Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Mod10 nov 04
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
CONTENTS
11 General Anaesthetics (GA) and Conscious Sedation
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationMODULE TEN MINOR ORAL SURGERY, ANAESTHESIA AND SEDATION INTRODUCTION
This module describes the various minor oral surgical procedures that maybe performed in either a general dental practice or hospital oral surgerydepartment. The use of anaesthetics and sedation in dentistry is alsodiscussed. LEARNING OUTCOMES
On completion of this module, students will:
Be aware of the various minor oral surgical procedures that may beperformed within dentistry
Have gained a general understanding of the use of anaesthetics indentistry
Appreciate the need for the use of oral sedation in dentistry
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module
OBJECTIVES
1. Explain what is meant by the term ‘minor oral surgery’
2. List five different minor oral surgical procedures
3. State four reasons why a tooth may be extracted
4. Outline the ‘surgical plan’ for minor oral surgery
5. Identify the instruments used for tooth extraction and minor oral
6. List three reasons for the use of sutures
7. Describe what is meant by ‘electrosurgery’
8. Explain the difference between analgesia and anaesthesia
9. Name two anaesthetic agents most commonly used in anaesthetic
10. State the purpose of ‘topical’ anaesthetics
11. Explain why ‘self-aspirating’ syringes are recommended when
administering a dental local anaesthetic agent
12. Describe the difference between a ‘dental infiltration’ and ‘regional
13. Explain the difference between ‘inhalation anaesthesia’ and
14. State two ways by which conscious sedation may be achieved
15. Name the Act which governs the use of anaesthesia and other drugs
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationMINOR ORAL SURGERY
Minor oral surgery usually refers to surgical procedures that may beperformed by the general dental practitioner (GDP) in the dental surgery.
Minor oral surgical procedures that may be carried out are:
Tooth removal (extraction)Removal of retained rootApicectomyRemoval of cystsAlveolar ridge preparationFrenectomyBiopsyElectrosurgery
Tooth Removal
Tooth removal is one of the oldest and most commonly performed surgicaloperations, frequently referred to as tooth extraction. There are severalreasons why a tooth may have to be extracted:
Failure of conservative treatmentFailure of endodontic treatmentDental abscessCaries, where conservation is not viable or not acceptable to the patientAs part of the treatment plan, e.g. dentures, implantationAs part of an orthodontic treatment planWhere teeth are impacted, e.g. wisdom teeth
Two possible surgical approaches to tooth extraction may be considered:
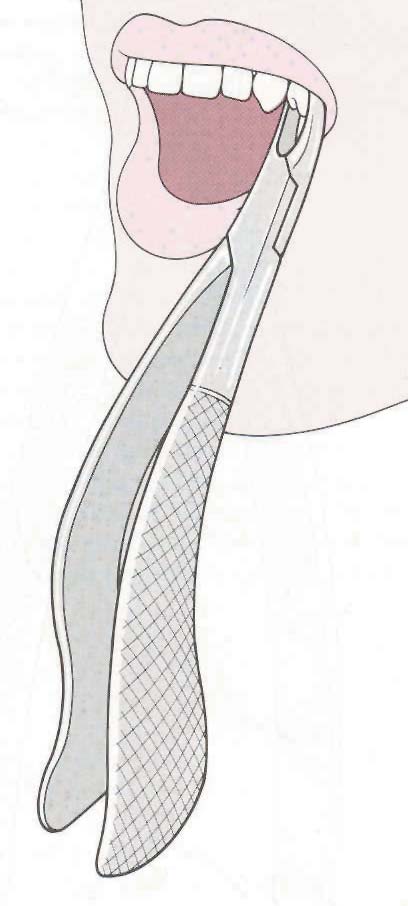
Forceps Extraction
The blades of the forceps are forced down into the periodontal ligament,between the tooth root and bony socket wall; the root of the tooth is grippedfirmly between the forceps blades and, by gentle but firm movements, thesocket wall is expanded to permit removal of the tooth.
Surgical Extraction
Surgical extraction may be required to remove the tooth from its socket; thisapplies for impacted teeth, or fragments of bone or teeth which have becomeretained or buried in the jaws. In order to remove the tooth and/or roots, itwill be necessary to lift a flap of gum with a scalpel and then it may benecessary to use surgical burs to remove bone and cut the tooth into smallerpieces, which can then be removed through the access available.
