Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
2002; 04
High dose chemotherapy and autologous stem cell transplantation in patients with peripheral T-cell lymphoma not achieving complete response after induction chemotherapy. The GEL-TAMO experience JOSÉ RODRIGUEZ, MARIA DOLORES CABALLERO, ANTONIO GUTIERREZ, MARCO GANDARILLAS, JORGE SIERRA, ARMANDO LOPEZ-GUILLERMO, ANNA SUREDA, JAVIER ZUAZU, JESUS MARIN, REYES ARRANZ, ENRIC CARRERAS, ANGEL LEON, ALBERTO FERNÁNDEZ DE SEVILLA, JESUS F. SAN MIGUEL, EULOGIO CONDE FOR THE GEL/TAMO SPANISH GROUP Background and Objectives. Patients with aggressive
non-Hodgkin’s lymphomas (NHL) who do not obtain a com-
In adult patients, the majority of aggressive T-cell
non-Hodgkin's lymphomas (NHL) are peripheral T-
plete response (CR) after induction chemotherapy have a
cell lymphomas (PTCL).1 Indeed, excluding cutaneous,
poor prognosis. However, provided they are sensitive to the
lymphoblastic and adult T-cell leukemia/lymphoma,
first regimen of chemotherapy, 25-40% of them with a B-
PTCL constitute approximately 10% of NHL.2 No stan-
cell phenotype may achieve long-term survival when treat-
dard therapy has been established to treat this type of
ed with high dose chemotherapy and autologous stem cell
lymphoma and usually,3-5 but not in all cases,6,7 when
transplantation (HDC/ASCT). The aim of this study was to
standard therapeutic regimens for aggressive lym-
analyze the efficacy of this therapy in the corresponding
phomas are applied, the T-cell immunophenotype con-
patients with peripheral T-cell lymphoma (PTCL).
fers a poor prognosis. However, results of salvage ther-
Design and Methods. We retrospectively evaluated the
apies including high-dose chemotherapy and autolo-
efficacy of ASCT in 35 patients with PTCL from the GEL-
gous stem cell transplantation (HDC/ASCT) seem to be
TAMO registry, who did not achieve a CR to standard induc-
similar to those observed for the corresponding B-cell
tion chemotherapy regimens for aggressive NHL. Thirty-one
patients underwent transplantation after achieving a partial
Failure to respond to induction therapy is defined as
response (PR) and 4 patients were non-responders.
not achieving a complete response (CR) to the first-line
Results. Following HDC/ASCT, 23 (66%) of the patients
therapy and represents a therapeutic challenge. Data
achieved a CR, 4 (11%) a PR and in 7 (20%) cases the
from corresponding B-cell lymphomas indicate that
transplant failed. One patient was not evaluated because of
approximately 40% of these patients can be salvaged
early toxic death. With a median follow-up of the survivors
with HDC/ASCT.8,10,11 However, the efficacy of this ther-
of 37.5 months, 18 patients (51%) are alive and 15
apy in patients with PTCL in whom induction has failed
patients (43%) are free of disease. Transplant-related mor-tality rate at 100 days was 11% and at 5 years the proba-
is less well defined. Recently, Kewalramini et al. report-
bilities of survival, freedom from progression and disease-
ed that patients with primary refractory PTCL treated
free survival for complete responders were 37%, 36% and
with HDC/ASCT respond in a similar manner to those
55% respectively. Pre-transplant lactate-dehydrogenase lev-
with a corresponding primary refractory aggressive B-
el, age-adjusted International Prognostic Index (aa-IPI) and
cell lymphoma.9 To investigate this possibility further,
tumor score correlated with survival.
we analyzed GEL-TAMO co-operative group patients
Interpretation and Conclusions. One third of the
with PTCL who had not achieved a complete response
patients with PTCL who fail to achieve CR to the first
after induction chemotherapy and who then underwent
chemotherapeutic regimen can be rescued with HDC/ASCT.
HDC/ASCT as a salvage therapy. Our data suggest that
Pre-transplant values of IPI and tumor score risk systems for
patients with this type of lymphoma who fail to respond
aggressive lymphomas were useful to predict subsequent
to induction therapy, do indeed fare similarly to patients
with the corresponding aggressive B-cell lymphomawhen treated with HDC/ASCT.
