was shown to potentiate the hypotensive effects of both acute and chronic nitrate administration and therefore, its co-administration with nitric oxide donors, organic nitrates or organic nitrites in any form, either regularly or intermittently is contraindicated. Drugs which must not be used concomitantly include glyceryl trinitrate (injection, tablets, sprays or patches), isosorbide salts, sodium nitroprusside, amyl nitrite, nicorandil or organic nitrates in any form.
VIAGRA is contraindicated in men for whom sexual intercourse is inadvisable due to cardiovascular risk factors (e.g., patients with severe cardiovascular disease such as established cardiac failure and unstable angina pectoris) (see PRECAUTIONS). The possibility of undiagnosed cardiovascular disorders in men with erectile dysfunction should be considered before prescribing VIAGRA.
VIAGRA is not recommended in patients with male erectile dysfunction with a previous episode of non-arteritic anterior ischaemic optic neuropathy (NAION) (see PRECAUTIONS, ADVERSE EFFECTS - Post Marketing Experience, Other events).
The safety of sildenafil has not been studied in the following sub-groups of patients and its use is therefore contraindicated until further information is available: severe hepatic impairment, hypotension (blood pressure <90/50 mmHg), hypertension (blood pressure >170/110), recent history of stroke or myocardial infarction and known hereditary degenerative retinal disorders such as retinitis pigmentosa (a minority of these patients have genetic disorders of retinal phosphodiesterases).
PRECAUTIONS A thorough medical history and physical examination should be undertaken to diagnose erectile dysfunction, determine potential underlying causes, and identify appropriate treatment. Prior to initiating any treatment for erectile dysfunction, physicians should consider the cardiovascular status of their patients, including those with recent onset angina, since there is a degree of cardiovascular risk associated with sexual intercourse. VIAGRA has vasodilator properties, resulting in mild and transient decreases in blood pressure and, as such, potentiates the hypotensive effect of nitrates (see CONTRAINDICATIONS).
Physicians should advise patients to stop use of all PDE5 inhibitors, including VIAGRA, and seek immediate medical attention in the event of a sudden loss of vision in one or both eyes. Such an event may be a sign of non-arteritic anterior ischaemic optic neuropathy (NAION), a cause of decreased vision including permanent loss of vision, that has been reported rarely post-marketing in temporal association with the use of all PDE-5 inhibitors. An observational study evaluating whether recent use of PDE5 inhibitors, as a class, was associated with acute onset of NAION suggests an increase in the risk of NAION with PDE5 inhibitor use. In case of sudden visual loss, patients should be advised to stop taking sildenafil and consult a physician immediately.
Individuals who have already experienced NAION are at increased risk of NAION recurrence. PDE 5 inhibitors, including VIAGRA, are not recommended in patients with male erectile dysfunction with a previous episode of NAION (see CONTRAINDICATIONS and ADVERSE EFFECTS, Post Marketing Experience, Other Events).
In clinical trials, sildenafil has been shown to have systemic vasodilatory properties that result in transient decreases in blood pressure (see CLINICAL TRIALS). This is of little or no
consequence in most patients. However, prior to prescribing sildenafil, physicians should carefully consider whether their patients with certain underlying conditions could be adversely affected by such vasodilatory effects, especially in combination with sexual activity. Patients with increased susceptibility to vasodilators include those with left ventricular outflow obstruction (e.g., aortic stenosis, hypertrophic obstructive cardiomyopathy), or those with the rare syndrome of multiple system atrophy manifesting as severely impaired autonomic control of blood pressure.
Agents for the treatment of erectile dysfunction should be used with caution in patients with anatomical deformation of the penis (such as angulation, cavernosal fibrosis or Peyronie’s disease), or in patients who have conditions which may predispose them to priapism (such as sickle cell anaemia, multiple myeloma or leukemia).
The safety and efficacy of combinations of VIAGRA with other treatments for erectile dysfunction have not been studied. Therefore the use of such combinations is not recommended.