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Instruments Used For Tooth Extractions
Forceps are made from high quality steel to provide the necessary strengthrequired when removing teeth. Forceps consist of three parts:
1. The Blades –The blades should be sharp to facilitate placement onto 2. The Hinge – The hinge should move freely, but must not be worn or 3. The Handles – The handles are serrated to give a firm handhold to
Forceps are available with different characteristics. They may have simple orpointed blades, and the blades may be in line with the handles or at rightangles to the handles. The handles may be straight or curved. The differentconfigurations of forceps design are to allow access and grip of the forceps tothe upper or lower teeth, single or multi-rooted teeth, and teeth on the left orright sides of the mouth. Elevators
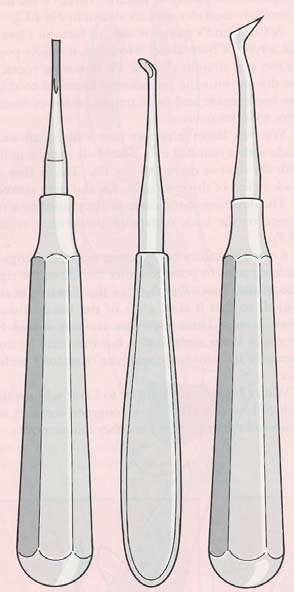
Elevators are used to remove roots or impacted teeth from their socketswhere the use of forceps is considered inappropriate. They are used to leverthe tooth out of the socket. Many different types of elevators are available andare usually identified by thename of the surgeon whooriginally designed them.
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationLuxation Instruments
Luxation instruments are used to cut the fibres around a tooth tomake an extraction easier. They are sharper and finer thanelevators.
Minor Oral Surgery Procedures Retained Roots
Retained roots may need to be surgically removed if part of the root
fractures and remains in the jaw during tooth removal, or if the
crown of the tooth is completely destroyed and there is insufficienttooth tissue to grip with forceps. Apicectomy
Surgical removal of the apex (tip) of the root of the tooth (beneath the gum)may be required when previous endodontic treatment has failed.
Removal of Cysts
A cyst is an abnormal fluid-filled cavity surrounded by a lining of epithelialcells. Cysts may occur in the jawbone; they may develop at the apex of a toothwith an infected or non-vital pulp. Other cysts are also found. If leftuntreated, cysts can grow and cause swelling or displace other adjacentteeth.
Alveolar Ridge Preparation
Occasionally, before denture construction, it may be necessary to trim orremove protruding sharp areas of bone which form the denture-bearingridges, so that stable and comfortable dentures can be made.
Frenectomy
When a very prominent fraenum may be present between the upper centralincisors and associated with an unsightly gap between these teeth, afrenectomy (removal of the fraenum) may be required, so that the gapbetween these two teeth can be orthodontically reduced, or simply to enableeffective toothbrushing or construction of dentures. This procedure is mostcommonly performed during childhood.
A biopsy is the surgical removal of a piece of tissue for microscopicexamination in order to determine the nature of a disease.
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Minor Oral Surgery – The Surgical Plan
Many of the above surgical procedures can be carried out in the dental chairunder local anaesthetic. However, depending on the length of time, themedical status of the patient and the stress likely to be experienced, some ofthese operations are carried out by oral surgeons in hospital operatingtheatres under general anaesthetic. All oral surgical procedures are carriedout in accordance with a common plan or sequence, as outlined below:
Raising a Flap
First, using a scalpel, an incision is made into the gingiva overlying theoperation site. Where the gingiva overlies the bone, the released area ofgingiva is lifted from the bone using an instrument called a periostealelevator and held to one side by a tissue retractor. Bone Removal
Bone removal is achieved using bone forceps and burs. If burs are used, theymust be cooled with a stream of sterile ‘isotonic’ saline, which is compatiblewith body cells and stops the bone being drilled from overheating, whichwould cause tissue damage.
Extraction
Extraction of the exposed tooth or root is achieved using suitable elevators orforceps. Cleaning (Debridement)
Any spicules of bone are removed with bone forceps and the margins of thesocket are smoothed with a bone file. Small bone chips and filings areremoved from the socket and the operative area by irrigation with sterilesaline delivered by a Hunt’s water syringe. Sutures (Stitches)
Once the socket and operation wound are cleared of all debris, the gingivaethat has been lifted is sutured back in place. Sutures are normally made ofblack braided silk, which need to be removed after seven days, or of catgut,which resorb (dissolve) after a few days.