Key words: autologous stem cell transplantation,T-cell lymphoma. Design and Methods Patients
http://www.haematologica.org/2003_12/1372.htm
Between July 1990 and December 1999, the hospitals
participating in the Spanish Group for Lymphoma and
Autologous Transplantation (GEL-TAMO) treated 115PTCL patients with HDC/ASCT. In this report we retro-spectively selected the 35 (30%) patients from the reg-
From the Servicios de Hematología Hospital Universitario Son Dureta, Palma deMallorca (JR, AG); Hospital Clínico Universitario, Salamanca (MDC, JSM); Hospital
istry who had failed to respond to first-line induction
Marqués de Valdecilla, Santander (MG, EC); Hospital de la Santa Creu i Sant Pau,
treatment and who received HDC/ASCT as part of their
Barcelona (JS, AS); Hospital Clinic i Provincial, Barcelona (ALG, EC); Hospital de laVall de Hebron, Barcelona (JZ); Hospital Nuestra Señora de Aranzazu, San Sebast-
salvage treatment. The clinical characteristics of the
ian (JM); Hospital de la Princesa, Madrid (RA); Hospital General de Jerez, Jerez de
patients at diagnosis and at the time of transplantation
la Frontera (AL); Institut Catala d’Oncologia, Barcelona, Spain (AFdS).
are set out in Table 1. Briefly, at diagnosis 47% of the
Correspondence: Dr. José Rodríguez, Servicio de Hematología, Hospital
patients had an age-adjusted IPI (aa-IPI) score of 2 or
Universitario Son Dureta, Av/Andrea Doria 55, Palma de Mallorca 07014, Spain.
3. The maximal response to induction therapy in most
haematologica/journal of hematology vol. 88(12):december 2003
ASCT in peripheral T-cell lymphoma after failed induction
Table 1. Clinical characteristics. Table 2. Transplant-related factors. TBI: total-body irradiation; BEAM: carmustine, etoposide,cytarabine, melphalan; BEAC: carmustine, etoposide, cytarabine,cyclophosphamide; CVB: carmustine, etoposide,cyclophosphamide; BM: bone marrow; PB: peripheral blood;G-CSF: granulocyte colony-stimulating factor;GM-CSF: granulocyte-macrophage colony-stimulating factor.BM, bone marrow; LDH, lactate dehydrogenase; β2M,
β2-microglobulin; NA, not available; CHOP, cyclophosphamide,
sive NHL (22 patients CHOP, 3 MegaCHOP, 6
adriamycin, vincristine, prednisone.
CYTABOM). A patient initially misdiagnosed withHodgkin’s disease received treatment with ABVD
patients [(31/35) (89%)] was only partial although
and 2 patients received radiotherapy pretransplan-
4/35 (11%) were refractory or the disease pro-
tation. The median time from diagnosis to trans-
gressed during treatment. At the time of trans-
plantation was 7 months and the conditioning reg-
plantation, 43% of the patients had extranodal dis-
imens were based on BEAM or BEAC in 23 cases,
total body irradiation/cyclophosphamide in 6 and
patients (91%) had an ECOG performance status of
0-1 and 3% of the patients had one or more bulkymasses. High levels of β2-microglobulin and lac-
Response assessment and follow-up
tate dehydrogenase (LDH) were detected in 45%
criteria
and 29% of the patients, respectively.