Caution is advised when sildenafil is administered to patients taking an alpha-blocker, as the co-administration may lead to symptomatic hypotension in a few susceptible individuals (see INTERACTIONS WITH OTHER MEDICINES). In order to minimise the potential for developing postural hypotension, patients should be haemodynamically stable on alpha-blocker therapy prior to initiating sildenafil treatment. Initiation of sildenafil at lower doses should be considered (see DOSAGE AND ADMINISTRATION). In addition, physicians should advise patients what to do in the event of postural hypotensive symptoms.
VIAGRA had no effect on bleeding time, including during co-administration with aspirin. In vitro studies with human platelets indicate that sildenafil potentiates the antiaggregatory effect of sodium nitroprusside (a nitric oxide donor). There is no safety information on the administration of VIAGRA to patients with bleeding disorders or active peptic ulceration. Therefore, VIAGRA should be administered with caution to these patients.
There are limited safety data in patients with diabetic retinopathy. The safety of VIAGRA in patients with untreated diabetic retinopathy has not been studied and therefore VIAGRA should be administered to these patients only after careful benefit-risk assessment.
Sudden decrease or loss of hearing, which may be accompanied by tinnitus and dizziness, has been reported in a small number of post marketing and clinical trials cases with the use of all PDE5 inhibitors, including sildenafil. Most of these patients had risk factors for sudden decrease or loss of hearing. No causal relationship has been made between the use of PDE5 inhibitors and sudden decrease or loss of hearing. In case of sudden decrease or loss of hearing patients should be advised to stop taking sildenafil and consult a physician promptly.
The incidence of adverse events may be greater in those patients who require the maximum recommended dose of 100 mg (e.g., some diabetic and spinal cord injury patients).
Patients with cardiovascular disease who have not engaged in sexual intercourse for a number of years should have their cardiovascular status carefully assessed prior to initiating treatment with VIAGRA.
Prolonged erections greater than four hours in duration and priapism (painful erections greater than 6 hours) have been reported infrequently since market approval of VIAGRA. In the
event of an erection that persists longer than 4 hours, the patient should seek immediate medical assistance. If priapism is not treated immediately, penile tissue damage and permanent loss of potency could result.
Effects on Fertility
There was no impairment of fertility in rats given sildenafil for 36 days to females and 102 days to males at a dose producing an AUC value of more than 25 times the human male AUC.
There is no information on the effects of sildenafil on semen production, sperm motility/morphology in patients suffering from erectile dysfunction. There was no effect on sperm motility or morphology after single 100 mg oral doses of VIAGRA in healthy volunteers.
Use in Pregnancy Australia Pregnancy Category B1. VIAGRA is not indicated for use by women.
No evidence of teratogenicity, embryotoxicity or fetotoxicity was observed in rats and rabbits which received up to 200 mg/kg/day during organogenesis. The dose results in total systemic drug exposure (AUC) for unbound sildenafil and its major metabolite of greater than 60 times the exposure observed in human males given the maximum recommended human dose (MRHD) of 100 mg. In the rat pre- and post-natal development study, the no observed adverse effect dose was 30 mg/kg/day given for 36 days. In non-pregnant rat the AUC at this dose was about 20 times human AUC. There are no adequate and well controlled studies of sildenafil in pregnant women.
Use in Lactation
VIAGRA is not indicated for use in women. No information is available on its secretion into breast milk.
Genotoxicity
Sildenafil was negative in in vitro bacterial and Chinese hamster ovary cell assays to detect mutagenicity, and in vitro human lymphocytes and in vivo mouse micronucleus assays to detect clastogenicity.
Carcinogenicity
Sildenafil was not carcinogenic when administered to rats for 24 months at a dose resulting in total systemic drug exposure (AUC) for unbound sildenafil and its major metabolite of 35- and 39-times, for male and female rats, respectively, the exposures observed in human males given the maximum recommended human dose (MRHD) of 100 mg. Sildenafil was not carcinogenic when administered to mice for 18-21 months at dosages up to the maximum tolerated dose of 10 mg/kg/day, but resulting in total systemic drug exposure for unbound
sildenafil and its major metabolite of less than the exposures observed in human males given the MRHD.
Effects on Ability to Drive and Use Machines
As transient visual disturbances and dizziness have been reported in some patients taking VIAGRA, particularly at the 100 mg dose, patients should be aware of how they react to VIAGRA before driving or operating machinery, and the doctor should advise accordingly.