In general, sutures perform three functions:
1. They control bleeding2. They promote healing3. They restore normal anatomy
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationElectrosurgery
Electrosurgery is a method of cutting and coagulating softtissues by means of passing high-frequency radio wavesthrough the tissue cells. By this method, a dentist can cutthrough tissue, reducing much of the bleeding normallyexperienced using a scalpel blade. Various shapes and sizesof loop electrodes can be used to remove and shape tissuewhere necessary and larger ball-ended or bar electrodes canbe used to arrest bleeding.
Electrosurgery has many uses, most notably in restorativedentistry, some of the most common procedures being,exposing unerupted teeth, gingivectomies and troughing(widening of the sulcus) for crown and bridge impressions. Electrosurgery unit foruse in implantology andmaxillo-surgeryANAESTHESIA AND SEDATION
Most dental procedures are carried out on highly sensitive tissues. Effectivepain control is necessary to enable patients to tolerate such operations.
Patients may be given a dental local anaesthetic (LA) to make an area numband insensitive to pain without affecting the other senses (analgesia), or ageneral anaesthetic (GA) to produce loss of all sensation, includingconsciousness. Dental Local Anaesthesia
Painful sensations from dental structures are directed to the brain alongspecific nerve pathways, where they are interpreted as pain. Deposition oflocal anaesthetic solutions around any of these nerve endings temporarilystops them from conveying messages to the brain. After some time, the effectof the local anaesthetic wears off and the nerve impulses return to normal. Local Anaesthetic Agents
Local dental anaesthetics are most commonly based on Lidocaine, formerlyknown as Lignocaine, or a related amide substance, such as Mepivicaine,Articaine or Prilocaine.
They are frequently formulated with a vasoconstrictor – commonlyAdrenaline (also known as Epenephrine), or Octapressin (also known asFelypressin) – and supplied in glass cartridges. Some patients are medicallycompromised and must not receive an anaesthetic with a vasoconstrictor e.g. patients who are prescribed anti coagulant drugs.
Adrenaline or Octapressin are used to reduce the rate that the anaesthetic iswashed away by the blood stream leading to more prolonged anaesthesia.
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Batch Numbering and Good Manufacturing Practice (GMP)
Anaesthetic drugs are manufactured in plants that operate to the mostexacting standards. These standards are laid down and monitored bygovernment, health and medicine regulatory authorities worldwide. Everyaspect of their manufacture and distribution is traced using a batchnumbering system. This information is screen printed on the side of thecartridges, embossed on the sterile packaging and also on the outercardboard box in which the anaesthetic cartridges are packed. Informationon expiry dates is similarly presented. Topical (or Surface) Anaesthetics
Topical anaesthetics are often formed from the same drugs mentioned above. They are formulated as gels or sprays to anaesthetise a small area of mucousmembrane or gingiva, so that the injection is more comfortable.
Dental Equipment for Local Anaesthesia Anaesthetic Cartridges
Dental anaesthetic solutions are supplied in sterile glass cartridges. Thecartridges have a rubber diaphragm on one end and a rubber plug at theother end. Cartridges are used in either a cartridge syringe or the singlepatient use injection system. Cartridges are available in either 1.8ml or 2.2ml. The size most commonly used in the UK is 2.2ml. Dental Syringes
If an injection of anaesthetic solution containing adrenaline is accidentallyinjected into a blood vessel, serious adverse drug reactions may occur. Mostdentists avoid this complication by using self-aspirating syringes andcartridges. These are designed so that once the needle has been inserted intothe site, and prior to injecting the anaesthetic solution, pressure can bereleased from the syringe plunger; the rubber bung in the cartridge recoils,draining a small amount of fluid back into the syringe.
If the fluid contains blood, this indicates the needle is in a blood vessel; the
needle is repositioned and another aspiration test performed. If the fluid isclear, injection of the anaesthetic solution can commence.
The single patient injection systems offer safety and ease of use through self-aspirating systems and accidental inoculation injury prevention isincorporated into the design.