The response to therapy was evaluated 1, 3 and
6 months after transplantation and, thereafter,
Therapy
every 6 months by the investigator responsible in
The first-line and conditioning regimens for trans-
each center. Evaluation followed the standard
plantation are presented in Table 2. All patients
guidelines laid out by Cheson et al.12 Complete
received standard induction regimens for aggres-
response (CR) was defined as the disappearance of
haematologica/journal of hematology vol. 88(12):december 2003
all clinical evidence of lymphoma for a minimum of
4 weeks, with no persisting symptoms related to
the disease. Prior to transplantation a complete
restaging was performed in all patients. To cate-
gorize a patient as a complete responder after
transplantation, residual masses had to remain
A partial response (PR) was defined as a decrease
% surviving
greater than 50% of the sum of the products of the
two longest diameters of all measurable lesions for
at least 4 weeks, and non-measurable lesions also
had to decrease by at least 50%. For patients to be
considered in this category no lesions could increase
Months from transplant
in size and no new lesion could appear. A state of
progressive disease (PD) was defined as any increase
greater than 25% in the sum of the diameters of any
measurable lesions or the appearance of a new
lesion. We defined transplant-related mortality as
death within 100 days of HDC/ASCT not related to
the disease, relapse or progression. Standard vari-
ables to calculate the age-adjusted International
Prognostic Index13 and other variables of known
% progression-free
prognostic importance, such as the MD Anderson
tumor score,14 were evaluated at the time of diag-
Months from transplant Statistical methods
Overall survival (OS), freedom from progression
(FFP) and disease-free survival (DFS) were measured
from the date of transplantation, and were esti-
mated according to the Kaplan-Meier method.15
Comparisons between the variables of interest at
the time of transplantation were performed by the
log-rank test.16 All p-values reported were two-sided
and statistical significance was defined at a p-val-
% disease-free Months from transplant Outcome
Response to transplant was as follows: 66%
Figure 1. Overall survival, freedom from progression and disease-free survival.
achieved a CR, 11% a PR, and in 20% of the cases
the treatment failed. The disease response was notevaluated for 1 patient because of early death post-transplantation. After a median follow-up of thesurvivors of 37.5 months (range: 3-109), 18 patientsout of the 35 transplanted (51%) were alive and 15(43%) showed no evidence of the disease. Of the 17patients who died, 12 (71%) died from progressive
Prognostic factors
disease, 4 (24%) as a result of treatment-related
Given the relatively small number of patients, we
causes, and 1 patient died from a second neoplasia
only performed univariate analysis to investigate
while deemed to be free of lymphoma at this point.
which variables might be associated with the pos-
The transplant-related mortality was 11% (2 cases
sible outcomes, including OS and FFP. We found
of adult respiratory distress syndrome, one sepsis,
that 2 or 3 aa-IPI risk factors, a tumor score >2,14
and one hepatic veno-oclusive disease). The actuar-
and an elevated LDH at the time of transplantation
ial OS at 5 years was 37% (95% confidence inter-
were associated with reduced survival (Figure 2).
val (CI), 16% to 58%), the FFP was 36% (95% CI,
However, we could not identify any factor at trans-
17% to 55%), and the DFS for complete responders
plantation that provided prognostic information
was 55% (95% CI, 30% to 80%: Figure 1).
haematologica/journal of hematology vol. 88(12):december 2003
ASCT in peripheral T-cell lymphoma after failed induction
Discussion p < 0.001
The most recent series5,17 of patients with
advanced stages of aggressive NHL treated withstandard protocols indicate that the T-cell
0-1 risk factors of a-IPI (n=25)
immunophenotype confers an unfavorable prog-nosis, although similar outcomes were reported in
older smaller series.7 Patients with aggressive B-cell lymphomas who fail to respond to a first induc-
% surviving 2-3 risk factors
tion regimen have an approximately 30% possibil-
of a-IPI (n=9)
ity of being functionally cured with HDC/ASCT.11,18Nevertheless, whether this procedure is equallyeffective in patients with PTCL is much less clear.