INTERACTIONS WITH OTHER MEDICINES Effects of Other Medicines on VIAGRA
Sildenafil metabolism is principally mediated by the cytochrome P450 (CYP) isoforms 3A4 (major route) and 2C9 (minor route). Therefore, inhibitors of these isoenzymes may reduce sildenafil clearance and inducers of these isoenzymes may increase sildenafil clearance.
Population pharmacokinetics analysis of clinical trial data indicated a reduction in sildenafil clearance when co-administered with CYP3A4 inhibitors (such as ketoconazole, erythromycin, cimetidine). However, there was no increased incidence of adverse events in these patients.
Cimetidine (800 mg), a non-specific CYP3A4 inhibitor, caused a 56% increase in plasma sildenafil concentrations when co-administered with VIAGRA (50 mg) to healthy volunteers.
When a single 100 mg dose of sildenafil was administered with erythromycin, a specific CYP3A4 inhibitor, at steady state (500 mg twice daily for 5 days), there was a 182% increase in sildenafil systemic exposure (AUC).
Co-administration of the HIV protease inhibitor saquinavir, also a CYP3A4 inhibitor, at steady state (1200 mg three times daily) with VIAGRA (100 mg single dose) resulted in a 140% increase in sildenafil Cmax and a 210% increase in sildenafil AUC (see DOSAGE AND ADMINISTRATION). Stronger CYP3A4 inhibitors such as ketoconazole and itraconazole would be expected to have still greater effects.
Co-administration with the HIV protease inhibitor ritonavir, which is a highly potent P450 inhibitor, at steady state (500 mg twice daily) with sildenafil (100 mg single dose) resulted in a 300% (4-fold) increase in sildenafil Cmax and a 1000% (11-fold) increase in sildenafil plasma AUC. At 24 hours the plasma levels of sildenafil were still approximately 200 ng/mL, compared to approximately 5 ng/mL when sildenafil was dosed alone. This is consistent with ritonavir’s marked effects on a broad range of P450 substrates (see DOSAGE AND ADMINISTRATION).
Since systemic exposure to sildenafil increases on co-administration with inhibitors of CYP3A4 the VIAGRA dose may have to be reduced depending on tolerability.
Single doses of antacid (magnesium hydroxide/aluminium hydroxide) did not affect the bioavailability of VIAGRA.
There is no information on the interaction between sildenafil and cyclosporin.
It can be expected that concomitant administration of CYP3A4 inducers, such as rifampicin, will decrease plasma levels of sildenafil.
Population pharmacokinetics analysis showed no effect of concomitant medication on sildenafil pharmacokinetics when grouped as CYP2C9 inhibitors, CYP2D6 inhibitors (such as selective serotonin reuptake inhibitors, tricyclic antidepressants), thiazide and related diuretics, loop and potassium sparing diuretics, ACE inhibitors, calcium channel blockers, beta-adrenoreceptor antagonists or inducers of CYP450 metabolism (such as barbiturates). Effects of VIAGRA on Other Medicines
Sildenafil is a weak inhibitor of the cytochrome P450 isoforms 1A2, 2C9, 2C19, 2D6, 2E1 and 3A4 (IC50 >150 mM). Given sildenafil peak plasma concentrations of approximately 1
mM after recommended doses, it is unlikely that sildenafil will alter the clearance of substrates of these isoenzymes.
There are no data on the interaction of sildenafil and non-specific phosphodiesterase inhibitors such as theophylline or dipyridamole.
In three specific drug-drug interaction studies, the alpha-blocker doxazosin (4 mg and 8 mg) and sildenafil (25 mg, 50 mg, or 100 mg) were administered simultaneously to patients with benign prostatic hyperplasia (BPH) stabilised on doxazosin therapy. In these study populations, mean additional reductions of supine blood pressure of 7/7 mmHg, 9/5 mmHg, and 8/4 mmHg, and mean additional reductions of standing blood pressure of 6/6 mmHg, 11/4 mmHg, and 4/5 mmHg, respectively, were observed. When sildenafil and doxazosin were administered simultaneously to patients stabilized on doxazosin therapy, there were infrequent reports of patients who experienced symptomatic postural hypotension. These reports included dizziness and lightheadedness, but not syncope. Concomitant administration of sildenafil to patients taking alpha-blocker therapy may lead to symptomatic hypotension in a few susceptible individuals
No significant interactions were shown when sildenafil 50 mg was co-administered with tolbutamide (250 mg) or warfarin (40 mg), both of which are metabolised by CYP2C9.