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationNeedles and Cartridges
Needles and cartridges are disposable itemsand are for single use only. They should bedisposed of as clinical waste in a rigid sharpscontainer. Administration of Local Anaesthetics (LA)
Several types of injection may be used. The dentist will select the typeaccording to the nature of treatment undertaken, length of operating timeand the amount of anaesthesia necessary for the operation. Types ofinjections are as follows:
Dental Infiltration
Dental infiltration injections are used to anaesthetise teeth for restoration orendodontic work, or for deep scaling and root surface debridement. Thesyringe needle is passed through the oral mucous membrane; the solution isthen injected, so that it lies in close contact with the surface of the bonecovering the apex of the tooth. The solution infiltrates through the bone andreaches the nerve endings as they enter the tooth through the apicalforamen. Thus, the pulp of the tooth and the surrounding gingiva becomesnumb.
Dental infiltrations are not very successful in the lower jaw (mandible) as thebone is very dense and the anaesthetic solution does not permeate to thetooth. Regional Block Injections
In regional block injections, the anaesthetic solution is deposited around amain nerve trunk, as opposed to a small nerve branch. This blocks allimpulses in the area that the nerve supplies. In dentistry, inferior dentalblocks numb the inferior dental nerve, the main nerve supply to the lower jaw,just as it exits the mandible through the inferior dental foramen. Impulsesfrom the lips, tongue and all the teeth on that side are blocked from reachingthe brain; all these structures are numbed by a single injection.
Intra-osseous and Intra-ligamentary Injections
Less commonly used techniques are intra-ligamentary and intra-osseousinjections, which require specialised equipment and introduce theanaesthetic under pressure using a very small needle, either down the sulcus(side of the tooth) into the periodontal ligament or through the bone, therebyachieving very rapid anaesthesia. M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
GENERAL ANAESTHETICS (GA)
General anaesthetics (GA) produce a state of unconsciousness with total lossof all sensation. GA may be required where the use of LA is inappropriate orinsufficient. The drugs usually employed for general anaesthetics are nitrousoxide, halothane and methohexitone. Nitrous oxide is administered withoxygen.
GA agents may be classified as either inhaled or intravenous. Inhalation Anaesthesia
For inhalation anaesthesia, the anaesthetic gases are administered to apatient through a tube attached to an anaesthetic machine. The gases passfrom the lungs into the blood stream and affect the normal functioning of thebrain, producing the state of unconsciousness and loss of all sensation.
Intravenous Anaesthesia
Intravenous injection of drugs may be employed to produce two differentresults: general anaesthesia or sedation. CONSCIOUS SEDATION
Most patients are able to accept dental treatment in which any discomfort isnumbed by LA. There are some patients, however, who are unable to toleratethis approach unless they are helped with sedation. Conscious sedation isthe administration of drugs which depress the central nervous systemsufficiently to make the dental treatment more acceptable while allowingverbal communication to be maintained. Thus, the patient does not becomeunconscious. The patient still requires the use of LA to numb the sensationof pain.
Conscious sedation can be achieved in three ways:
Oral Sedation
Oral sedatives may be taken as a single dose one hour before treatment ordivided into three doses; the first dose is taken the night before treatment,the second dose on waking, and the third dose one hour before treatment. Relative Analgesia (RA) (Inhalation Analgesia)
Relative analgesia (RA) is achieved by inhaling the sedative gases from a RAmachine, sometimes known colloquially as ‘gas and air’. Here sedation isachieved by the administration of nitrous oxide and at least 30% oxygen.
The sedated patient remains co-operative and responsive to verbalinstructions.
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationIntravenous sedation
Conscious sedation can also be achieved by the injection of sedative drugs,which reduce anxiety, but allow the patient to retain verbal contact. Drugsadministered intravenously are more effective than the same drugs takenorally. In addition they induce amnesia, where the patient will have little or nomemory of the procedure.
Legal Requirements of the Medicines Act 1968
Anaesthetics and other drugs used in the practice of dentistry are governedby the Medicines Act 1968 and the various regulations issued under that Act. Regulations exist which determine how the drugs are distributed, who isqualified to promote drugs and the ways in which they can be advertised. General Anaesthesia in Dentistry
The first recorded general anaesthetic given to a patient by a dentist was inBoston, Massachusetts, in 1846, when William T. G. Morton administeredether to a man having a tumour removed from his neck. In December of thatyear, dentists in Britain were giving ether to anaesthetise patients for dentalextractions.
The Poswillo Report, commissioned by the Government to look into thepractice of anaesthesia in dentistry, was published in 1990. It concluded:
‘…that if anaesthesia was to continue in general dental practice, thestandard of practice found in the hospitals had to be introduced into thedental clinics. ’
As a result, many dentists were unable to continue to offer GA and patientsrequiring GA for their dental treatment had to be referred to hospital.