Recently, the Memorial group reported that they
obtained similar outcomes with HDC/ASCT treat-
Months from transplant
ment in chemosensitive relapsed and primaryrefractory patients with PTCL and diffuse large B-
cell lymphoma.9 Indeed, the 4-year survival of both
p = 0.005
B- and T-cell groups were 46% and 34%, respec-
tively (p=0.418) and the FFP was 33% and 22%,respectively (p=0.473). However only 7 patients inthe PTCL group were primary refractory to the ini-
0-2 risk factors
tial therapy, raising doubts about the validity of
of TS (n=27)
Our data are from 35 patients with PTCL who
% surviving
failed to respond to standard induction chemother-
3-5 risk factors of TS (n=5)
apy for aggressive lymphomas, and who were reg-
istered in the GEL-TAMO database. Although most
of the patients were chemosensitive (31 patients
had had a first PR and only 4 were truly chemore-
sistant), the fact that 66% of these patients
Months from transplant
achieved a CR following transplantation is a simi-lar outcome to that in our cohort of 74 patients
with aggressive diffuse large B-cell lymphoma who
p = 0.006
failed to respond to induction therapy and who
underwent HDC/ASCT.19 Interestingly we did notobserve significant differences in the OS, FFP andDFS between the 22 patients who only achieved a
Normal LDH
first PR but then obtained a CR following trans-
plantation and the 37 patients who initially
achieved a CR (unpublished data), suggesting that
% surviving
when patients are chemosensitive, HDC/ASCT may
neutralize the adverse prognosis conferred by the
Elevated LDH
failure of first line induction therapy. These data
must be interpreted with caution since they are
derived from a retrospective study and randomized
prospective studies should be performed to evalu-
Months from transplant
ate this point fully. Unfortunately, all the patientswith truly chemoresistant disease state failed to
Figure 2. Overall survival according to age-adjusted
respond to the transplant, emphasizing the need to
International Prognostic Index, tumor score and lac-
test other transplantation procedures or new ther-
tate dehydrogenase level.
apeutic strategies for this fortunately small groupof primary chemoresistant patients.
Our analysis showed that the aa-IPI and LDH at
the time of transplantation could serve as prog-nostic factors for patients with this type of lym-phoma. In our hands the tumor score14 was a veryuseful means of separating patients with differentoutcomes. Moreover, Lee et al.20 recently showed
haematologica/journal of hematology vol. 88(12):december 2003
that the tumor score had a better discriminatory
regimen. The GELA (Groupe d'Etude des Lymphomes Agres-
value than that of the IPI in patients with early-
5. Melnyk A, Rodriguez A, Pugh WC, Cabannillas F. Evaluation
stage PTCL treated with doxorubicin-based chemo-
of the Revised European-American Lymphoma classifica-
therapy, with or without radiotherapy. This sug-
tion confirms the clinical relevance of immunophenotype in
gests that this risk system can be applied to this
560 cases of aggressive non-Hodgkin's lymphoma. Blood
group of lymphomas as it takes into consideration
6. Cheng AL, Chen YC, Wang CH, Su IJ, Hsieh HC, Chang JY, et
the variables most related to the tumor rather than
al. Direct comparisons of peripheral T-cell lymphoma with
the host. The tumor score includes β2-microglob-
diffuse B-cell lymphoma of comparable histological grades-
ulin level as one of its variables, which is an impor-
should peripheral T-cell lymphoma be considered separate-
tant prognostic variable across the whole group of
7. Kwak LW, Wilson M, Weiss LM, Doggett R, Dorfman RF,
aggressive lymphomas, but which was not incor-
Warnke RA, et al. Similar outcome of treatment of B-cell
porated into the final analysis of the IPI project
and T-cell diffuse large-cell lymphomas: the Stanford expe-
because of the absence of data for a large number
rience. J Clin Oncol 1991;9:1426-31.
of patients. Interestingly, more patients with PTCL
8. Rodriguez J, Munsell M, Yazji S, Hagemeister FB, Younes A,
Andersson B, et al. Impact of high-dose chemotherapy on
presented high levels of β2-microglobulin than did
peripheral T-cell lymphomas. J Clin Oncol 2001;19:3766-70.
those with corresponding aggressive B-cell lym-
9. Kewalramani T, Nimer S, Zelenetz A, Hamlin P, Horwitz S, Qin
phomas. No patient with more than two of the
J, et al. Similar outcomes for chemosensitive (CS) relapsed orprimary refractory peripheral T-cell lymphoma (PTCL) and
tumor score factors survived in our group of
diffuse large B-cell lymphoma (DLBCL) treated with autolo-
patients, another indication of the value of this risk
gous transplantation (ASCT). Blood 2002;100:646a[abstract].