VIAGRA (50 mg) did not potentiate the increase in bleeding time caused by aspirin (150 mg).
Sildenafil causes a small reduction in supine and tilted diastolic blood pressure (3.5 and 6.1 mmHg respectively) in healthy subjects who had a blood alcohol level of 80 mg/dL.
No interaction was seen when VIAGRA (100 mg) was co-administered with amlodipine in hypertensive patients. The mean additive reduction on supine blood pressure (systolic, 8 mmHg; diastolic, 7 mmHg) was of a similar magnitude to that seen when sildenafil was administered alone to healthy volunteers (see PHARMACOLOGY, Pharmacodynamics).
Analysis of the safety data base showed no difference in the side effect profile in patients taking VIAGRA with and without anti-hypertensive medication.
Sildenafil was shown to potentiate the hypotensive effect of acute and chronic nitrate administration. Therefore, use of nitric oxide donors, organic nitrates, or organic nitrites in
any form either regularly or intermittently with sildenafil is contraindicated (see CONTRAINDICATIONS).
ADVERSE EFFECTS Clinical Trial Data
VIAGRA was administered to over 3700 patients (aged 19-87) during clinical trials worldwide. Over 550 patients were treated for longer than one year.
Treatment with VIAGRA was well tolerated. In placebo controlled clinical studies, the discontinuation rate due to adverse events was low and similar to placebo. The adverse events were generally transient and mild to moderate in nature.
Across trials of all designs, the profile of adverse events reported by patients receiving VIAGRA was similar. In fixed dose studies, the incidence of adverse events increased with dose. The nature of the adverse events in flexible dose studies, which more closely reflect the recommended dosage regimen, was similar to that for fixed dose studies.
When VIAGRA was taken as recommended (on an as needed basis in flexible dose placebo controlled clinical trials) the following adverse events were reported:
Table 1: Adverse events reported by ³2% of patients treated with VIAGRA or placebo in PRN flexible dose phase II/III studies
Adverse event
+ Abnormal Vision: Mild and transient predominantly colour tinge to vision, but also increased perception to light or blurred vision. In these studies, only one patient discontinued due to abnormal vision. This effect was more common at doses of 100 mg or more.
Other adverse reactions occurred at a rate of >2%, but equally commonly on placebo: respiratory tract infection, back pain, flu syndrome and arthralgia.
In fixed dose studies, dyspepsia (17%) and abnormal vision (11%) were more common at 100 mg than at lower doses.
At doses above the recommended dose range, adverse events were similar to those detailed above but generally were reported more frequently.
No cases of priapism were reported during controlled clinical trials.
The following events occurred in <2% of patients in controlled clinical trials; a causal relationship to VIAGRA is uncertain. Reported events include those with a plausible relation to drug use; omitted are minor events and reports too imprecise to be meaningful:
Body as a whole: infection, face oedema, photosensitivity reaction, shock, asthenia, pain, chills, accidental fall, abdominal pain, allergic reaction, chest pain, accidental injury.
Cardiovascular: angina pectoris, AV block, migraine, syncope, tachycardia, palpitation, hypotension, postural hypotension, myocardial ischaemia, cerebral thrombosis, cardiac arrest, heart failure, abnormal electrocardiogram, cardiomyopathy, vasodilation.
Digestive: nausea, vomiting, glossitis, colitis, dysphagia, gastritis, gastroenteritis, oesophagitis, stomatitis, dry mouth, liver function tests abnormal, rectal haemorrhage, gingivitis.
Haemic and Lymphatic: anaemia and leukopenia.
Metabolic and Nutritional: thirst, oedema, gout, unstable diabetes, hyperglycaemia, peripheral oedema, hyperuricemia, hypoglycaemic reaction, hypernatremia.