In November 1998, in light of public concern and following considerabledebate, the GDC issued revised ethical guidelines on the use of GA. Theimpact of the guidelines was immediate. Between November 1998 andDecember 1998, the number of courses of treatment including GA fell from22,349 to 10,520. In March 2001, the number of treatments in general dentalpractice using GA was less than one sixth of the total for December 1998. There has been an increase in the number of courses involving sedation overthis same period: 9,593 in March 2001, compared to 5,150 in December 1998.
In July 2000, the Department of Health (DoH) produced a review of generalanaesthesia and sedation called A Conscious Decision. The reportrecommended that:
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
• From 1 January 2002, GA for dental treatment should only take place in a
hospital or suitably equipped and staffed place.
• The use of GA to reduce pain and anxiety with dental treatment should be
discouraged. GA should only be undertaken when absolutely necessary.
Other specific recommendations of the report include:
• High standards of conscious sedation must be attained. This should
include the use of dedicated assistants, appropriate undergraduate andpostgraduate training, and similar arrangements for patient assessment,consent and patient escorts as for GA.
• Higher standards of resuscitation are required in dental practices. This
must include training in basic life support for all clinical staff and theirassistants.
• Members of the team must practise resuscitation at regular intervals. All
clinical staff in dental practices must undertake training to ensure thatthey deal effectively with medical emergencies. All training must berecorded and monitored by the Primary Care Trusts.
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
• Minor oral surgery usually refers to surgical procedures that may be
performed by the general dental practitioner.
• Tooth extraction is one of the most commonly performed surgical
procedures carried out in dentistry. Tooth extraction may be required fora number of reasons. Two approaches to tooth extraction may be forcepsextraction or surgical extraction.
• All minor oral surgical procedures are carried out in accordance with a
common plan, raising a flap, bone removal, delivery, debridement andsuture.
• Electrosurgery is a method of cutting and coagulating tissues by means
of passing high-frequency radio waves through the tissue cells.
• Local anaesthesia (LA) makes an area numb without affecting the other
senses (analgesia), general anaesthetic produces a state ofunconsciousness.
• Local anaesthetics are based on Lidocaine and frequently contain
adrenaline. All anaesthetics are batch numbered. Standards ofproduction of anaesthetic drugs are monitored by government, andhealth and medical regulatory authorities worldwide.
• Topical (or surface) anaesthetics may be used to anaesthetise small
areas of mucous membrane so that the insertion of the needle is not felt.
• Local anaesthetic equipment comprises the anaesthetic cartridge, needle
and self aspirating syringe. The needle and cartridge are designed forsingle use only and should be disposed of in a rigid sharps container.
• Dental infiltration injections are used to restore teeth and for endodontic
work. The anaesthetic solution infiltrates through the bone and reachesthe nerve endings as they enter the tooth at the apical foramen. Dentalinfiltrations are not very effective on mandibular pre-molars and molarsas the bone is too thick for the solution to permeate.
• Regional block injections are used to numb the inferior dental nerve, the
• Less commonly used injections are the intra-osseous and intra-
• General anaesthesia (GA) may be required when the use of local
anaesthesia is insufficient or inappropriate. GA may be administered byinhalation or intravenous injection. M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
• Conscious sedation is the administration of drugs which depress the
central nervous system. The patient remains conscious, so LA is stillrequired. Conscious sedation may be administered by either oral sedationor relative analgesia (inhalation analgesia).
• Anaesthetics and other drugs used in dentistry are governed by the
Medicines Act 1968 and other amendments issued under that Act.
• In July 2000, the Department of Health produced a review of general
anaesthesia and sedation. As a result of that review, from January 2002,GA for dental treatment may only be carried out in a hospital. Otherrecommendations of the report include, high standards of conscioussedation must be attained, higher standards of resuscitation are requiredin dental practices and that members of the dental team must regularlypractise resuscitation techniques.