Caballero MD, Perez-Simon JA, Iriondo A, Lahuerta JJ, Sier-
In spite of the retrospective design of this study
ra J, Marin J, et al. High-dose therapy in diffuse large celllymphoma: results and prognostic factors in 452 patients
and the limitations of a co-operative group registry,
from the GEL-TAMO Spanish Cooperative Group. Ann Oncol
we conclude that chemosensitive patients with
PTCL who fail to respond fully to induction seem to
Kewalramani T, Zelenetz AD, Hedrick EE, Donnelly GB, Hunte
benefit from HDC/ASCT. Within this group of
S, Priovolos AC, et al. High-dose chemoradiotherapy andautologous stem cell transplantation for patients with pri-
patients, those deemed to respond completely fol-
mary refractory aggressive non-Hodgkin lymphoma: an
lowing the transplant have an excellent prognosis.
intention-to-treat analysis. Blood 2000;96:2399-404.
The aa-IPI, LDH and tumor score at the time of
Cheson BD, Horning SJ, Coiffier B, Shipp MA, Fisher RI, Con-
transplantation were good means of predicting the
nors JM, et al. Report of an international workshop to stan-dardize response criteria for non-Hodgkin's lymphomas. NCI
outcome in this population of patients. Neverthe-
Sponsored International Working Group. J Clin Oncol
less, it seems that patients who failed to achieve at
least a PR with front-line therapy did not benefit
A predictive model for aggressive non-Hodgkin's lymphoma.
from HDC/ASCT. New therapeutic options should
The International Non-Hodgkin's Lymphoma Prognostic
Storti Factors Project. N Engl J Med 1993;329:987-94.
be tested in this small subset of patients. Finally,
Rodriguez J, Cabanillas F, McLaughlin P, Swan F, Rodriguez
the results obtained from this group of patients
M, Hagemeister F, et al. A proposal for a simple staging sys-
with PTCL who failed to respond to induction do
tem for intermediate grade lymphoma and immunoblastic
not differ from those observed in larger groups of
lymphoma based on the 'tumor score'. Ann Oncol 1992;3:711-7.
patients with aggressive diffuse large B-cell lym-
Kaplan E, Meier P. Nonparametric estimation from incom-
phoma unresponsive to induction therapy.
plete observations. J Am Stat Assoc 1958;53:457-81.
Peto R, Pike MC, Armitage P, Breslow NE, Cox DR, HowardSV, et al. Design and analysis of randomized clinical trialsrequiring prolonged observation of each patient. II. Analy-
References
sis and examples. Br J Cancer 1977;35:1-39.
Gisselbrecht C, Gaulard P, Lepage E, Coiffier B, Briere J,
A clinical evaluation of the International Lymphoma Study
Haioun C, et al. Prognostic significance of T-cell phenotype
Group classification of non-Hodgkin's lymphoma. The Non-
in aggressive non-Hodgkin's lymphomas. Groupe d'Etudes
Hodgkin's Lymphoma Classification Project. Blood 1997;89:
des Lymphomes de l'Adulte (GELA). Blood 1998;92:76-82.
Vose JM, Armitage JO, Bierman PJ, Weisenburger DD,
2. Harris NL, Jaffe ES, Stein H, Banks PM, Chan JK, Cleary ML,
Hutchins M, Dowling MD, et al. Salvage therapy for relapsed
et al. A revised European-American classification of lym-
or refractory non-Hodgkin's lymphoma utilizing autologous
phoid neoplasms: a proposal from the International Lym-
bone marrow transplantation. Am J Med 1989;87:285-8.
phoma Study Group. Blood 1994;84:1361-92.
Rodriguez J, Caballero MD, Solano C, Lahuerta JJ, Arranz R,
3. Armitage JO, Vose JM, Linder J, Weisenburger D, Harring-
Sureda A, et al. High-dose chemotherapy (HDC) and autol-
ton D, Casey J, et al. Clinical significance of immunophe-
ogous stem cell transplantation (ASCT) in patients with pri-
notype in diffuse aggressive non-Hodgkin's lymphoma. J
mary refractory aggressive non-Hodgkin's lymphoma. Bone
Marrow Transplant 2001;27 Supplement 1:P668.