Musculoskeletal: arthritis, arthrosis, myalgia, tendon rupture, tenosynovitis, bone pain, myasthenia, synovitis.
Nervous: ataxia, hypertonia, neuralgia, neuropathy, paraesthesia, tremor, vertigo, depression, insomnia, somnolence, abnormal dreams, reflexes decreased, hypaesthesia.
Respiratory: rhinitis, respiratory disorder, asthma, dyspnoea, laryngitis, pharyngitis, sinusitis, bronchitis, sputum increased, cough increased.
Skin and appendages: urticaria, herpes simplex, pruritus, sweating, skin ulcer, contact dermatitis, exfoliative dermatitis.
Special senses: mydriasis, conjunctivitis, photophobia, tinnitus, eye pain, sudden decrease or loss of hearing, ear pain, eye haemorrhage, cataract, dry eyes.
Urogenital: prostatic disorder, cystitis, nocturia, urinary frequency, breast enlargement, urinary incontinence, abnormal ejaculation, genital oedema and anorgasmia.
Post Marketing Experience
Cardiovascular: serious cardiovascular events, including myocardial infarction, sudden cardiac death, ventricular arrhythmia, cerebrovascular haemorrhage, transient ischaemic attack and hypertension, have been reported post marketing in temporal association with the use of VIAGRA. Most, but not all, of these patients had pre-existing cardiovascular risk factors. Many of these events were reported to occur during or shortly after sexual activity, and a few were reported to occur shortly after the use of VIAGRA without sexual activity. Others were reported to have occurred hours to days after the use of VIAGRA and sexual
activity. It is not possible to determine whether these events are related directly to VIAGRA, to sexual activity, to the patient’s underlying cardiovascular disease, to a combination of these factors, or to other factors. Tachycardia, hypotension, syncope, and epistaxis have also been reported post-marketing. Rare spontaneous reports have been received of hypotensive events after the use of sildenafil in combination with alpha blockers.
Other Events
Other events reported post marketing to have been observed in temporal association with VIAGRA and not listed in the clinical trials adverse reactions section include:
Nervous: seizure, seizure recurrence and anxiety
Urogenital: priapism, haematuria and prolonged erection
Ocular: diplopia, temporary vision loss/decreased vision, ocular redness or bloodshot appearance, ocular burning, ocular swelling/pressure, increased intraocular pressure, retinal vascular disease or bleeding, vitreous detachment/traction and paramacular oedema.
Non-arteritic anterior ischaemic optic neuropathy (NAION), a cause of decreased vision including permanent loss of vision, has been reported rarely post-marketing in temporal association with the use of phosphodiesterase type 5 (PDE5) inhibitors, including VIAGRA. Most, but not all, of these patients had underlying anatomic or vascular risk factors for developing NAION, including but not necessarily limited to: low cup to disc ratio (“crowded disc”), age over 50, diabetes, hypertension, coronary artery disease, hyperlipidaemia and smoking. An observational study evaluating whether recent use of PDE5 inhibitors, as a class, was associated with acute onset of NAION suggests an increase in the risk of NAION with PDE5 inhibitor use (see CONTRAINDICATIONS and PRECAUTIONS).
Body as whole: hypersensitivity reaction.
Special senses: Cases of sudden decrease or loss of hearing have been reported post marketing in temporal association with the use of PDE5 inhibitors, including VIAGRA. In some of the cases, medical conditions and other factors were reported that may have also played a role in the otologic adverse events. In many cases, medical follow-up information was limited. It is not possible to determine whether these reported events are related directly to the use of VIAGRA, to the patient’s underlying risk factors for hearing loss, a combination of these factors, or to other factors (see PRECAUTIONS).
DOSAGE AND ADMINISTRATION
VIAGRA tablets are for oral administration.
Use in Adults
The recommended dose is 50 mg taken as needed approximately one hour before sexual activity. Based on the efficacy and toleration, the dose may be increased to 100 mg or decreased to 25 mg. The maximum recommended dose is 100 mg. The maximum recommended dosing frequency is once per day.