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationGLOSSARY
A swollen area accumulating with pus in a body tissue
Anaesthetic
A substance that produces insensibility to pain
Analgesia
The scientific study of the body structure in humansor animals
Apicectomy
The removal of the tip of the root of a tooth
The examination of tissue removed from the body todiscover the presence, cause or extent of disease
A sac containing fluid, gas, soft or morbid matter
Diaphragm
A thin sheet of material used as a partition
Electrodes
A conductor through which electricity enters or leaves
Epithelial Frenectomy Gingivectomy Haemorrhaging Implantation Infiltrates Inhalation Intra-osseous
Intra = within or upon; Osseus = relating to bone
Intravenous Isotonic M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Prosthetics
The branch of dentistry supplying prostheses
Sedation
A state of rest or sleep produced by a sedative drug
The joining of the edges of a wound by stitching
Undergraduate
A student at university who has not yet taken a degree
Vasoconstrictor
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and SedationREFERENCES H. Levison. (2004). Textbook for Dental Nurses (9th edition). Blackwell Monksgaard. R. G. Smith. (1993). Dental Surgery Assistants Handbook (2nd edition). Mosby. Further Reading Dr J Meecham. Local Anaesthesia – A Complete Update. Better Practice 2000. General Anaesthetics. March 2001. The Dental Practice Board – Annual Review 2000/2001, pages 25 – 26. General Anaesthesia For Dental Treatment To Be Restricted To Hospitals By January 2002. BDTA Newsletter, No 10, 28 July 2000. Maintaining Standards. General Dental Council, 2001.
Atmospheric Responsibility and Climate Change The global atmosphere is a vital, fragile, and precious resource. Without it there would be no life onearth. Its overall stability is a crucial matter, not only for the sake of human welfare, but also for the sakeof all the many natural goods and services on which human welfare depends. With the build up ofgreenhouse gases in the atmosphere,
Refl exiones sobre la organización del sistema sanitario Resumen del informe CAE n° 103 (31/12/2012) Sinopsis Este informe privilegia dos aspectos:• ¿Cuáles son las justifi caciones económicas de la intervención del • ¿Qué pensar de los sistemas vigentes de tarifi cación de los actos La primera interrogación nos remite a los argumentos habituales, en favor de la in
 Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
MINOR ORAL SURGERY
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
MINOR ORAL SURGERY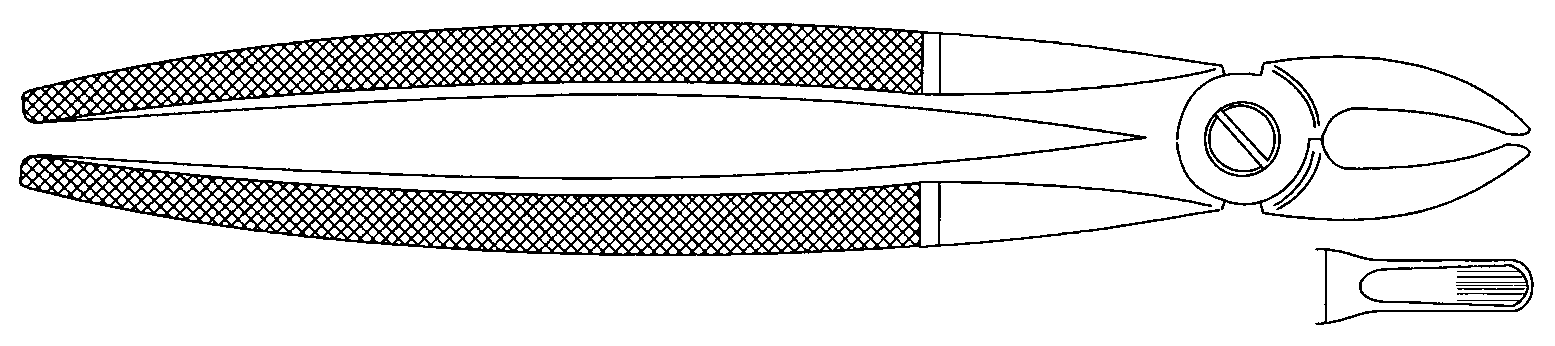
 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Instruments Used For Tooth Extractions
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Instruments Used For Tooth Extractions  Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Luxation Instruments
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Luxation Instruments  Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Electrosurgery
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Electrosurgery M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Batch Numbering and Good Manufacturing Practice (GMP)
M i n o r O r a l S u r g e r y, Anaesthesia and Sedation Module 10
Batch Numbering and Good Manufacturing Practice (GMP) Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Needles and Cartridges
Module 10 M i n o r O r a l S u r g e r y, Anaesthesia and Sedation
Needles and Cartridges