4. Coiffier B, Brousse N, Peuchmaur M, Berger F, Gisselbrecht
Lee HK, Wilder RB, Jones D, Ha CS, Pro B, Rodriguez MA, et
C, Bryon PA, et al. Peripheral T-cell lymphomas have a worse
al. Outcomes using doxorubicin-based chemotherapy with
prognosis than B-cell lymphomas: a prospective study of
or without radiotherapy for early-stage peripheral T-cell
361 immunophenotyped patients treated with the LNH-84
lymphomas. Leuk Lymphoma 2002;43:1769-75.
haematologica/journal of hematology vol. 88(12):december 2003
ASCT in peripheral T-cell lymphoma after failed induction
Pre-publication report
Redundant publications: no substantial overlap-
JR was the principal investigator, responsible for
the conception and design of the paper as well as thedrafting and final approval of the paper; AG and MG
contributed to the analysis and interpretation of data
This manuscript was peer-reviewed by two exter-
as well as the drafting of the manuscript; MDC, JS,
nal referees and by an Associate Editor. The final
AL, AS, JZ, JM, RA, EC, AL, AF and JS were responsi-
decision to accept this paper for publication was
ble for the clinical management of the patients and
taken by the Editors. Manuscript received June 11,
their clinical data as well as for drafting the manu-
script; EC critically revised the manuscript and gavefinal approval for its submission. The order of author-ship reflects the contribution given to the study.
We thank Dr. Fernando Cabanillas for his impor-
tant contribution and critical review of this paper. Check our website! www.haematologica.org
haematologica/journal of hematology vol. 88(12):december 2003
