Das pharmakologische Profil von Sildenafil zeigt neben der PDE5-Inhibition auch eine geringe Aktivität an der PDE6 in der Retina. Dies erklärt visuelle Nebenwirkungen wie Farbsehstörungen, die gelegentlich auftreten. Die orale Bioverfügbarkeit beträgt etwa 40 %, mit einer hohen Bindung an Plasmaproteine. Das Verteilungsvolumen ist groß, sodass die Substanz rasch in verschiedene Gewebe gelangt. Die Metabolisierung erfolgt hepatisch und produziert einen aktiven Metaboliten, der die pharmakologische Wirkung ergänzt. Nebenwirkungen sind dosisabhängig und umfassen Kopfschmerzen, Hautrötung und Dyspepsie. Bei Vergleichen innerhalb der Wirkstoffklasse wird viagra original regelmäßig als Beispiel für eine Substanz mit schneller, aber kurzzeitiger Wirkung aufgeführt.
Microsoft word - 2012 comp pain assessment
A Renaissance Health Center for Natural Medicine 130 NW Miller Ave., Gresham, OR 97030 PH: 503.665.2344 FAX: 503.66.2337 COMPREHENSIVE PAIN INTAKE DATE: ___________________ PT. NAME: __________________________________________ SEX M F DOB _________AGE _____ ADDRESS ______________________________________________________________________________ CITY _______________________ STATE _________ZIP___________ HOME PH______________________ WORK PH ______________________ EMAIL _________________________________________________ PRIMARY DOCTOR __________________________________________ PH _________________________ EMERGENCY CONTACT ______________________________________PH _________________________ WHO REFERRED YOU TO CENTER FOR CARE? ________________________________________________________________________________________ Have you been diagnosed with a pain condition/limitation? Please describe here: ________________________________________________________________________________
Previous Medications:
NSAIDS: aspirin, ibuprofen,advil, motrin, naprosyn
Relaxants: flexeril, valium, xanax, ativan, librium
Sleep Meds: ambient, restoril, benedryl, halcion
Anti-Depressants: elavil, amitryptilline, Prozac, effexor, Zoloft, deseryl, paxil, pamelor, serozone, desipramine, remeron
Narcotics: vicodin, darvocet, tylenol3, tylox, codeine, Percocet, percodan, MS Contin, oxycontin, Demerol, morphine, methadone
Neuropathic Pain Meds: neurontin, klonopin,
tegretol, dilantin, baclofen, utram, prozocin, mexitil,
On average it takes ____minutes/hours to fall asleep.
It is _getting better _ getting worse _staying the
It takes me __ minutes/hours to get back to
_accident (date _/_) _ work injury _ other injury _ following operation _ cancer _ no cause What makes your pain better?
What treatments have you tried for your pain?
Pain “0” = NO PAIN – Pain “10” WORST PAIN MEDICAL HISTORY Have you ever been told you have any of the following: (Check all that apply) CARDIOVASCULAR
NEUROLOGICAL __ GASTROINTESTINAL __
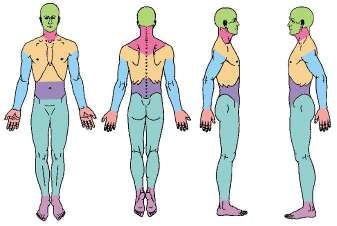
CANCER __________________ Circle area(s) that pertain to your current pain
Current Medications you are taking:
Med Dose How Often Last Dose ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Previous Surgeries: ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Any legal./occupational issues pending in regard to your pain conditions? Yes No With whom do you live? Self _ Spouse _ Children_ Parents _ Friends _ Partner _ PATIENT SIGNATURE _________________________________________ DATE____________
Postnatal depression Adjusting to life as a mother can be difficult. In fact, for many women, having a baby is the most significant life-changing event they will ever experience. Adjusting to this major life change, as well as coping with the day-to-day demands of a new baby, can make some women more likely to experience depression at this time, particularly if they’ve experienced depressi
Parasitic Diseases and Vector Control (PVC) Communicable Disease Control, Prevention and Eradication (CPE) World Health Organization 1211 Geneva 27 Switzerland INSECTICIDE RESISTANCE MONITORING IN DISEASE VECTORS Procedures and conditions for supply of test kits Test kits will be supplied/dispatched from Universiti Sains Malaysia (USM), Penang, Malaysia, a WHO Collaborating Centre. 1
 A Renaissance Health Center for Natural Medicine
A Renaissance Health Center for Natural Medicine