Use in the Elderly
Since sildenafil clearance is reduced in elderly patients, a first dose of 25 mg should be considered. Based on efficacy and toleration, the dose may be increased to 50 mg and 100 mg.
Use in Patients with Impaired Renal Function
The dosing recommendations for Use in Adults should be followed for patients with mild to moderate renal impairment (Clcr = 30-80 mL/min).
Since sildenafil clearance is reduced in patients with severe renal impairment (Clcr <30 mL/min) a 25 mg starting dose should be considered. Based on efficacy and toleration, the dose may be increased to 50 mg and 100 mg.
Use in Patients with Impaired Hepatic Function
Since sildenafil clearance is reduced in patients with hepatic impairment (e.g., cirrhosis) a 25 mg starting dose should be considered. Based on efficacy and toleration, the dose may be increased to 50 mg and 100 mg.
Use in Patients using Other Medicines
Concomitant use of potent CYP 3A4 inhibitors has been associated with increased plasma levels of sildenafil (e.g., erythromycin, 182%, saquinavir, 210%). It can also be expected that more potent CYP 3A4 inhibitors such as ketoconazole and itraconazole would result in increased plasma levels of sildenafil (see Effects of Other Medicines on VIAGRA). Since higher plasma levels may increase both the efficacy and incidence of adverse events, a starting dose of 25 mg should be considered in these patients.
Given the extent of the interaction with patients receiving concomitant therapy with ritonavir, it is recommended not to exceed a maximum single dose of 25 mg of sildenafil in a 48 hour period (see Effects of Other Medicines on VIAGRA).
In order to minimise the potential for developing postural hypotension, patients should be stable on alpha-blocker therapy prior to initiating sildenafil treatment. In addition, initiation of sildenafil at lower doses should be considered (see PRECAUTIONS and INTERACTIONS WITH OTHER MEDICINES).
Use in Children
VIAGRA is not indicated for use in children.
OVERDOSAGE
Overdose information is limited. In studies with healthy volunteers, of single doses up to 800 mg, adverse events were similar to those seen at lower doses but incidence rates and severities were increased.
In cases of overdose, standard supportive measures should be adopted as required. Sildenafil blood levels are not clinically useful. Monitor ECG and blood pressure in symptomatic patients. Renal dialysis is not expected to accelerate clearance as sildenafil is highly bound to plasma proteins and not eliminated in the urine.
Contact the Poisons Information Centre on 13 11 26 for advice on the management of an overdose.
PRESENTATION AND STORAGE CONDITIONS
The 25 mg tablets are blue film-coated, rounded diamond-shaped tablets, marked PFIZER on one side and VGR 25 on the other.
The 50 mg tablets are blue film-coated, rounded diamond-shaped tablets, marked PFIZER on one side and VGR 50 on the other.
The 100 mg tablets are blue film-coated, rounded diamond-shaped tablets, marked PFIZER on one side and VGR 100 on the other.
VIAGRA tablets are presented in PVC/Al blister or PVC/PE/PCTFE (Aclar)/Al blister packs of 4, 8 and 12 tablets. Not all pack sizes may be marketed.
NAME AND ADDRESS OF THE SPONSOR
Pfizer Australia Pty Ltd ABN 50 008 422 348 38-42 Wharf Rd West Ryde NSW 2114.
POISON SCHEDULE DATE OF APPROVAL Date of Most Recent Amendment
Ò Registered trademark Pfizer Inc.
This is the first in a series of concept papers commissioned by the International Trachoma Initiative (ITI) to bridge the mission and programmatic work of ITI with the current discussions in other fields related to health and development issues in poor countries. The general aim of the concept papers is to assist ITI to clarify and articulate the success of its current programs to eliminate blind
Shipping Products Can Products be sent to: PRODUCT MAIN NAME Acetyl-L-Carnitine Acomplia Acomplia Amantadine Abramicina Aminoguanidine Anacervix AndroCheck AndroPatch AndroPatch Antaxone Arimidex Artemisinin Aslavital B17 Laetrile Injectable PRODUCT MAIN NAME B17 Laetrile Tablets B17 Laetrile Tablets BEC5 Curaderm Beyond Any Multip
 PRODUCT INFORMATION
PRODUCT INFORMATION