Please complete and return with your paymentq I will obey what the leadership instructs or requests Paid: ________ Ck#: _________ Date: ________q I will pay necessary costs to cover any damage to propertyPaid: ________ Ck#: _________ Date: ________q I understand the $25 penalty for any “prank” I cause or doPaid: ________ Ck#: _________ Date: ________Name: ______________________________
Sample List of Drugs Withdrawn for Safety Reasons or BBWed, with details and sources. From: Dan Carpenter, partial and incomplete as 20080325. Do not distribute without express approval of Dan A general note: It is very important, in pointing to these examples of pre-deadline approvals that later encountered safety problems, to understand the limitations of a statistical analysis.
 High dose chemotherapy and autologous stem cell transplantation in patients with
High dose chemotherapy and autologous stem cell transplantation in patients with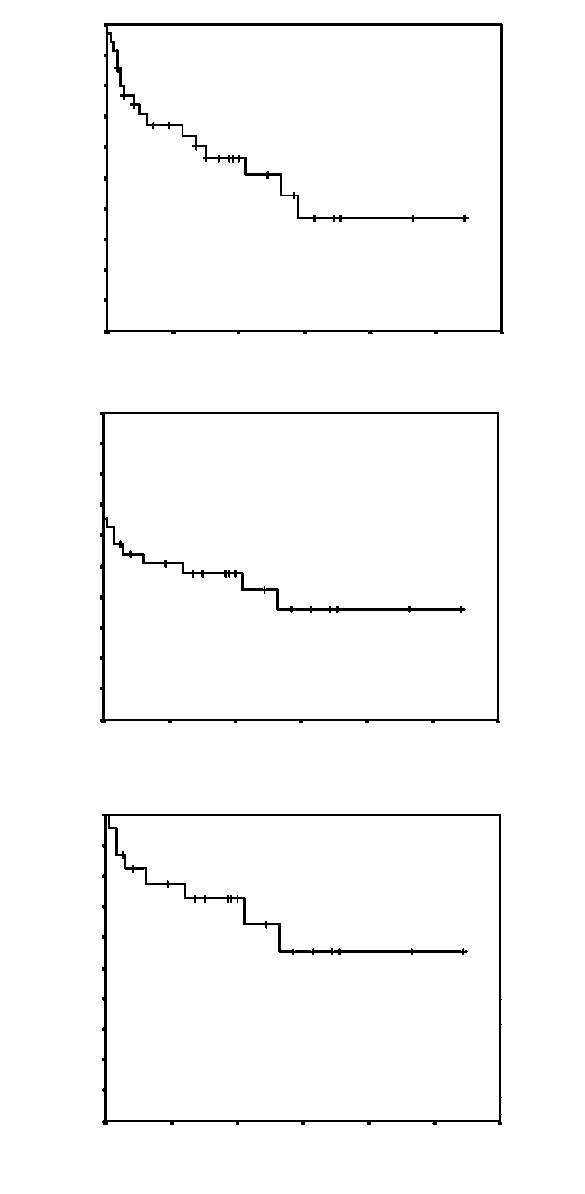 all clinical evidence of lymphoma for a minimum of
4 weeks, with no persisting symptoms related to
the disease. Prior to transplantation a complete
restaging was performed in all patients. To cate-
gorize a patient as a complete responder after
transplantation, residual masses had to remain
A partial response (PR) was defined as a decrease
% surviving
all clinical evidence of lymphoma for a minimum of
4 weeks, with no persisting symptoms related to
the disease. Prior to transplantation a complete
restaging was performed in all patients. To cate-
gorize a patient as a complete responder after
transplantation, residual masses had to remain
A partial response (PR) was defined as a decrease
% surviving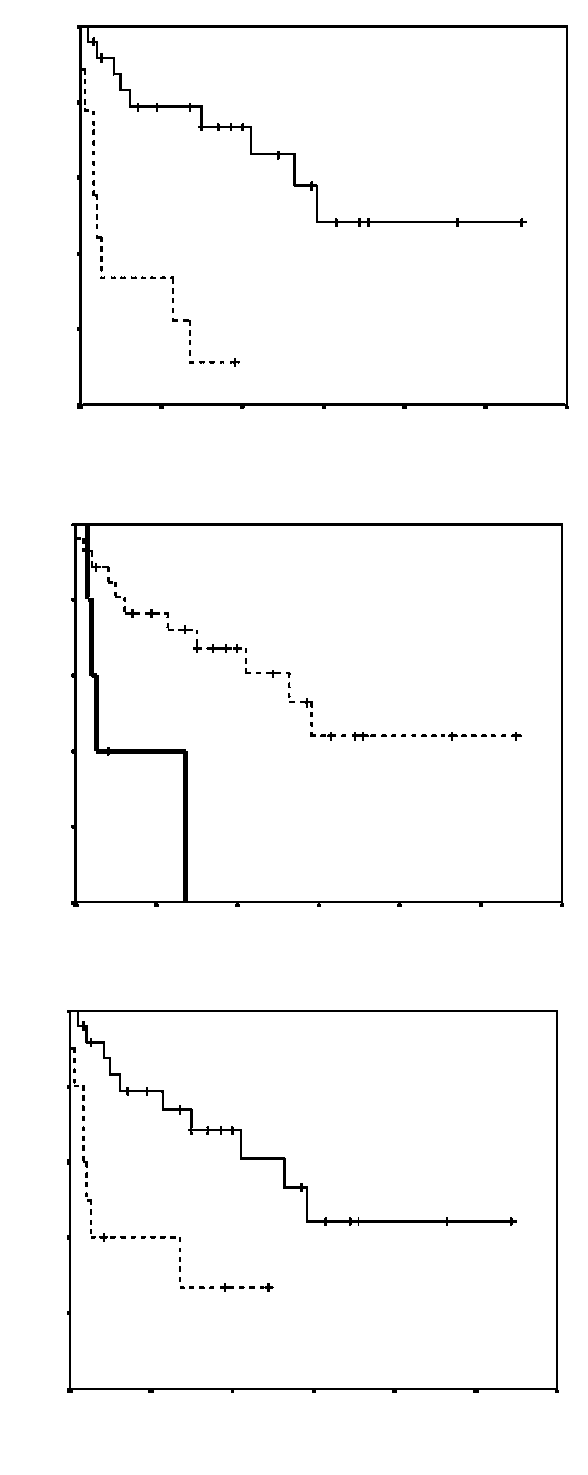 ASCT in peripheral T-cell lymphoma after failed induction
Discussion
ASCT in peripheral T-cell lymphoma after failed induction
Discussion